Anatomy, Biomechanics and Regional Interdependence of the Thorax: Difference between revisions
No edit summary |
No edit summary |
||
| (11 intermediate revisions by 5 users not shown) | |||
| Line 3: | Line 3: | ||
[[Category:Course Pages]] | [[Category:Course Pages]] | ||
[[Category: | [[Category:Plus Content]] | ||
[[Category:Thoracic Spine]] | [[Category:Thoracic Spine]] | ||
[[Category:Musculoskeletal/Orthopaedics]] | [[Category:Musculoskeletal/Orthopaedics]] | ||
== Introduction == | == Introduction == | ||
The thorax is an area of the spine that has, historically, been under-explored. It can, however, be a silent contributor to many presentations in clinical practice.<ref name=":0" /> | The [[Thoracic Anatomy|thorax]] is an area of the spine that has, historically, been under-explored. It can, however, be a silent contributor to many presentations in clinical practice.<ref name=":0" /> | ||
One cross-sectional survey in Denmark | One cross-sectional survey in Denmark<ref name=":4">Leboeuf-Yde C, Nielsen J, Kyvik KO, Fejer R, Hartvigsen J. [https://link.springer.com/article/10.1186/1471-2474-10-39 Pain in the lumbar, thoracic or cervical regions: do age and gender matter? A population-based study of 34,902 Danish twins 20–71 years of age]. ''BMC Musculoskelet Disord''. 2009;10(39).</ref> looked at the prevalence of spinal pain. It found that in one year<ref name=":4" />: | ||
* 13 percent of respondents had thoracic pain | * 13 percent of respondents had [[Thoracic Back Pain|thoracic pain]] | ||
* 43 percent had low back pain | * 43 percent had [[Low Back Pain|low back pain]] | ||
* 44 percent had neck pain | * 44 percent had [[Mechanical Neck Pain|neck pain]] | ||
However, between 36 to 41 percent of individuals who present with neck or back pain will also have thoracic pain (i.e. around 4 in 10 patients).<ref>Roquelaure Y, Bodin J, Ha C, Le Marec F, Fouquet N, Ramond-Roquin A et al. Incidence and risk factors for thoracic spine pain in the working population: the French Pays de la Loire study. Arthritis Care Res (Hoboken). 2014;66(11):1695-702. </ref> This is, therefore, a region that should not be ignored in physiotherapy practice.<ref name=":0">Bell-Jenje T. The Thorax Simplified - Anatomy, Biomechanics and Regional Interdependence Course. | However, between 36 to 41 percent of individuals who present with neck or back pain will also have thoracic pain (i.e. around 4 in 10 patients).<ref>Roquelaure Y, Bodin J, Ha C, Le Marec F, Fouquet N, Ramond-Roquin A et al. [https://onlinelibrary.wiley.com/doi/10.1002/acr.22323 Incidence and risk factors for thoracic spine pain in the working population: the French Pays de la Loire study]. Arthritis Care Res (Hoboken). 2014;66(11):1695-702. </ref> This is, therefore, a region that should not be ignored in physiotherapy practice.<ref name=":0">Bell-Jenje T. The Thorax Simplified - Anatomy, Biomechanics and Regional Interdependence Course. Plus , 2021.</ref> | ||
== Anatomy == | == Anatomy == | ||
There are 136 joints in the [[Thoracic Anatomy|thoracic spine]] and 112 muscle attachments. The orientation of the thoracic joints and ribs limit flexion, extension and lateral flexion, but facilitate rotation.<ref name=":0" /> | There are 136 joints in the [[Thoracic Anatomy|thoracic spine]] and 112 [[muscle]] attachments. The orientation of the thoracic joints and ribs limit flexion, extension and lateral flexion, but facilitate rotation.<ref name=":0" /> | ||
{{#ev:youtube|3mniZ_zQuRE}}<ref>Kenhub - Learn Human Anatomy. Thoracic Spine - Definition & Components - Human Anatomy | Kenhub. Available from: https://www.youtube.com/watch?v=3mniZ_zQuRE [last accessed 28/8/2021]</ref> | {{#ev:youtube|3mniZ_zQuRE}}<ref>Kenhub - Learn Human Anatomy. Thoracic Spine - Definition & Components - Human Anatomy | Kenhub. Available from: https://www.youtube.com/watch?v=3mniZ_zQuRE [last accessed 28/8/2021]</ref> | ||
=== Range of Motion === | === Range of Motion === | ||
The total rotation available in the thoracic spine is 85 degrees (+/- 14.8 degrees).<ref>Heneghan NR, Hall A, Hollands M, Balanos GM. Stability and intra-tester reliability of an in vivo measurement of thoracic axial rotation using an innovative methodology. Manual Therapy. 2009; 14(4):452-5.</ref> It contributes 80 percent of the total range of axial trunk rotation.<ref>Fujii R, Sakaura H, Mukai Y, Hosono N, Ishii T, Iwasaki M et al. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2223353/ Kinematics of the lumbar spine in trunk rotation: in vivo three-dimensional analysis using magnetic resonance imaging]. ''Eur Spine J''. 2007;16(11):1867-74. </ref> Each thoracic segment rotates between 6 and 8 degrees. This is significantly more than the lumbar segments, which only rotate 2 to 3 degrees.<ref name=":3">Lee LJ. A closer look at the thorax [Internet. Physical Therapy Web [cited 30 August 2021]. Available from: https://physicaltherapyweb.com/closer-look-thorax-lj-lee/</ref> | The total rotation available in the thoracic spine is 85 degrees (+/- 14.8 degrees).<ref>Heneghan NR, Hall A, Hollands M, Balanos GM. Stability and intra-tester reliability of an in vivo measurement of thoracic axial rotation using an innovative methodology. Manual Therapy. 2009; 14(4):452-5.</ref> It contributes 80 percent of the total range of axial trunk rotation.<ref>Fujii R, Sakaura H, Mukai Y, Hosono N, Ishii T, Iwasaki M et al. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2223353/ Kinematics of the lumbar spine in trunk rotation: in vivo three-dimensional analysis using magnetic resonance imaging]. ''Eur Spine J''. 2007;16(11):1867-74. </ref> Each thoracic segment rotates between 6 and 8 degrees. This is significantly more than the [[Lumbar Anatomy|lumbar segments]], which only rotate 2 to 3 degrees.<ref name=":3">Lee LJ. A closer look at the thorax [Internet. Physical Therapy Web [cited 30 August 2021]. Available from: https://physicaltherapyweb.com/closer-look-thorax-lj-lee/</ref> | ||
Thoracic movement is critical for optimal performance in rotational sports and the thoracic spine kinematically links the upper and lower quarters.<ref>Heneghan NR, Lokhaug SM, Tyros I, Longvastøl S, Rushton A. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7173996/ Clinical reasoning framework for thoracic spine exercise prescription in sport: a systematic review and narrative synthesis]. BMJ Open Sport Exerc Med. 2020;6(1):e000713. </ref><ref>Heneghan NR. Webb K, Mahoney T, Rushton A. [https://www.researchgate.net/publication/334720891_Thoracic_spine_mobility_an_essential_link_in_upper_limb_kinetic_chains_in_athletes_A_systematic_review Thoracic spine mobility, an essential link in upper limb kinetic chains in athletes: A systematic review]. ''Transl Sports Med''. 2019;2:301-15.</ref> It also contributes 55 percent of the total force during a throw.<ref>Kaczmarek PK, Lubiatowski P, Cisowski P, Grygorowicz M, Łepski M, Długosz J et al. [https://www.researchgate.net/publication/263207986_Shoulder_problems_in_overhead_sports_Part_I_-_biomechanics_of_throwing Shoulder problems in overhead sports. Part I - biomechanics of throwing]. Pol Orthop Traumatol. 2014;79:50-8. </ref> | Thoracic movement is critical for optimal performance in rotational sports and the thoracic spine kinematically links the upper and lower quarters.<ref>Heneghan NR, Lokhaug SM, Tyros I, Longvastøl S, Rushton A. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7173996/ Clinical reasoning framework for thoracic spine exercise prescription in sport: a systematic review and narrative synthesis]. BMJ Open Sport Exerc Med. 2020;6(1):e000713. </ref><ref>Heneghan NR. Webb K, Mahoney T, Rushton A. [https://www.researchgate.net/publication/334720891_Thoracic_spine_mobility_an_essential_link_in_upper_limb_kinetic_chains_in_athletes_A_systematic_review Thoracic spine mobility, an essential link in upper limb kinetic chains in athletes: A systematic review]. ''Transl Sports Med''. 2019;2:301-15.</ref> It also contributes 55 percent of the total force during a throw.<ref>Kaczmarek PK, Lubiatowski P, Cisowski P, Grygorowicz M, Łepski M, Długosz J et al. [https://www.researchgate.net/publication/263207986_Shoulder_problems_in_overhead_sports_Part_I_-_biomechanics_of_throwing Shoulder problems in overhead sports. Part I - biomechanics of throwing]. Pol Orthop Traumatol. 2014;79:50-8. </ref> | ||
| Line 30: | Line 30: | ||
=== Regions of the Thorax === | === Regions of the Thorax === | ||
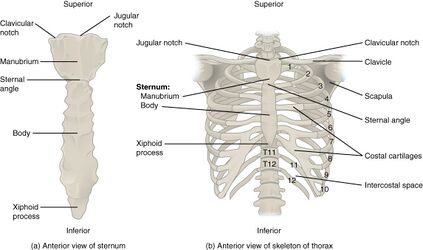
* Vertebromanubrial: | * [[File:Rib Cage.jpg|right|frameless|423x423px]]Vertebromanubrial: | ||
** Includes: T1 and T2, ribs 1 and 2, the manubrium and clavicle | ** Includes: T1 and T2, [[ribs]] 1 and 2, the manubrium and [[Clavicula|clavicle]] | ||
* Vertebrosternal | * Vertebrosternal | ||
** Includes: T3 to T7, true ribs 3 to 7 and sternum | ** Includes: T3 to T7, true ribs 3 to 7 and [[sternum]] | ||
* Vertebrochondral: | * Vertebrochondral: | ||
** Includes: T8 to T10 and false ribs 8 to 10 | ** Includes: T8 to T10 and false ribs 8 to 10 | ||
* Thoracolumbar | * Thoracolumbar | ||
** Includes: T11 and T12, floating ribs 11 and 12<ref name=":0" /> | ** Includes: T11 and T12, floating ribs 11 and 12<ref name=":0" /> | ||
NB: True ribs attach directly to the sternum via cartilage, false ribs attach to the lowest true ribs and floating ribs only have posterior attachments to the spine. | NB: True ribs attach directly to the sternum via [[cartilage]], false ribs attach to the lowest true ribs and floating ribs only have posterior attachments to the spine. | ||
==== Ribs ==== | ==== Ribs ==== | ||
* Ribs 1, 11 and 12 articulate with the named vertebra (i.e. rib 1 articulates with T1) | * Ribs 1, 11 and 12 articulate with the named vertebra (i.e. rib 1 articulates with T1) | ||
* Ribs 2 to 10 articulate with the named vertebra, as well as the body above, the intervertebral disc and the anterior surface of the transverse process of the named vertebra | * Ribs 2 to 10 articulate with the named vertebra, as well as the body above, the [[intervertebral disc]] and the anterior surface of the transverse process of the named vertebra | ||
* More information about the ribs is available [[Ribs|here]] | * More information about the ribs is available [[Ribs|here]] | ||
==== The Thoracic Ring (T3-T9) ==== | ==== The Thoracic Ring (T3-T9) ==== | ||
<blockquote>'The "thoracic ring” consists of two adjacent vertebrae and the related intervertebral disc, the right and left ribs (attached to the vertebra-disc-vertebra complex at the costovertebral joints), and the anterior attachments to the sternum/manubrium and related cartilages.'<ref name=":1">Lee LJ. Thoracic ring approach. Available from: https://ljlee.ca/teaching-models/the-thoracic-ring-approach/ (accessed 28 August 2021).</ref></blockquote>There are 13 articulations per thoracic ring | <blockquote>'The "thoracic ring” consists of two adjacent vertebrae and the related intervertebral disc, the right and left ribs (attached to the vertebra-disc-vertebra complex at the costovertebral joints), and the anterior attachments to the sternum/manubrium and related cartilages.'<ref name=":1">Lee LJ. Thoracic ring approach. Available from: https://ljlee.ca/teaching-models/the-thoracic-ring-approach/ (accessed 28 August 2021).</ref></blockquote>There are 13 articulations per thoracic ring<ref name=":0" /><ref name=":1" />: | ||
* Zygapophyseal / facet = 2 articulations | * Zygapophyseal / facet = 2 articulations | ||
| Line 59: | Line 59: | ||
== Thoracic Function == | == Thoracic Function == | ||
Lee has described the thoracic spine as a “slinky" or a "shock-absorbing spring”. | Lee<ref name=":1" /> has described the thoracic spine as a “slinky" or a "shock-absorbing spring”. It consists of a dynamic stack of 10 thoracic rings<ref name=":1" /> and has the following functions<ref name=":3" />: | ||
* Force transmission | * Force transmission | ||
** NB: many patients with chronic low back pain or cervical pain have a stiff thoracic spine and increasing thoracic mobility allows for more even distribution of load through the spine with movement<ref>McConnell J. Recalcitrant chronic low back and leg pain--a new theory and different approach to management. Man Ther. 2002;7(4):183-92. </ref> <ref>Mohanty PP, Pattnaik M. Mobilisation of the thoracic spine in the management of spondylolisthesis. J Bodyw Mov Ther. 2016;20(3):598-603. </ref><ref>Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther. 2005;10(2):127-35. </ref> | ** NB: many patients with chronic low back pain or cervical pain have a stiff thoracic spine and increasing thoracic mobility allows for more even distribution of load through the spine with movement<ref>McConnell J. Recalcitrant chronic low back and leg pain--a new theory and different approach to management. Man Ther. 2002;7(4):183-92. </ref> <ref>Mohanty PP, Pattnaik M. Mobilisation of the thoracic spine in the management of spondylolisthesis. J Bodyw Mov Ther. 2016;20(3):598-603. </ref><ref>Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther. 2005;10(2):127-35. </ref> | ||
* Central area for myofascial attachments | * Central area for [[Thoracolumbar Fascia|myofascial]] attachments | ||
* Protects heart, lungs, vessels and digestive tract<ref>Edmondston SJ, Singer KP. Thoracic spine: anatomical and biomechanical considerations for manual therapy. Man Ther. 1997;2(3):132-43. </ref> | * Protects heart, lungs, vessels and digestive tract<ref>Edmondston SJ, Singer KP. Thoracic spine: anatomical and biomechanical considerations for manual therapy. Man Ther. 1997;2(3):132-43. </ref> | ||
* Aids optimal respiratory function | * Aids optimal [[Respiratory Assessment|respiratory function]] <ref>Kudzinskas A, Callahan AL. [https://www.ncbi.nlm.nih.gov/books/NBK557710/ Anatomy, Thorax.] InStatPearls [Internet] 2021 Jul 31. StatPearls Publishing.</ref> | ||
* Houses the autonomic nervous system | * Houses the autonomic nervous system | ||
== Thoracic Asymmetry == | == Thoracic Asymmetry == | ||
It is normal for there to be thoracic asymmetry of the facet orientation in the thoracic spine.<ref>Masharawi Y, Rothschild B, Dar G, Peleg S, Robinson D, Been E et al. Facet orientation in the thoracolumbar spine: three-dimensional anatomic and biomechanical analysis. Spine (Phila Pa 1976). 2004;29(16):1755-63.</ref> Asymmetrical anatomy may, however, cause changes in the coupled motion at a segment.<ref>Andriacchi T, Schultz A, Belytschko T, Galante J. A model for studies of mechanical interactions between the human spine and rib cage. J Biomech. 1974;7(6):497–507.</ref> | It is normal for there to be thoracic asymmetry of the [[Facet Joints|facet]] orientation in the thoracic spine.<ref>Masharawi Y, Rothschild B, Dar G, Peleg S, Robinson D, Been E et al. Facet orientation in the thoracolumbar spine: three-dimensional anatomic and biomechanical analysis. Spine (Phila Pa 1976). 2004;29(16):1755-63.</ref> Asymmetrical anatomy may, however, cause changes in the coupled motion at a segment.<ref>Andriacchi T, Schultz A, Belytschko T, Galante J. A model for studies of mechanical interactions between the human spine and rib cage. J Biomech. 1974;7(6):497–507.</ref> | ||
== Regional Interdependence == | == Regional Interdependence == | ||
| Line 77: | Line 77: | ||
=== 1. Cervical spine === | === 1. Cervical spine === | ||
Tsang and colleagues found that | Tsang and colleagues<ref name=":2" /> found that motion of the thoracic spine, particularly the upper thoracic spine, contributes to neck mobility. The upper thoracic spine contributes:<ref name=":2">Tsang SM, Szeto GP, Lee RY. Normal kinematics of the neck: the interplay between the cervical and thoracic spines. Man Ther. 2013;18(5):431-7. </ref> | ||
* 25 percent to cervical flexion and extension | * 25 percent to cervical flexion and extension | ||
| Line 87: | Line 87: | ||
=== 2. Shoulder === | === 2. Shoulder === | ||
The scapula is a sesamoid bone, which rests upon the thorax. It is influenced by the position of the thoracic spine elements and the ribs. | The [[scapula]] is a sesamoid [[bone]], which rests upon the thorax. It is influenced by the position of the thoracic spine elements and the ribs. [[Posture]]<nowiki/>s such as [[Thoracic Hyperkyphosis|thoracic kyphosis]], thoracic [[scoliosis]] or flattened / inverted thoracic spine, can change the resting position of the scapula.<ref name=":0" /> | ||
* Thoracic kyphosis is associated with a loss of glenohumeral range of motion and impingement symptoms<ref>Barrett E, O'Keeffe M, O'Sullivan K, Lewis J, McCreesh K. Is thoracic spine posture associated with shoulder pain, range of motion and function? A systematic review. Man Ther. 2016;26:38-46. </ref> | * Thoracic kyphosis is associated with a loss of [[Glenohumeral Joint|glenohumeral]] range of motion and [[Impingement / Instability Differentiation|impingement]] symptoms<ref>Barrett E, O'Keeffe M, O'Sullivan K, Lewis J, McCreesh K. Is thoracic spine posture associated with shoulder pain, range of motion and function? A systematic review. Man Ther. 2016;26:38-46. </ref> | ||
* Treating the thoracic spine has been shown to alter shoulder symptoms<ref>Strunce JB, Walker MJ, Boyles RE, Young BA. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2813499/ The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain]. J Man Manip Ther. 2009;17(4):230-6.</ref><ref>Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH et al. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009;14(4):375-80.</ref> <ref>Haider R, Bashir MS, Adeel M, Ijaz MJ, Ayub A. [https://jpma.org.pk/article-details/8600?article_id=8600 Comparison of conservative exercise therapy with and without Maitland Thoracic Manipulative therapy in patients with subacromial pain: Clinical trial]. J Pak Med Assoc. 2018 Mar;68(3):381-7. </ref> | * Treating the thoracic spine has been shown to alter shoulder symptoms<ref>Strunce JB, Walker MJ, Boyles RE, Young BA. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2813499/ The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain]. J Man Manip Ther. 2009;17(4):230-6.</ref><ref>Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH et al. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009;14(4):375-80.</ref> <ref>Haider R, Bashir MS, Adeel M, Ijaz MJ, Ayub A. [https://jpma.org.pk/article-details/8600?article_id=8600 Comparison of conservative exercise therapy with and without Maitland Thoracic Manipulative therapy in patients with subacromial pain: Clinical trial]. J Pak Med Assoc. 2018 Mar;68(3):381-7. </ref> | ||
=== 3. Other Relationships === | === 3. Other Relationships === | ||
* Sympathetic nerve blocks at the thoracic spine can improve chronic upper extremity neuropathic pain<ref>Yoo HS, Nahm FS, Lee PB, Lee CJ. Early thoracic sympathetic block improves the treatment effect for upper extremity neuropathic pain. Anesth Analg. 2011;113(3):605-9. </ref> | * [[Sympathetic Nervous System|Sympathetic]] nerve blocks at the thoracic spine can improve chronic upper extremity [[Neuropathic Pain|neuropathic pain]]<ref>Yoo HS, Nahm FS, Lee PB, Lee CJ. Early thoracic sympathetic block improves the treatment effect for upper extremity neuropathic pain. Anesth Analg. 2011;113(3):605-9. </ref> | ||
* 70 percent of patients with lateral elbow pain have co-existing thoracic pain (compared to 16 percent of the control group)<ref>Berglund KM, Persson BH, Denison E. Prevalence of pain and dysfunction in the cervical and thoracic spine in persons with and without lateral elbow pain. Man Ther. 2008;13(4):295-9.</ref> | * 70 percent of patients with lateral [[elbow]] pain have co-existing thoracic pain (compared to 16 percent of the control group)<ref>Berglund KM, Persson BH, Denison E. Prevalence of pain and dysfunction in the cervical and thoracic spine in persons with and without lateral elbow pain. Man Ther. 2008;13(4):295-9.</ref> | ||
== Postural and Positional Implications == | == Postural and Positional Implications == | ||
Certain postural dysfunctions could result in compensatory thoracic dysfunction (i.e. ‘gives’):<ref name=":0" /> | Certain postural dysfunctions could result in compensatory thoracic dysfunction (i.e. ‘gives’):<ref name=":0" /> | ||
* Inextensible | * Inextensible [[Hamstrings|hamstring]]<nowiki/>s force the thoracic spine to 'give' into flexion during stride, lunging and long sitting | ||
* Inextensible hip flexors can cause lordosis and kyphosis | * Inextensible hip flexors can cause [[Low Back Pain Related to Hyperlordosis|lordosis]] and kyphosis | ||
* A leg length discrepancy and asymmetrical load can cause thoracic scoliosis | * A [[Leg Length Discrepancy|leg length discrepancy]] and asymmetrical load can cause thoracic scoliosis | ||
[[File:Bigstock Image - Forward Head Posture - ID302417506.jpg|thumb|Figure 1. Forward head position.|alt=|400x400px]] | [[File:Bigstock Image - Forward Head Posture - ID302417506.jpg|thumb|Figure 1. Forward head position.|alt=|400x400px]] | ||
* Forward head position (Figure 1) | |||
Poor cervico-thoracic postures such as<ref name=":0" />: | |||
* [[Forward Head Posture|Forward head position]] (Figure 1) | |||
* Thoracic kyphosis | * Thoracic kyphosis | ||
* Scoliosis | * Scoliosis | ||
* Flat / inverted thoracic spine | * [[Sway Back Posture|Flat / inverted thoracic spine]] | ||
Can cause | Can cause<ref name=":0" />: | ||
* Muscle imbalances | * Muscle imbalances | ||
* Joint incongruity | * Joint incongruity | ||
* Ligament laxity | * [[Ligament]] laxity | ||
* Altered neurodynamics | * Altered neurodynamics | ||
Thoracic scoliosis | |||
Thoracic scoliosis<ref name=":0" />: | |||
* Even minor curves cause wedging of the vertebrae and discs<ref>Stokes IA, Aronsson DD. Disc and vertebral wedging in patients with progressive scoliosis. J Spinal Disord. 2001;14(4):317-22. </ref> | * Even minor curves cause wedging of the vertebrae and discs<ref>Stokes IA, Aronsson DD. Disc and vertebral wedging in patients with progressive scoliosis. J Spinal Disord. 2001;14(4):317-22. </ref> | ||
| Line 126: | Line 130: | ||
* Potentially 40 percent of patients presenting for physiotherapy with back or neck pain will have an associated thoracic spine dysfunction which needs to be assessed and managed | * Potentially 40 percent of patients presenting for physiotherapy with back or neck pain will have an associated thoracic spine dysfunction which needs to be assessed and managed | ||
* Biomechanics and knowledge of the clinical anatomy of the thorax will help you to better understand the underlying pathogenesis of these conditions | * [[Biomechanics]] and knowledge of the clinical anatomy of the thorax will help you to better understand the underlying pathogenesis of these conditions | ||
* Thoracic rotation is essential for optimal sports performance and functional activities | * Thoracic rotation is essential for optimal sports performance and functional activities | ||
* Postural dysfunctions such as tight hamstrings or hip flexors may force compensatory 'gives' in the thoracic spine - it is essential to look for the source of the problem | * Postural dysfunctions such as tight hamstrings or hip flexors may force compensatory 'gives' in the thoracic spine - it is essential to look for the source of the problem | ||
== References == | == References == | ||
Latest revision as of 16:17, 13 January 2023
Top Contributors - Jess Bell, Lucinda hampton, Kim Jackson, Olajumoke Ogunleye, Merinda Rodseth and Robin Tacchetti
Introduction[edit | edit source]
The thorax is an area of the spine that has, historically, been under-explored. It can, however, be a silent contributor to many presentations in clinical practice.[1]
One cross-sectional survey in Denmark[2] looked at the prevalence of spinal pain. It found that in one year[2]:
- 13 percent of respondents had thoracic pain
- 43 percent had low back pain
- 44 percent had neck pain
However, between 36 to 41 percent of individuals who present with neck or back pain will also have thoracic pain (i.e. around 4 in 10 patients).[3] This is, therefore, a region that should not be ignored in physiotherapy practice.[1]
Anatomy[edit | edit source]
There are 136 joints in the thoracic spine and 112 muscle attachments. The orientation of the thoracic joints and ribs limit flexion, extension and lateral flexion, but facilitate rotation.[1]
Range of Motion[edit | edit source]
The total rotation available in the thoracic spine is 85 degrees (+/- 14.8 degrees).[5] It contributes 80 percent of the total range of axial trunk rotation.[6] Each thoracic segment rotates between 6 and 8 degrees. This is significantly more than the lumbar segments, which only rotate 2 to 3 degrees.[7]
Thoracic movement is critical for optimal performance in rotational sports and the thoracic spine kinematically links the upper and lower quarters.[8][9] It also contributes 55 percent of the total force during a throw.[10]
Regions of the Thorax[edit | edit source]
- Vertebromanubrial:
- Vertebrosternal
- Includes: T3 to T7, true ribs 3 to 7 and sternum
- Vertebrochondral:
- Includes: T8 to T10 and false ribs 8 to 10
- Thoracolumbar
- Includes: T11 and T12, floating ribs 11 and 12[1]

NB: True ribs attach directly to the sternum via cartilage, false ribs attach to the lowest true ribs and floating ribs only have posterior attachments to the spine.
Ribs[edit | edit source]
- Ribs 1, 11 and 12 articulate with the named vertebra (i.e. rib 1 articulates with T1)
- Ribs 2 to 10 articulate with the named vertebra, as well as the body above, the intervertebral disc and the anterior surface of the transverse process of the named vertebra
- More information about the ribs is available here
The Thoracic Ring (T3-T9)[edit | edit source]
'The "thoracic ring” consists of two adjacent vertebrae and the related intervertebral disc, the right and left ribs (attached to the vertebra-disc-vertebra complex at the costovertebral joints), and the anterior attachments to the sternum/manubrium and related cartilages.'[11]
There are 13 articulations per thoracic ring[1][11]:
- Zygapophyseal / facet = 2 articulations
- Costovertebral = 4 articulations
- Intervertebral = 1 articulation
- Costotransverse = 2 articulations
- Costochondral = 2 articulations
- Sternocostal = 2 articulations
Because of the strong anatomical connections between the ribs and the thoracic spine, mobilising a rib laterally will cause motion at the vertebral segments of that thoracic ring, as well as the rib on the opposite side of the body.[1]
Thoracic Function[edit | edit source]
Lee[11] has described the thoracic spine as a “slinky" or a "shock-absorbing spring”. It consists of a dynamic stack of 10 thoracic rings[11] and has the following functions[7]:
- Force transmission
- Central area for myofascial attachments
- Protects heart, lungs, vessels and digestive tract[15]
- Aids optimal respiratory function [16]
- Houses the autonomic nervous system
Thoracic Asymmetry[edit | edit source]
It is normal for there to be thoracic asymmetry of the facet orientation in the thoracic spine.[17] Asymmetrical anatomy may, however, cause changes in the coupled motion at a segment.[18]
Regional Interdependence[edit | edit source]
The regional interdependence theory proposes that: “seemingly unrelated impairments in remote anatomical regions of the body may contribute to and be associated with a patient’s primary report of symptoms.”[19] It has been proposed that there may also be central mechanisms involved in mediating regional interdependence.[20]
Examples of interdependency in the thoracic spine include the following:[1]
1. Cervical spine[edit | edit source]
Tsang and colleagues[22] found that motion of the thoracic spine, particularly the upper thoracic spine, contributes to neck mobility. The upper thoracic spine contributes:[22]
- 25 percent to cervical flexion and extension
- 10 percent to cervical rotation
Thoracic spine changes are, therefore, implicated in a loss of cervical range of motion, so this area should always be assessed in patients with neck dysfunction.[22]
Similarly, Engell and colleagues have found that when manual therapy techniques (e.g. high-velocity low-amplitude spinal manipulative therapy) are applied to the thoracic spine, forces can be transmitted to the neck.[23]
2. Shoulder[edit | edit source]
The scapula is a sesamoid bone, which rests upon the thorax. It is influenced by the position of the thoracic spine elements and the ribs. Postures such as thoracic kyphosis, thoracic scoliosis or flattened / inverted thoracic spine, can change the resting position of the scapula.[1]
- Thoracic kyphosis is associated with a loss of glenohumeral range of motion and impingement symptoms[24]
- Treating the thoracic spine has been shown to alter shoulder symptoms[25][26] [27]
3. Other Relationships[edit | edit source]
- Sympathetic nerve blocks at the thoracic spine can improve chronic upper extremity neuropathic pain[28]
- 70 percent of patients with lateral elbow pain have co-existing thoracic pain (compared to 16 percent of the control group)[29]
Postural and Positional Implications[edit | edit source]
Certain postural dysfunctions could result in compensatory thoracic dysfunction (i.e. ‘gives’):[1]
- Inextensible hamstrings force the thoracic spine to 'give' into flexion during stride, lunging and long sitting
- Inextensible hip flexors can cause lordosis and kyphosis
- A leg length discrepancy and asymmetrical load can cause thoracic scoliosis

Poor cervico-thoracic postures such as[1]:
- Forward head position (Figure 1)
- Thoracic kyphosis
- Scoliosis
- Flat / inverted thoracic spine
Can cause[1]:
- Muscle imbalances
- Joint incongruity
- Ligament laxity
- Altered neurodynamics
Thoracic scoliosis[1]:
- Even minor curves cause wedging of the vertebrae and discs[30]
- 80 percent of athletes who experience asymmetrical loading on their trunk and shoulders (e.g. javelin throwers, tennis players) have thoracic scoliosis[31]
- It could, therefore, be proposed that scoliosis provides a mechanical advantage in asymmetrical sports[1]
Summary[edit | edit source]
- Potentially 40 percent of patients presenting for physiotherapy with back or neck pain will have an associated thoracic spine dysfunction which needs to be assessed and managed
- Biomechanics and knowledge of the clinical anatomy of the thorax will help you to better understand the underlying pathogenesis of these conditions
- Thoracic rotation is essential for optimal sports performance and functional activities
- Postural dysfunctions such as tight hamstrings or hip flexors may force compensatory 'gives' in the thoracic spine - it is essential to look for the source of the problem
References[edit | edit source]
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 Bell-Jenje T. The Thorax Simplified - Anatomy, Biomechanics and Regional Interdependence Course. Plus , 2021.
- ↑ 2.0 2.1 Leboeuf-Yde C, Nielsen J, Kyvik KO, Fejer R, Hartvigsen J. Pain in the lumbar, thoracic or cervical regions: do age and gender matter? A population-based study of 34,902 Danish twins 20–71 years of age. BMC Musculoskelet Disord. 2009;10(39).
- ↑ Roquelaure Y, Bodin J, Ha C, Le Marec F, Fouquet N, Ramond-Roquin A et al. Incidence and risk factors for thoracic spine pain in the working population: the French Pays de la Loire study. Arthritis Care Res (Hoboken). 2014;66(11):1695-702.
- ↑ Kenhub - Learn Human Anatomy. Thoracic Spine - Definition & Components - Human Anatomy | Kenhub. Available from: https://www.youtube.com/watch?v=3mniZ_zQuRE [last accessed 28/8/2021]
- ↑ Heneghan NR, Hall A, Hollands M, Balanos GM. Stability and intra-tester reliability of an in vivo measurement of thoracic axial rotation using an innovative methodology. Manual Therapy. 2009; 14(4):452-5.
- ↑ Fujii R, Sakaura H, Mukai Y, Hosono N, Ishii T, Iwasaki M et al. Kinematics of the lumbar spine in trunk rotation: in vivo three-dimensional analysis using magnetic resonance imaging. Eur Spine J. 2007;16(11):1867-74.
- ↑ 7.0 7.1 Lee LJ. A closer look at the thorax [Internet. Physical Therapy Web [cited 30 August 2021]. Available from: https://physicaltherapyweb.com/closer-look-thorax-lj-lee/
- ↑ Heneghan NR, Lokhaug SM, Tyros I, Longvastøl S, Rushton A. Clinical reasoning framework for thoracic spine exercise prescription in sport: a systematic review and narrative synthesis. BMJ Open Sport Exerc Med. 2020;6(1):e000713.
- ↑ Heneghan NR. Webb K, Mahoney T, Rushton A. Thoracic spine mobility, an essential link in upper limb kinetic chains in athletes: A systematic review. Transl Sports Med. 2019;2:301-15.
- ↑ Kaczmarek PK, Lubiatowski P, Cisowski P, Grygorowicz M, Łepski M, Długosz J et al. Shoulder problems in overhead sports. Part I - biomechanics of throwing. Pol Orthop Traumatol. 2014;79:50-8.
- ↑ 11.0 11.1 11.2 11.3 Lee LJ. Thoracic ring approach. Available from: https://ljlee.ca/teaching-models/the-thoracic-ring-approach/ (accessed 28 August 2021).
- ↑ McConnell J. Recalcitrant chronic low back and leg pain--a new theory and different approach to management. Man Ther. 2002;7(4):183-92.
- ↑ Mohanty PP, Pattnaik M. Mobilisation of the thoracic spine in the management of spondylolisthesis. J Bodyw Mov Ther. 2016;20(3):598-603.
- ↑ Cleland JA, Childs JD, McRae M, Palmer JA, Stowell T. Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial. Man Ther. 2005;10(2):127-35.
- ↑ Edmondston SJ, Singer KP. Thoracic spine: anatomical and biomechanical considerations for manual therapy. Man Ther. 1997;2(3):132-43.
- ↑ Kudzinskas A, Callahan AL. Anatomy, Thorax. InStatPearls [Internet] 2021 Jul 31. StatPearls Publishing.
- ↑ Masharawi Y, Rothschild B, Dar G, Peleg S, Robinson D, Been E et al. Facet orientation in the thoracolumbar spine: three-dimensional anatomic and biomechanical analysis. Spine (Phila Pa 1976). 2004;29(16):1755-63.
- ↑ Andriacchi T, Schultz A, Belytschko T, Galante J. A model for studies of mechanical interactions between the human spine and rib cage. J Biomech. 1974;7(6):497–507.
- ↑ Sueki DG, Cleland JA, Wainner RS. A regional interdependence model of musculoskeletal dysfunction: research, mechanisms, and clinical implications. J Man Manip Ther. 2013;21(2):90-102.
- ↑ Ghamkhar L, Arab AM, Nourbakhsh MR, Kahlaee AH, Zolfaghari R. Examination of regional interdependence theory in chronic neck pain: interpretations from correlation of strength measures in cervical and pain-free regions. Pain Med. 2020;21(2):e182-e190.
- ↑ FoundationPT. The truth about aches and pains - Regional Interdependence Overview. Available from: https://www.youtube.com/watch?v=v4YXQgamW2Q [last accessed 28/8/2021]
- ↑ 22.0 22.1 22.2 Tsang SM, Szeto GP, Lee RY. Normal kinematics of the neck: the interplay between the cervical and thoracic spines. Man Ther. 2013;18(5):431-7.
- ↑ Engell S, Triano JJ, Howarth SJ. Force transmission between thoracic and cervical segments of the spine during prone-lying high-velocity low-amplitude spinal manipulation: A proof of principle for the concept of regional interdependence. Clin Biomech (Bristol, Avon). 2019;69:58-63.
- ↑ Barrett E, O'Keeffe M, O'Sullivan K, Lewis J, McCreesh K. Is thoracic spine posture associated with shoulder pain, range of motion and function? A systematic review. Man Ther. 2016;26:38-46.
- ↑ Strunce JB, Walker MJ, Boyles RE, Young BA. The immediate effects of thoracic spine and rib manipulation on subjects with primary complaints of shoulder pain. J Man Manip Ther. 2009;17(4):230-6.
- ↑ Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH et al. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009;14(4):375-80.
- ↑ Haider R, Bashir MS, Adeel M, Ijaz MJ, Ayub A. Comparison of conservative exercise therapy with and without Maitland Thoracic Manipulative therapy in patients with subacromial pain: Clinical trial. J Pak Med Assoc. 2018 Mar;68(3):381-7.
- ↑ Yoo HS, Nahm FS, Lee PB, Lee CJ. Early thoracic sympathetic block improves the treatment effect for upper extremity neuropathic pain. Anesth Analg. 2011;113(3):605-9.
- ↑ Berglund KM, Persson BH, Denison E. Prevalence of pain and dysfunction in the cervical and thoracic spine in persons with and without lateral elbow pain. Man Ther. 2008;13(4):295-9.
- ↑ Stokes IA, Aronsson DD. Disc and vertebral wedging in patients with progressive scoliosis. J Spinal Disord. 2001;14(4):317-22.
- ↑ Swärd L. The thoracolumbar spine in young elite athletes. Current concepts on the effects of physical training. Sports Med. 1992;13(5):357-64.

