Axillary Nerve Injury: Difference between revisions
Leana Louw (talk | contribs) No edit summary |
No edit summary |
||
| Line 6: | Line 6: | ||
== '''Definition/Description''' == | == '''Definition/Description''' == | ||
Axillary nerve injury is characterised by trauma to the axillary nerve: from either a compressive force or a traction injury following anterior dislocation of the shoulder. | Axillary nerve injury is characterised by trauma to the axillary nerve: from either a compressive force or a traction injury following anterior dislocation of the shoulder.<ref name="Allen et al">Allen J, Dean K. Recognizing, managing, and testing an axillary- nerve dysfunction. Athletic Therapy Today. 2002;7(2):28-29.</ref><ref name="Apaydin et al">Apaydin N, Tubbs S, Loukas M, Duparc F. [https://www.ncbi.nlm.nih.gov/pubmed/19916067 Review of the surgical anatomy of the axillary nerve and the anatomic basis of its iatrogenic and traumatic injury.] Springer. 2010;32:193-201. | ||
</ref><ref name="Cutts et al">Cutts S, Prempeh M, Drew S. [https://www.ncbi.nlm.nih.gov/pubmed/19126329 Anterior shoulder dislocation.] Ann R Coll Surg Engl. 2009:91:2-7.</ref><ref name="Duralde">Duralde X. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1323394/ Neurologic injuries in the athlete’s shoulder]. Journal of Athletic Training. 2000;35(3):316-328.</ref><ref name="Handoll et al">Handoll HHG, Hanchard NCA, Goodchild LM, Feary J. [https://www.ncbi.nlm.nih.gov/pubmed/24782346 Conservative management following closed reduction of traumatic ; anterior dislocation of the shoulder (review).] Cochrane Database of Systematic Review. 2006;1:1-26.</ref><ref name="Miller">Miller T. [https://www.ncbi.nlm.nih.gov/pubmed/19078679 Peripheral nerve injuries at the shoulder]. The Journal of Manipulative Therapy. 1998;6(4)170-183.</ref><ref name="Neal et al">Neal S, Fields K. [https://www.ncbi.nlm.nih.gov/pubmed/20082510 Peripheral nerve entrapment and injury in the upper extremity.] American Family Physician. 2010; 81(2): 147-155.</ref | </ref><ref name="Cutts et al">Cutts S, Prempeh M, Drew S. [https://www.ncbi.nlm.nih.gov/pubmed/19126329 Anterior shoulder dislocation.] Ann R Coll Surg Engl. 2009:91:2-7.</ref><ref name="Duralde">Duralde X. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1323394/ Neurologic injuries in the athlete’s shoulder]. Journal of Athletic Training. 2000;35(3):316-328.</ref><ref name="Handoll et al">Handoll HHG, Hanchard NCA, Goodchild LM, Feary J. [https://www.ncbi.nlm.nih.gov/pubmed/24782346 Conservative management following closed reduction of traumatic ; anterior dislocation of the shoulder (review).] Cochrane Database of Systematic Review. 2006;1:1-26.</ref><ref name="Miller">Miller T. [https://www.ncbi.nlm.nih.gov/pubmed/19078679 Peripheral nerve injuries at the shoulder]. The Journal of Manipulative Therapy. 1998;6(4)170-183.</ref><ref name="Neal et al">Neal S, Fields K. [https://www.ncbi.nlm.nih.gov/pubmed/20082510 Peripheral nerve entrapment and injury in the upper extremity.] American Family Physician. 2010; 81(2): 147-155.</ref><ref name="Payne et al">Payne M, Doherty T, Sequeira K, Miller T. [https://www.ncbi.nlm.nih.gov/pubmed/19078679 Peripheral nerve injury associated with shoulder trauma: a retrospective study and review of literature.] Journal of Clinical Neuromuscular Disease. 2002; 4(1): 1-6.</ref><ref name="Perlmutter et al">Perlmutter G, Apruzzese W. [https://www.ncbi.nlm.nih.gov/pubmed/9858397 Axillary nerve injuries in contact sports: recommendations for treatment and rehabilitation.] Sports Med. 1998;26(5): 351-360.</ref><ref name="Visser et al">Visser C, Coene L, Brand R, Tavy D. [https://www.ncbi.nlm.nih.gov/pubmed/10463745 The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery a prospective clinical and emg study.] Journal of Bone and Joint Surgery. British volume. 1999; 81-B(4). 679-685.</ref><br> | ||
Axillary nerve injury referred to neuropathy of the axillary nerve. It describes a loss of movement or lack of sensation in the shoulder area of the body. Stress or damage to the axillary nerve, which serves the [[Deltoid|deltoid muscles]] and skin of the [[shoulder]], causes this dysfunction. | Axillary nerve injury referred to neuropathy of the axillary nerve. It describes a loss of movement or lack of sensation in the shoulder area of the body. Stress or damage to the axillary nerve, which serves the [[Deltoid|deltoid muscles]] and skin of the [[shoulder]], causes this dysfunction. | ||
| Line 13: | Line 13: | ||
Since this is a problem with just one nerve, it is a type of Peripheral neuropathy called mononeuropathy. Of all [[brachial plexus]] injuries, axillary nerve palsy represents only 3% to 6% of them. | Since this is a problem with just one nerve, it is a type of Peripheral neuropathy called mononeuropathy. Of all [[brachial plexus]] injuries, axillary nerve palsy represents only 3% to 6% of them. | ||
== '''Epidemiology/Etiology''' | == '''Epidemiology/Etiology'''<ref name="Allen et al" /><ref name="Apaydin et al" /><ref name="Cutts et al" /><ref name="Duralde" /><ref name="Handoll et al" /><ref name="Miller" /><ref name="Neal et al" /><ref name="Payne et al" /><ref name="Perlmutter et al" /><ref name="Visser et al" /> == | ||
*Anterior [http://www.physio-pedia.com/index.php5?title=Shoulder_Dislocation shoulder dislocation] is the most common occurring dislocation at the shoulder. | *Anterior [http://www.physio-pedia.com/index.php5?title=Shoulder_Dislocation shoulder dislocation] is the most common occurring dislocation at the shoulder.<ref name="Apaydin et al" /><ref name="Cutts et al" /><ref name="Duralde" /><ref name="Handoll et al" /><ref name="Miller" /><ref name="Payne et al" /><ref name="Perlmutter et al" /> | ||
Men and women 3:1 | Men and women 3:1<ref name="Handoll et al" /> | ||
9-65% involve axillary nerve injury | 9-65% involve axillary nerve injury<ref name="Apaydin et al" /><ref name="Payne et al" /><ref name="Perlmutter et al" /><ref name="Cox et al">Cox C, Kuhn J. [https://www.ncbi.nlm.nih.gov/pubmed/18772685 Operatice versus nonoperative treatment of acute shoulder dislocation in the athlete.] Current Sports Medicine Reports. 2008;7(5): 263-268.</ref><ref name="McFarland et al">McFarland E, Caicedo J, Kim T, Banchasuek P. [https://www.ncbi.nlm.nih.gov/pubmed/12130416 Axillary nerve injury in anterior shoulder reconstructions: use of a subscapularis muscle- splitting technique and a review of the literature.] Am J Sports Med. 2002;30:601-606.</ref> | ||
23% have combination neuropathies, all involving the axillary nerve | 23% have combination neuropathies, all involving the axillary nerve<ref name="Payne et al" /> | ||
The incidence of brachial plexus and axillary nerve injury increases dramatically following shoulder dislocation in patients ≥50 years of age, if [[fracture]] is associated with the dislocation, and if the duration of the dislocation lasts >12 hours | The incidence of brachial plexus and axillary nerve injury increases dramatically following shoulder dislocation in patients ≥50 years of age, if [[fracture]] is associated with the dislocation, and if the duration of the dislocation lasts >12 hours<ref name="Payne et al" /><ref name="Perlmutter et al" /><ref name="Visser et al" /><ref name="Kazemi">Kazemi M. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2485375/ Acute traumatic anterior glenohumeral dislocation complicated by axillary nerve damage: a case report.] Journal of the Canadian Chiropractic Association. 1998;42(3):150-155.</ref><ref name="Safran">Safran M. [https://www.ncbi.nlm.nih.gov/pubmed/15090401 Nerve injury about the shoulder in athletes, Part 1: Suprascapular nerve and axillary nerve.] Am J Sports Med . 2004;32(3):803-819.</ref> | ||
The incidence of nerve injury doubled with the presence of an associated fracture | The incidence of nerve injury doubled with the presence of an associated fracture<ref name="Visser et al" /><br> | ||
*Traction and compression to the axillary nerve<ref name="Allen et al" /><ref name="Apaydin et al" /><ref name="Miller" /><ref name="Neal et al" /><ref name="Perlmutter et al" /><ref name="Visser et al" />[[Image:Axillary Nerve Fig 1.jpg|frame|right|Figure 1- Depiction of the axillary nerve stretched across the humeral head during dislocation. Adapted from Apaydin et al.]]<ref name="Apaydin et al" /> | *Traction and compression to the axillary nerve<ref name="Allen et al" /><ref name="Apaydin et al" /><ref name="Miller" /><ref name="Neal et al" /><ref name="Perlmutter et al" /><ref name="Visser et al" />[[Image:Axillary Nerve Fig 1.jpg|frame|right|Figure 1- Depiction of the axillary nerve stretched across the humeral head during dislocation. Adapted from Apaydin et al.]]<ref name="Apaydin et al" /> | ||
The axillary nerve becomes stretched across the humerus as it dislocates anteriorly and inferiorly.<ref name="Apaydin et al" /><ref name="Perlmutter et al" /><br> | The axillary nerve becomes stretched across the humerus as it dislocates anteriorly and inferiorly.<ref name="Apaydin et al" /><ref name="Perlmutter et al" /><br> | ||
| Line 44: | Line 44: | ||
The axon and all 3 connective tissue layers (endoneurium, perineurium, and epineurium) remain intact with a decrease in conduction<br> | The axon and all 3 connective tissue layers (endoneurium, perineurium, and epineurium) remain intact with a decrease in conduction<br> | ||
Comparable to a | Comparable to a 1st-degree nerve injury (Sunderland's Classification of Nerve Injury)<br> | ||
====== Axonotmesis ====== | ====== Axonotmesis ====== | ||
| Line 51: | Line 51: | ||
The endoneurium acts as a guide for axonal regeneration<br> | The endoneurium acts as a guide for axonal regeneration<br> | ||
Comparable to a | Comparable to a 2nd degree degree nerve injury <br> | ||
====== Neurotmesis ====== | ====== Neurotmesis ====== | ||
| Line 57: | Line 57: | ||
Connective sheath damage ranges from partial disruption of the endoneurium to complete disruption of the involved nerve | Connective sheath damage ranges from partial disruption of the endoneurium to complete disruption of the involved nerve | ||
* | *3rddegree nerve injury= axon and endoneurium are damaged with preservation of the perineurium | ||
* | *4thdegree nerve injury= axon, endoneurium, and perineurium are damaged with preservation of the epineurium | ||
* | *5thdegree nerve injury= complete disruption of the nerve<br> | ||
<br> | <br> | ||
== '''Characteristics/Clinical Presentation''' == | == '''Characteristics/Clinical Presentation''' == | ||
It is important to note that the clinical presentation of axillary nerve dysfunction is variable and can go undetected, as the concomitant dislocation or fracture may mask the symptoms. | It is important to note that the clinical presentation of axillary nerve dysfunction is variable and can go undetected, as the concomitant dislocation or fracture may mask the symptoms.<ref name="Allen et al" /><ref name="Perlmutter et al" /> Nerve injury should be considered as part of the differential diagnosis process when a patient reports pain, weakness, or paresthesias.<ref name="Neal et al" /><br> | ||
'''Subjective Examination'''<br> | '''Subjective Examination'''<br> | ||
*Generalized mild, dull, and achy pain to the deep or lateral shoulder, with occasional radiation to the proximal arm | *Generalized mild, dull, and achy pain to the deep or lateral shoulder, with occasional radiation to the proximal arm <ref name="Duralde" /><ref name="Miller" /><ref name="Vitanzo et al" /><ref name="Miller 2">Miller T. [https://www.tandfonline.com/doi/abs/10.1179/jmt.1998.6.4.184 Axillary neuropathy following traumatic dislocation of the shoulder: a case study.] The Journal of Manual & Manipulative Therapy. 1998;6(4):184-185.</ref><br> | ||
*Numbness and tingling of the lateral arm and/or posterior aspect of the shoulder | *Numbness and tingling of the lateral arm and/or posterior aspect of the shoulder <ref name="Duralde" /><ref name="Miller" /><ref name="Neal et al" /><ref name="Perlmutter et al" /><ref name="Safran" /><ref name="Miller 2" /> in some cases, persisting 2-4 weeks post-injury <br> | ||
*Feeling of instability | *Feeling of instability<ref name="Miller 2" /><br> | ||
*Weakness, especially with flexion, abduction, and external rotation | *Weakness, especially with flexion, abduction, and external rotation <ref name="Miller" /><ref name="Perlmutter et al" /><ref name="Vitanzo et al" /><ref name="Miller 2" /><br> | ||
*Fatigue, especially with overhead activities, heavy lifting, and/or throwing | *Fatigue, especially with overhead activities, heavy lifting, and/or throwing <ref name="Neal et al" /><ref name="Safran" /><ref name="Vitanzo et al" /><br> | ||
*May/or may not reveal a history of trauma to the shoulder region | *May/or may not reveal a history of trauma to the shoulder region <ref name="Duralde" /><ref name="Miller" /><br> | ||
*History of dislocation with soreness persisting ~1week post-injury | *History of dislocation with soreness persisting ~1week post-injury <ref name="Miller 2" /> | ||
*Easing Factors include: rest, ice, analgesics, and anti-inflammatory medications | *Easing Factors include: rest, ice, analgesics, and anti-inflammatory medications <ref name="Miller" /><ref name="Neal et al" /><ref name="Manske et al">Manske R, Sumler A, Runge J. [http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.1018.8428&rep=rep1&type=pdf Quadrilateral space syndrome.] Humen Kinetics-ATTI.2009;14(2):45-47.</ref><br> | ||
Many athletes with axillary nerve injury may be asymptomatic with incomplete or complete lesions, with the only complaints of weakness and early-onset fatigue with exercise. | Many athletes with axillary nerve injury may be asymptomatic with incomplete or complete lesions, with the only complaints of weakness and early-onset fatigue with exercise. <ref name="Duralde" /><ref name="Safran" /><br> | ||
<br> | <br> | ||
| Line 81: | Line 81: | ||
== '''Differential Diagnosis''' == | == '''Differential Diagnosis''' == | ||
Axillary nerve injury with shoulder dislocation can present similarly to or concomitantly with the following conditions: | Axillary nerve injury with shoulder dislocation can present similarly to or concomitantly with the following conditions: <ref name="Perlmutter et al" /><ref name="Kazemi" /><ref name="Vitanzo et al" /><br> | ||
==== 1. Unhappy Triad ==== | ==== 1. Unhappy Triad ==== | ||
The “Unhappy Triad” consists of a shoulder dislocation that results in both a [http://www.physio-pedia.com/index.php5?title=Test_Item_Cluster_-_Full-Thickness_Rotator_Cuff_Tear rotator cuff tear] and axillary nerve injury.<br> | The “Unhappy Triad” consists of a shoulder dislocation that results in both a [http://www.physio-pedia.com/index.php5?title=Test_Item_Cluster_-_Full-Thickness_Rotator_Cuff_Tear rotator cuff tear] and axillary nerve injury.<br> | ||
*Occurs in 9-18% of anterior shoulder dislocations | *Occurs in 9-18% of anterior shoulder dislocations<ref name="Payne et al" /> | ||
*Risk of an “unhappy triad” with anterior shoulder dislocation increases after the age of 40 | *Risk of an “unhappy triad” with anterior shoulder dislocation increases after the age of 40<ref name="Payne et al" /> | ||
==== 2. Quadrilateral Space Syndrome ==== | ==== 2. Quadrilateral Space Syndrome ==== | ||
QSS is an “uncommon condition that involves the compression of the posterior humeral circumflex artery and the axillary nerve within the quadrilateral space,” secondary to an acute trauma or from overuse, especially with overhead sports like throwing and swimming. | QSS is an “uncommon condition that involves the compression of the posterior humeral circumflex artery and the axillary nerve within the quadrilateral space,” secondary to an acute trauma or from overuse, especially with overhead sports like throwing and swimming.<ref name="Manske et al" /> | ||
*Cardinal Features | *Cardinal Features<ref name="Manske et al" /> | ||
**Generalized shoulder pain | **Generalized shoulder pain | ||
**Paresthesias in a nondermatomal pattern | **Paresthesias in a nondermatomal pattern | ||
**Point tenderness to the quadrilateral space | **Point tenderness to the quadrilateral space | ||
**(+) arteriogram findings with the shoulder in abduction and external rotation | **(+) arteriogram findings with the shoulder in abduction and external rotation | ||
*Symptoms are typically present with the arm in an overhead position, especially in late cocking or the early acceleration phases of throwing | *Symptoms are typically present with the arm in an overhead position, especially in late cocking or the early acceleration phases of throwing<ref name="Manske et al" /> | ||
==== 3. Posterior Cord of the Brachial Plexus Injury ==== | ==== 3. Posterior Cord of the Brachial Plexus Injury ==== | ||
| Line 102: | Line 102: | ||
==== [http://www.physio-pedia.com/Parsonage-Turner_Syndrome 5. Parsonage-Turner Syndrome (PTS)] ==== | ==== [http://www.physio-pedia.com/Parsonage-Turner_Syndrome 5. Parsonage-Turner Syndrome (PTS)] ==== | ||
PTS is an uncommon, idiopathic condition, characterized by an acute onset of intense pain, without a mechanism of injury, that subsides within days-weeks, leaving behind residual weakness/paralysis in upper extremity muscles. | PTS is an uncommon, idiopathic condition, characterized by an acute onset of intense pain, without a mechanism of injury, that subsides within days-weeks, leaving behind residual weakness/paralysis in upper extremity muscles.<ref name="Mamula et al">Mamula C, Erhard R, Piva S. [https://www.ncbi.nlm.nih.gov/pubmed/16294987 Cervical radiculopathy or parsonage-turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms.] Journal of Orthopaedic Sports Physical Therapy. 2005; 55(10): 659-664.</ref><br> | ||
*Symptoms are NOT related to neck movements. | *Symptoms are NOT related to neck movements. | ||
*Aka: Acute brachial neuritis | *Aka: Acute brachial neuritis | ||
<br>For more details, see [http://www.physio-pedia.com/index.php5?title=Image:Axillary_Nerve_Diff_Dx_Chart.pdf <span style="font-style: italic;"><span style="font-weight: bold;">Differential Diagnosis Chart</span></span>]. | <br>For more details, see [http://www.physio-pedia.com/index.php5?title=Image:Axillary_Nerve_Diff_Dx_Chart.pdf <span style="font-style: italic;"><span style="font-weight: bold;">Differential Diagnosis Chart</span></span>].<ref name="Miller" /><ref name="Neal et al" /><ref name="Payne et al" /><ref name="Perlmutter et al" /><ref name="Kazemi" /><ref name="Safran" /><ref name="Vitanzo et al" /><ref name="Miller 2" /><ref name="Manske et al" /><ref name="Mamula et al" /><ref name="Hertel et al">Hertel R, Lambert SM, Ballmer FT. [https://www.ncbi.nlm.nih.gov/pubmed/9593085 The deltoid extension lag sign for diagnosis and grading of axillary nerve palsy.] J Shoulder & Elbow Surgery 1998;7(1):97-108.</ref><ref name="Wainner et al">Wainner R, Fritz J, Irrgang J, Boninger M, Delitto A, Allison S. [https://www.ncbi.nlm.nih.gov/pubmed/12544957 Reliability and diagnositic accuracy of the clinical examination and patient self report measures for cervical radiculopathy.] SPINE. 2003; 28(1):52-62.</ref><ref name="Park et al">Park H, Yokota A, Gill H, Rassi G, McFarland E. [https://www.ncbi.nlm.nih.gov/pubmed/15995110 Diagnostic accuracy of clinical tests for the differential degrees of subacromial impingement syndrome.] The Journal of Bone and Joint Surgery. 2005;87-A(7): 1446-1455.</ref><br> | ||
== '''Examination''' == | == '''Examination''' == | ||
Physical examination should begin with a screening consisting of an evaluation of the head and neck which shouldn’t reveal any abnormalities. | Physical examination should begin with a screening consisting of an evaluation of the head and neck which shouldn’t reveal any abnormalities.<ref name="Perlmutter et al" /><ref name="Miller 2" /> If the patient presents with a recent shoulder dislocation, presence of a radial pulse and sensation and movement of the digits should also be assessed as part of the initial screening.<ref name="Neal et al" /><br> | ||
[[Image:Axillary Nerve Fig 3.jpg|Image:Axillary_Nerve_Fig_3.jpg]]<br> | [[Image:Axillary Nerve Fig 3.jpg|Image:Axillary_Nerve_Fig_3.jpg]]<br> | ||
Figure 3<ref name="Allen et al" /><ref name="Duralde" /><ref name="Miller" /><ref name="Neal et al" /><ref name="Perlmutter et al" /><ref name="Visser et al" /><ref name="Safran" /><ref name="Vitanzo et al" /><ref name="Miller 2" /><ref name="Manske et al" /> | |||
<br>[[Image:Axillary Nerve Fig 4.jpg|frame|Figure 4- Picture of significant atrophy to the left deltoid and mild atrophy to the teres minor. Adapted from Vitanzo et al.]]<ref name="Vitanzo et al" /> [[Image:Axillary Extension Lag Fig 5.jpg|frame|center|Figure 5- Extension Lag Sign: Elevate the patient's arm to near full extension. Ask the patient to actively maintain that position. A (+) test is if the patient's arm drops. Adapted from Hertel et al.]]<ref name="Hertel et al" /> | |||
{| cellspacing="1" cellpadding="1" style="width: 707px; height: 25px;" | {| cellspacing="1" cellpadding="1" style="width: 707px; height: 25px;" | ||
| Line 123: | Line 123: | ||
|} | |} | ||
Click for more information on the [http://www.physio-pedia.com/index.php5?title=Inferior_Sulcus_Test Sulcus Sign]Click for more information on the [http://www.physio-pedia.com/index.php5?title=Apprehension_Test Apprehension] & [http://www.physio-pedia.com/index.php5?title=Jobes_Relocation_Test Jobe Relocation] Test | |||
It is important to note that the physical examination findings are dependent on the extent of the axillary nerve damage. Furthermore, there is a lack of consensus regarding the ability of a patient to retain normal range of motion and function when presenting with axillary nerve injury. | It is important to note that the physical examination findings are dependent on the extent of the axillary nerve damage. Furthermore, there is a lack of consensus regarding the ability of a patient to retain normal range of motion and function when presenting with axillary nerve injury. <ref name="Perlmutter et al" /> | ||
[[Image:Axillary Nerve Injury Fig 6.jpg|Image:Axillary_Nerve_Injury_Fig_6.jpg]] | [[Image:Axillary Nerve Injury Fig 6.jpg|Image:Axillary_Nerve_Injury_Fig_6.jpg]]Figure 6 <ref name="Perlmutter et al" /><ref name="Safran" /><ref name="Manske et al" /><br> | ||
Accurate manual muscle testing is necessary as 60% of athletes may be able to elevate the effected arm by compensating with and recruiting the [[pectoralis major]] and [[supraspinatus]] muscle groups, and prevent subluxation by utilizing the supraspinatus and long head of the [[Biceps Femoris|biceps]] muscles. | Accurate manual muscle testing is necessary as 60% of athletes may be able to elevate the effected arm by compensating with and recruiting the [[pectoralis major]] and [[supraspinatus]] muscle groups, and prevent subluxation by utilizing the supraspinatus and long head of the [[Biceps Femoris|biceps]] muscles. <ref name="Duralde" /><ref name="Perlmutter et al" /><ref name="Safran" /> However, there is no evidence to translate this statistic to the general population. | ||
<br>The sensory examination of the axillary nerve has been calculated to have a poor sensitivity (7%) in detecting the presence of axillary nerve injury, emphasizing the need for electrodiagnostic evaluation for a patient with persistent weakness and decreased shoulder function following shoulder dislocation. | <br>The sensory examination of the axillary nerve has been calculated to have a poor sensitivity (7%) in detecting the presence of axillary nerve injury, emphasizing the need for electrodiagnostic evaluation for a patient with persistent weakness and decreased shoulder function following shoulder dislocation. <ref name="Payne et al" /><ref name="Visser et al" /><br> | ||
== '''Clinical Diagnosis''' == | == '''Clinical Diagnosis''' == | ||
The best means to confirm a concomitant axillary nerve injury with shoulder dislocation includes detailed subjective and objective clinical examinations, along with electromyogram (EMG) studies. | The best means to confirm a concomitant axillary nerve injury with shoulder dislocation includes detailed subjective and objective clinical examinations, along with electromyogram (EMG) studies.<ref name="Miller" /> | ||
==== Clinical Exam ==== | ==== Clinical Exam ==== | ||
==== EMG ==== | ==== EMG ==== | ||
The diagnostic test of choice to identify nerve conduction loss is EMG However, significant nerve damage may not be identified until 2-3 weeks post-injury. | The diagnostic test of choice to identify nerve conduction loss is EMG However, significant nerve damage may not be identified until 2-3 weeks post-injury.<ref name="Apaydin et al" /><ref name="Miller" /><ref name="Perlmutter et al" /> EMG can distinguish between atrophy secondary to pain or that of nerve injury.<ref name="Duralde" /> EMG studies also serve as means to track the patient’s progression or regression throughout the recovery phase, ultimately indicating whether a surgical or conservative treatment approach is needed | ||
==== MRI | ==== MRI<ref name="Neal et al" /> ==== | ||
MRI is rarely used for initial evaluation of a typical nerve injury It may be useful if the diagnosis is unclear or if there is evidence of abnormal recovery A normal MRI does not rule out nerve injury.<ref name="Duralde" /> The duration of recovery from axillary nerve injury is prolonged, lasting as long as up to 35 weeks. | MRI is rarely used for initial evaluation of a typical nerve injury It may be useful if the diagnosis is unclear or if there is evidence of abnormal recovery A normal MRI does not rule out nerve injury.<ref name="Duralde" /> The duration of recovery from axillary nerve injury is prolonged, lasting as long as up to 35 weeks.<ref name="Visser et al" /> | ||
Neuropraxias ( | Neuropraxias (1st degree) nerve injury <ref name="Duralde" /> | ||
Full recovery occurs 85% to 100% of the time with conservative management within 6 to 12 months. | Full recovery occurs 85% to 100% of the time with conservative management within 6 to 12 months.<ref name="Safran" /><ref name="Vitanzo et al" /> Muscle weakness due to the axillary nerve lesion may recover spontaneously as the tissues from the shoulder dislocation heal.<ref name="Visser et al" /> | ||
Axonotmesis ( | Axonotmesis (2nd degree) nerve injury | ||
The recovery rate is near 80% secondary to the short distance between the site of injury and the muscle endplates. | The recovery rate is near 80% secondary to the short distance between the site of injury and the muscle endplates. <ref name="Duralde" /><ref name="Perlmutter et al" /> Recovery should be evident between 3-4 months post-injury <ref name="Duralde" /> EMG re-evaluations should be preformed at monthly intervals for signs of regeneration. By 6 months post-injury, if there are no signs of functional return, surgical exploration and possible nerve grafting are recommended. <ref name="Duralde" /> | ||
Neurotmesis ( | Neurotmesis (3rd-5th degree) nerve injury | ||
Without surgical intervention, there is typically no recovery. | Without surgical intervention, there is typically no recovery. <ref name="Perlmutter et al" /> | ||
== '''Medical Management''' '''''(current best evidence)''''' == | == '''Medical Management''' '''''(current best evidence)''''' == | ||
=== Surgery === | === Surgery === | ||
There is uncertainty among clinicians as to the appropriate time for surgical exploration following isolated axillary nerve injury, with some authors recommending exploration at 3 months post-injury while others recommend at 6 to 12 months post-injury. | There is uncertainty among clinicians as to the appropriate time for surgical exploration following isolated axillary nerve injury, with some authors recommending exploration at 3 months post-injury while others recommend at 6 to 12 months post-injury.<ref name="Perlmutter et al" /><ref name="Manske et al" /> The site of the axillary nerve injury is variable, making both anterior and/or posterior surgical approaches appropriate.<ref name="Duralde" /> If the axillary nerve cannot be repaired without tension, cable grafts are required. Indications for surgery are rare but must be understood by clinicians in order to maximize outcomes and minimize complications.<ref name="Neal et al" /> | ||
==== Indications for surgery: ==== | ==== Indications for surgery: ==== | ||
Suspicion of osteophyte formation or compression in the quadrilateral space. | Suspicion of osteophyte formation or compression in the quadrilateral space.<ref name="Miller" /> | ||
No axillary nerve recovery observed by 3 to 4 months following injury. | No axillary nerve recovery observed by 3 to 4 months following injury.<ref name="Perlmutter et al" /> | ||
No improvements were seen after 3 to 6 months of conservative treatment. | No improvements were seen after 3 to 6 months of conservative treatment.<ref name="Vitanzo et al" /> | ||
No EMG/NCV evidence of recovery by 3 to 6 months after injury. | No EMG/NCV evidence of recovery by 3 to 6 months after injury.<ref name="Safran" /> | ||
Surgery for shoulder instability in young active patients reduces the likelihood of recurrent anterior shoulder dislocations, therefore reducing the possibility of axillary nerve compromise. | Surgery for shoulder instability in young active patients reduces the likelihood of recurrent anterior shoulder dislocations, therefore reducing the possibility of axillary nerve compromise.<ref name="Handoll et al 2" /> | ||
In the rare occasion that surgery is indicated, there are several types of surgeries which can be considered by the patient and his surgeon. | In the rare occasion that surgery is indicated, there are several types of surgeries which can be considered by the patient and his surgeon.<ref name="Neal et al" /><ref name="Safran" />There is a better prognosis if the surgery is performed within 6 months of the injury but functional improvements can be expected with surgical intervention up to 12 months year after the injury.<ref name="Safran" /><ref name="Vitanzo et al" /> The clinician should be aware of these prognostic correlations between time of injury and time of surgery to maximize the patient's outcome. Prognosis is good in 90% of patients <ref name="Duralde" /> | ||
==== Surgical Procedures: ==== | ==== Surgical Procedures: ==== | ||
| Line 180: | Line 180: | ||
[http://medical-dictionary.thefreedictionary.com/Neurorrhaphy Neurorrhaphy] | [http://medical-dictionary.thefreedictionary.com/Neurorrhaphy Neurorrhaphy] | ||
[http://medical-dictionary.thefreedictionary.com/Nerve+grafting Nerve grafting] The sural nerve is commonly used during nerve grafting, not only of the axillary nerve, but in other peripheral nerves injuries as well. Prognosis for the axillary nerve with graft repair is better than other peripheral nerve repairs secondary to its short length. | [http://medical-dictionary.thefreedictionary.com/Nerve+grafting Nerve grafting] The sural nerve is commonly used during nerve grafting, not only of the axillary nerve, but in other peripheral nerves injuries as well. Prognosis for the axillary nerve with graft repair is better than other peripheral nerve repairs secondary to its short length. <ref name="Payne et al" /><ref name="Perlmutter et al" /> | ||
[http://medical-dictionary.thefreedictionary.com/Neurotization Neurotization]<br> | [http://medical-dictionary.thefreedictionary.com/Neurotization Neurotization]<br> | ||
=== Nonsurgical Reduction === | === Nonsurgical Reduction === | ||
Reduction eliminates the need for surgical intervention, and is followed by immobilization and physical therapy management. | Reduction eliminates the need for surgical intervention, and is followed by immobilization and physical therapy management.<ref name="Deyle et al">Deyle G, Nagel K. [https://www.ncbi.nlm.nih.gov/pubmed/17469672 Prolonged immobilization in abduction and neutral rotation for a first-episode anterior shoulder dislocation.] Journal of orthopedic sports physical therapy. 2007; 37(4): 192-198.</ref> | ||
Immobilization for young adult males 4-6 weeks | Immobilization for young adult males 4-6 weeks <ref name="Handoll et al 2">Handoll HHG, Al-Maiyah MA. [https://www.ncbi.nlm.nih.gov/pubmed/14974064 Surgical versus non-surgical treatment for acute anterior shoulder dislocation.]Cochrane Database of Systematic Review. 2004;1:1-37.</ref><ref name="Deyle et al" /> Immobilization for older patients 7-10 days <ref name="Visser et al" /> Precaution should be taken during manipulative reduction of a dislocation, in which traction together with rotation or abduction are applied simultaneously, creating extra distraction and increasing the risk of axillary nerve damage. <ref name="Visser et al" /> Other treatments include: [[Pain Medications|NSAIDS]], rest, [[Cryotherapy|ice]] <ref name="Miller" /><ref name="Neal et al" /><ref name="Manske et al" /><ref name="Handoll et al 2" /><br> | ||
== '''Physical Therapy Management''' '''''(current best evidence)''''' == | == '''Physical Therapy Management''' '''''(current best evidence)''''' == | ||
Current research encompassing treatment and intervention of axillary nerve injuries following shoulder dislocation is limited. The research suggests that the management of the axillary nerve damage following shoulder dislocation is treated in the same manner as treating an isolated dislocation, with an emphasis on strengthening and stimulation of the deltoids and [[Teres Minor|teres minor muscles]]. | Current research encompassing treatment and intervention of axillary nerve injuries following shoulder dislocation is limited. The research suggests that the management of the axillary nerve damage following shoulder dislocation is treated in the same manner as treating an isolated dislocation, with an emphasis on strengthening and stimulation of the deltoids and [[Teres Minor|teres minor muscles]].<ref name="Duralde" /><ref name="Kazemi" />There should be a great amount of importance placed on allowing ligamentous, capsular, and nervous tissues time to heal while preventing joint stiffness, which could ultimately hinder function greater in the long run.<ref name="Neal et al" /><ref name="Visser et al" /><ref name="Kazemi" /> | ||
=== '''Non-Surgical Physical Therapy Treatment''' === | === '''Non-Surgical Physical Therapy Treatment''' === | ||
==== '''0-2 weeks''' | ==== '''0-2 weeks'''<ref name="Duralde" /><ref name="Visser et al" /><ref name="Kazemi" /><ref name="Miller 2" /><ref name="Deyle et al" /><ref name="Gibson et al">Gibson K, Growse A, Korda L, Wray E, MacDermid J. [https://www.ncbi.nlm.nih.gov/pubmed/15162108 The effectiveness of rehabilitation for nonoperative management of shoulder instability: a systematic review.] Journal of Hand Therapy. 2004; 17(2): 229-242</ref> ==== | ||
Shoulder immobilization via sling after reduction. There is insufficient evidence to support whether physical therapy should be initiated during or after immobilization. | Shoulder immobilization via sling after reduction. There is insufficient evidence to support whether physical therapy should be initiated during or after immobilization. <ref name="Handoll et al" /> | ||
====== [http://www.youtube.com/watch?v=HSYpMuRXJBs Isometric Strengthening]; Dosing: 10 seconds X 6 repetitions X 2 day within limits of pain ====== | ====== [http://www.youtube.com/watch?v=HSYpMuRXJBs Isometric Strengthening]; Dosing: 10 seconds X 6 repetitions X 2 day within limits of pain ====== | ||
| Line 218: | Line 218: | ||
Active Range of Motion (AROM); Dosing 10 repetitions X 2 day: Elbow(Flexion, Extension ,Pronation, Supination); Wrist (Flexion, Extension, Radial/Ulnar deviation); Hand (Opening/Closing Fist) | Active Range of Motion (AROM); Dosing 10 repetitions X 2 day: Elbow(Flexion, Extension ,Pronation, Supination); Wrist (Flexion, Extension, Radial/Ulnar deviation); Hand (Opening/Closing Fist) | ||
Pendulum Exercises 3 sets x 30 seconds | Pendulum Exercises 3 sets x 30 seconds<ref name="Kazemi" /> | ||
Postural/Periscapular Muscular Strengthening/Neuromuscular Re-education | Postural/Periscapular Muscular Strengthening/Neuromuscular Re-education<ref name="Perlmutter et al" /><ref name="Miller 2" /><ref name="Deyle et al" /> | ||
====== Strengthening of Target Muscles | ====== Strengthening of Target Muscles<ref name="Kazemi" /> ====== | ||
Deltoid: “Neuromuscular electrical stimulation of the deltoid muscle can also be helpful to decrease the extent of deltoid muscle atrophy.” | Deltoid: “Neuromuscular electrical stimulation of the deltoid muscle can also be helpful to decrease the extent of deltoid muscle atrophy.” <ref name="Allen et al" /><ref name="Perlmutter et al" /> | ||
[[Rhomboids|Rhomboid Major/Minor]] | [[Rhomboids|Rhomboid Major/Minor]] | ||
| Line 231: | Line 231: | ||
Upper/Middle/Lower [[Trapezius]] | Upper/Middle/Lower [[Trapezius]] | ||
'''''PRECAUTION''''': against shoulder abduction & flexion beyond 90 degrees, and ER beyond neutral in the first 3 weeks. | '''''PRECAUTION''''': against shoulder abduction & flexion beyond 90 degrees, and ER beyond neutral in the first 3 weeks.<ref name="Kazemi" /> | ||
Older individuals have lower rates of re-occurrence of shoulder dislocation and an increase in incidence of joint stiffness. Therefore, progressive strengthening and proprioceptive training should be initiated sooner than in younger individuals, who usually begin around week 6. | Older individuals have lower rates of re-occurrence of shoulder dislocation and an increase in incidence of joint stiffness. Therefore, progressive strengthening and proprioceptive training should be initiated sooner than in younger individuals, who usually begin around week 6. <ref name="Miller" /><ref name="Kazemi" /> | ||
==== '''4-6 weeks''' ==== | ==== '''4-6 weeks''' ==== | ||
D/C sling | D/C sling | ||
Strengthening Program light resistive exercises | Strengthening Program light resistive exercises <ref name="Deyle et al" /> | ||
Target muscles: [[Deltoid|Deltoids]], [[Rotator Cuff|Rotator Cuff muscles]], Postural muscles | Target muscles: [[Deltoid|Deltoids]], [[Rotator Cuff|Rotator Cuff muscles]], Postural muscles | ||
Proprioceptive Techniques | Proprioceptive Techniques <ref name="Kazemi" /><ref name="Miller 2" /><ref name="Deyle et al" /> [[Proprioception|PNF]] diagonals | ||
Closed Chained Activities | Closed Chained Activities | ||
| Line 250: | Line 250: | ||
Weight Shifts | Weight Shifts | ||
==== '''6 weeks-Discharge ''' | ==== '''6 weeks-Discharge '''<ref name="Cutts et al" /><ref name="Handoll et al 2" /><ref name="Robinson et al" /><ref name="Mahaffey et al" /> ==== | ||
Continue ROM, glenohumeral and scapulothoracic stabilization/strengthening exercises, [[proprioception]], and joint mobility, while maintaining optimal conditions for tissue healing | Continue ROM, glenohumeral and scapulothoracic stabilization/strengthening exercises, [[proprioception]], and joint mobility, while maintaining optimal conditions for tissue healing | ||
Begin to initiate sport/job specific activities, progressing to full return as patient’s functional status allows | Begin to initiate sport/job specific activities, progressing to full return as patient’s functional status allows | ||
There is no consensus of when return to sport/work is appropriate following an axillary nerve injury. In general, improvement on the EMG and at least 80% return of deltoid muscle strength is recommended. | There is no consensus of when return to sport/work is appropriate following an axillary nerve injury. In general, improvement on the EMG and at least 80% return of deltoid muscle strength is recommended. <ref name="Cutts et al" /><ref name="Handoll et al 2" /> | ||
It has been suggested that return to activity for shoulder dislocation is approximately 12 weeks, and 16 weeks for competitive sports. | It has been suggested that return to activity for shoulder dislocation is approximately 12 weeks, and 16 weeks for competitive sports. <ref name="Robinson et al">Robinson M, Howes J, Murdoch H, Will E. Graham C. [https://www.ncbi.nlm.nih.gov/pubmed/17079387 After primary traumatic anterior shoulder dislocation in young patients.] The Journal of Bone Surgery. 2006;88(11): 2326-2336.</ref><ref name="Mahaffey et al">Mahaffey B, Smith P. [https://www.ncbi.nlm.nih.gov/pubmed/17079387 Shoulder instability in young athletes.] American Family Physician. 1999;59(10): 2773-2782.</ref> | ||
''Note'': Progression of these interventions with increased weight or resistance should be based on each individual patient and their level of pain and perceived joint stability throughout a controlled movement. | ''Note'': Progression of these interventions with increased weight or resistance should be based on each individual patient and their level of pain and perceived joint stability throughout a controlled movement.<ref name="Kazemi" /> | ||
Conservative physical therapy treatment can last between 3 to 6 months. It is essential that the physical therapist continuously monitor the progression of axillary nerve reinnervation during treatment and contact the patient’s physician if there are no signs of improvement between 3 to 4 months. | Conservative physical therapy treatment can last between 3 to 6 months. It is essential that the physical therapist continuously monitor the progression of axillary nerve reinnervation during treatment and contact the patient’s physician if there are no signs of improvement between 3 to 4 months.<ref name="Neal et al" /><ref name="Perlmutter et al" /> | ||
<br> | <br> | ||
| Line 271: | Line 271: | ||
=== '''Post-Surgical Physical Therapy''' === | === '''Post-Surgical Physical Therapy''' === | ||
There is a lack of research to support how long a patient should be immobilized after surgical repair of the axillary nerve. Current recommendations report that the shoulder should be immobilized for 4 to 6 weeks, after which rehabilitation should focus on increasing shoulder range of motion and strengthening. | There is a lack of research to support how long a patient should be immobilized after surgical repair of the axillary nerve. Current recommendations report that the shoulder should be immobilized for 4 to 6 weeks, after which rehabilitation should focus on increasing shoulder range of motion and strengthening. <ref name="Manske et al" /> | ||
== '''Clinical Bottom Line'''[http://www.searchmedica.com/?parentreferrer=http://infections.consultantlive.com/display/article/1145625/1435040&c=pc] == | == '''Clinical Bottom Line'''[http://www.searchmedica.com/?parentreferrer=http://infections.consultantlive.com/display/article/1145625/1435040&c=pc] == | ||
Revision as of 03:58, 5 February 2019
Original Editor - Kimberley Anlauf
Top Contributors - Kimberley Anlauf, Vidya Acharya, Kim Jackson, Amanda Ager, Samuel Adedigba, Garima Gedamkar, Uchechukwu Chukwuemeka, Bianca Camacho, Evan Thomas, 127.0.0.1, Admin, Tony Lowe, Leana Louw, Michael Gillespie, Chrysolite Jyothi Kommu, Johnathan Fahrner, WikiSysop, Claire Knott, Jose Antonio Cadena, Abbey Wright, Jeremy Brady, Peter Zatezalo, Wendy Walker and Naomi O'Reilly
Definition/Description[edit | edit source]
Axillary nerve injury is characterised by trauma to the axillary nerve: from either a compressive force or a traction injury following anterior dislocation of the shoulder.[1][2][3][4][5][6][7][8][9][10]
Axillary nerve injury referred to neuropathy of the axillary nerve. It describes a loss of movement or lack of sensation in the shoulder area of the body. Stress or damage to the axillary nerve, which serves the deltoid muscles and skin of the shoulder, causes this dysfunction.
Since this is a problem with just one nerve, it is a type of Peripheral neuropathy called mononeuropathy. Of all brachial plexus injuries, axillary nerve palsy represents only 3% to 6% of them.
Epidemiology/Etiology[1][2][3][4][5][6][7][8][9][10][edit | edit source]
- Anterior shoulder dislocation is the most common occurring dislocation at the shoulder.[2][3][4][5][6][8][9]
Men and women 3:1[5]
9-65% involve axillary nerve injury[2][8][9][11][12]
23% have combination neuropathies, all involving the axillary nerve[8]
The incidence of brachial plexus and axillary nerve injury increases dramatically following shoulder dislocation in patients ≥50 years of age, if fracture is associated with the dislocation, and if the duration of the dislocation lasts >12 hours[8][9][10][13][14]
The incidence of nerve injury doubled with the presence of an associated fracture[10]
- Traction and compression to the axillary nerve[1][2][6][7][9][10][2]
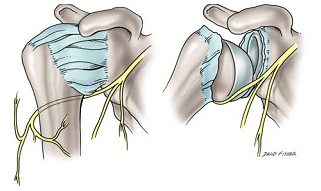 Figure 1- Depiction of the axillary nerve stretched across the humeral head during dislocation. Adapted from Apaydin et al.
Figure 1- Depiction of the axillary nerve stretched across the humeral head during dislocation. Adapted from Apaydin et al.

The axillary nerve becomes stretched across the humerus as it dislocates anteriorly and inferiorly.[2][9]
Propagated tension due to overstretching of the axillary nerve over the humeral head during shoulder dislocations may cause elongation of the free portion of the axillary nerve and the increased tension may even result in axillary nerve avulsions from the posterior cord of brachial plexus.[2][9]
The axillary nerve is susceptible to injury at several sites, including the origin of the nerve from the posterior cord, the anterior inferior aspect of the subscapularis muscle and shoulder capsule, the quadrilateral space, and within the subfascial surface of the deltoid muscle.[9]

Nerve Injury Overview[edit | edit source]
Nerve regeneration takes place at a rate of ~1mm/day
Seddon's Classification of Nerve Injury[edit | edit source]
Neuropraxia[edit | edit source]
The axon and all 3 connective tissue layers (endoneurium, perineurium, and epineurium) remain intact with a decrease in conduction
Comparable to a 1st-degree nerve injury (Sunderland's Classification of Nerve Injury)
Axonotmesis[edit | edit source]
Axonal damage is present with preservation of the endoneurium
The endoneurium acts as a guide for axonal regeneration
Comparable to a 2nd degree degree nerve injury
Neurotmesis[edit | edit source]
Axonal damage is present
Connective sheath damage ranges from partial disruption of the endoneurium to complete disruption of the involved nerve
- 3rddegree nerve injury= axon and endoneurium are damaged with preservation of the perineurium
- 4thdegree nerve injury= axon, endoneurium, and perineurium are damaged with preservation of the epineurium
- 5thdegree nerve injury= complete disruption of the nerve
Characteristics/Clinical Presentation[edit | edit source]
It is important to note that the clinical presentation of axillary nerve dysfunction is variable and can go undetected, as the concomitant dislocation or fracture may mask the symptoms.[1][9] Nerve injury should be considered as part of the differential diagnosis process when a patient reports pain, weakness, or paresthesias.[7]
Subjective Examination
- Generalized mild, dull, and achy pain to the deep or lateral shoulder, with occasional radiation to the proximal arm [4][6][15][16]
- Numbness and tingling of the lateral arm and/or posterior aspect of the shoulder [4][6][7][9][14][16] in some cases, persisting 2-4 weeks post-injury
- Feeling of instability[16]
- Weakness, especially with flexion, abduction, and external rotation [6][9][15][16]
- Fatigue, especially with overhead activities, heavy lifting, and/or throwing [7][14][15]
- May/or may not reveal a history of trauma to the shoulder region [4][6]
- History of dislocation with soreness persisting ~1week post-injury [16]
- Easing Factors include: rest, ice, analgesics, and anti-inflammatory medications [6][7][17]
Many athletes with axillary nerve injury may be asymptomatic with incomplete or complete lesions, with the only complaints of weakness and early-onset fatigue with exercise. [4][14]
Differential Diagnosis[edit | edit source]
Axillary nerve injury with shoulder dislocation can present similarly to or concomitantly with the following conditions: [9][13][15]
1. Unhappy Triad[edit | edit source]
The “Unhappy Triad” consists of a shoulder dislocation that results in both a rotator cuff tear and axillary nerve injury.
- Occurs in 9-18% of anterior shoulder dislocations[8]
- Risk of an “unhappy triad” with anterior shoulder dislocation increases after the age of 40[8]
2. Quadrilateral Space Syndrome[edit | edit source]
QSS is an “uncommon condition that involves the compression of the posterior humeral circumflex artery and the axillary nerve within the quadrilateral space,” secondary to an acute trauma or from overuse, especially with overhead sports like throwing and swimming.[17]
- Cardinal Features[17]
- Generalized shoulder pain
- Paresthesias in a nondermatomal pattern
- Point tenderness to the quadrilateral space
- (+) arteriogram findings with the shoulder in abduction and external rotation
- Symptoms are typically present with the arm in an overhead position, especially in late cocking or the early acceleration phases of throwing[17]
3. Posterior Cord of the Brachial Plexus Injury[edit | edit source]
4. C5-6 Cervical Radiculopathy[edit | edit source]
5. Parsonage-Turner Syndrome (PTS)[edit | edit source]
PTS is an uncommon, idiopathic condition, characterized by an acute onset of intense pain, without a mechanism of injury, that subsides within days-weeks, leaving behind residual weakness/paralysis in upper extremity muscles.[18]
- Symptoms are NOT related to neck movements.
- Aka: Acute brachial neuritis
For more details, see Differential Diagnosis Chart.[6][7][8][9][13][14][15][16][17][18][19][20][21]
Examination[edit | edit source]
Physical examination should begin with a screening consisting of an evaluation of the head and neck which shouldn’t reveal any abnormalities.[9][16] If the patient presents with a recent shoulder dislocation, presence of a radial pulse and sensation and movement of the digits should also be assessed as part of the initial screening.[7]

Figure 3[1][4][6][7][9][10][14][15][16][17]


| [22] | [23] |
Click for more information on the Sulcus SignClick for more information on the Apprehension & Jobe Relocation Test
It is important to note that the physical examination findings are dependent on the extent of the axillary nerve damage. Furthermore, there is a lack of consensus regarding the ability of a patient to retain normal range of motion and function when presenting with axillary nerve injury. [9]
Image:Axillary_Nerve_Injury_Fig_6.jpgFigure 6 [9][14][17]
Accurate manual muscle testing is necessary as 60% of athletes may be able to elevate the effected arm by compensating with and recruiting the pectoralis major and supraspinatus muscle groups, and prevent subluxation by utilizing the supraspinatus and long head of the biceps muscles. [4][9][14] However, there is no evidence to translate this statistic to the general population.
The sensory examination of the axillary nerve has been calculated to have a poor sensitivity (7%) in detecting the presence of axillary nerve injury, emphasizing the need for electrodiagnostic evaluation for a patient with persistent weakness and decreased shoulder function following shoulder dislocation. [8][10]
Clinical Diagnosis[edit | edit source]
The best means to confirm a concomitant axillary nerve injury with shoulder dislocation includes detailed subjective and objective clinical examinations, along with electromyogram (EMG) studies.[6]
Clinical Exam[edit | edit source]
EMG[edit | edit source]
The diagnostic test of choice to identify nerve conduction loss is EMG However, significant nerve damage may not be identified until 2-3 weeks post-injury.[2][6][9] EMG can distinguish between atrophy secondary to pain or that of nerve injury.[4] EMG studies also serve as means to track the patient’s progression or regression throughout the recovery phase, ultimately indicating whether a surgical or conservative treatment approach is needed
MRI[7][edit | edit source]
MRI is rarely used for initial evaluation of a typical nerve injury It may be useful if the diagnosis is unclear or if there is evidence of abnormal recovery A normal MRI does not rule out nerve injury.[4] The duration of recovery from axillary nerve injury is prolonged, lasting as long as up to 35 weeks.[10]
Neuropraxias (1st degree) nerve injury [4]
Full recovery occurs 85% to 100% of the time with conservative management within 6 to 12 months.[14][15] Muscle weakness due to the axillary nerve lesion may recover spontaneously as the tissues from the shoulder dislocation heal.[10]
Axonotmesis (2nd degree) nerve injury
The recovery rate is near 80% secondary to the short distance between the site of injury and the muscle endplates. [4][9] Recovery should be evident between 3-4 months post-injury [4] EMG re-evaluations should be preformed at monthly intervals for signs of regeneration. By 6 months post-injury, if there are no signs of functional return, surgical exploration and possible nerve grafting are recommended. [4]
Neurotmesis (3rd-5th degree) nerve injury
Without surgical intervention, there is typically no recovery. [9]
Medical Management (current best evidence)[edit | edit source]
Surgery[edit | edit source]
There is uncertainty among clinicians as to the appropriate time for surgical exploration following isolated axillary nerve injury, with some authors recommending exploration at 3 months post-injury while others recommend at 6 to 12 months post-injury.[9][17] The site of the axillary nerve injury is variable, making both anterior and/or posterior surgical approaches appropriate.[4] If the axillary nerve cannot be repaired without tension, cable grafts are required. Indications for surgery are rare but must be understood by clinicians in order to maximize outcomes and minimize complications.[7]
Indications for surgery:[edit | edit source]
Suspicion of osteophyte formation or compression in the quadrilateral space.[6]
No axillary nerve recovery observed by 3 to 4 months following injury.[9]
No improvements were seen after 3 to 6 months of conservative treatment.[15]
No EMG/NCV evidence of recovery by 3 to 6 months after injury.[14]
Surgery for shoulder instability in young active patients reduces the likelihood of recurrent anterior shoulder dislocations, therefore reducing the possibility of axillary nerve compromise.[24]
In the rare occasion that surgery is indicated, there are several types of surgeries which can be considered by the patient and his surgeon.[7][14]There is a better prognosis if the surgery is performed within 6 months of the injury but functional improvements can be expected with surgical intervention up to 12 months year after the injury.[14][15] The clinician should be aware of these prognostic correlations between time of injury and time of surgery to maximize the patient's outcome. Prognosis is good in 90% of patients [4]
Surgical Procedures:[edit | edit source]
Nerve grafting The sural nerve is commonly used during nerve grafting, not only of the axillary nerve, but in other peripheral nerves injuries as well. Prognosis for the axillary nerve with graft repair is better than other peripheral nerve repairs secondary to its short length. [8][9]
Nonsurgical Reduction[edit | edit source]
Reduction eliminates the need for surgical intervention, and is followed by immobilization and physical therapy management.[25]
Immobilization for young adult males 4-6 weeks [24][25] Immobilization for older patients 7-10 days [10] Precaution should be taken during manipulative reduction of a dislocation, in which traction together with rotation or abduction are applied simultaneously, creating extra distraction and increasing the risk of axillary nerve damage. [10] Other treatments include: NSAIDS, rest, ice [6][7][17][24]
Physical Therapy Management (current best evidence)[edit | edit source]
Current research encompassing treatment and intervention of axillary nerve injuries following shoulder dislocation is limited. The research suggests that the management of the axillary nerve damage following shoulder dislocation is treated in the same manner as treating an isolated dislocation, with an emphasis on strengthening and stimulation of the deltoids and teres minor muscles.[4][13]There should be a great amount of importance placed on allowing ligamentous, capsular, and nervous tissues time to heal while preventing joint stiffness, which could ultimately hinder function greater in the long run.[7][10][13]
Non-Surgical Physical Therapy Treatment[edit | edit source]
0-2 weeks[4][10][13][16][25][26][edit | edit source]
Shoulder immobilization via sling after reduction. There is insufficient evidence to support whether physical therapy should be initiated during or after immobilization. [5]
Isometric Strengthening; Dosing: 10 seconds X 6 repetitions X 2 day within limits of pain[edit | edit source]
Shoulder(Flexion, Extension, Abduction, Adduction, Internal Rotation)
Joint Mobility:[edit | edit source]
Active Range of Motion(AROM); Dosing 10 repetitions X 2 day
Elbow(Flexion, Extension,Pronation, Supination)
Wrist (Flexion, Extension, Radial/Ulnar deviation)
Hand (Opening/Closing Fist)
2-4 weeks[edit | edit source]
Joint Mobility[edit | edit source]
Passive/Active Assisted Range of Motion(PROM/AAROM); Dosing 10 repetitions X 2 day: Shoulder (Flexion, Internal Rotation, Adduction)
Avoid end-range ER/Abd until later stages of treatment!
Active Range of Motion (AROM); Dosing 10 repetitions X 2 day: Elbow(Flexion, Extension ,Pronation, Supination); Wrist (Flexion, Extension, Radial/Ulnar deviation); Hand (Opening/Closing Fist)
Pendulum Exercises 3 sets x 30 seconds[13]
Postural/Periscapular Muscular Strengthening/Neuromuscular Re-education[9][16][25]
Strengthening of Target Muscles[13][edit | edit source]
Deltoid: “Neuromuscular electrical stimulation of the deltoid muscle can also be helpful to decrease the extent of deltoid muscle atrophy.” [1][9]
Upper/Middle/Lower Trapezius
PRECAUTION: against shoulder abduction & flexion beyond 90 degrees, and ER beyond neutral in the first 3 weeks.[13]
Older individuals have lower rates of re-occurrence of shoulder dislocation and an increase in incidence of joint stiffness. Therefore, progressive strengthening and proprioceptive training should be initiated sooner than in younger individuals, who usually begin around week 6. [6][13]
4-6 weeks[edit | edit source]
D/C sling
Strengthening Program light resistive exercises [25]
Target muscles: Deltoids, Rotator Cuff muscles, Postural muscles
Proprioceptive Techniques [13][16][25] PNF diagonals
Closed Chained Activities
Wall push-ups -->Table-->Floor
Weight Shifts
6 weeks-Discharge [3][24][27][28][edit | edit source]
Continue ROM, glenohumeral and scapulothoracic stabilization/strengthening exercises, proprioception, and joint mobility, while maintaining optimal conditions for tissue healing
Begin to initiate sport/job specific activities, progressing to full return as patient’s functional status allows
There is no consensus of when return to sport/work is appropriate following an axillary nerve injury. In general, improvement on the EMG and at least 80% return of deltoid muscle strength is recommended. [3][24]
It has been suggested that return to activity for shoulder dislocation is approximately 12 weeks, and 16 weeks for competitive sports. [27][28]
Note: Progression of these interventions with increased weight or resistance should be based on each individual patient and their level of pain and perceived joint stability throughout a controlled movement.[13]
Conservative physical therapy treatment can last between 3 to 6 months. It is essential that the physical therapist continuously monitor the progression of axillary nerve reinnervation during treatment and contact the patient’s physician if there are no signs of improvement between 3 to 4 months.[7][9]

For examples of therapeutic exercises, see Examples of Therapeutic Exercises in Axillary Nerve Injury Rehabilitation.
Post-Surgical Physical Therapy[edit | edit source]
There is a lack of research to support how long a patient should be immobilized after surgical repair of the axillary nerve. Current recommendations report that the shoulder should be immobilized for 4 to 6 weeks, after which rehabilitation should focus on increasing shoulder range of motion and strengthening. [17]
Clinical Bottom Line[1][edit | edit source]
A standardized treatment is not yet known for patients with axillary nerve injury secondary to shoulder dislocation. However, immobilization based on age, treatments focused on ROM, strength, neuromuscular re-education, and function all seem to be a recurrent theme. With early detection, prognosis for the injured axillary nerve is good due to its short length needed to regenerate.
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 Allen J, Dean K. Recognizing, managing, and testing an axillary- nerve dysfunction. Athletic Therapy Today. 2002;7(2):28-29.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 2.9 Apaydin N, Tubbs S, Loukas M, Duparc F. Review of the surgical anatomy of the axillary nerve and the anatomic basis of its iatrogenic and traumatic injury. Springer. 2010;32:193-201.
- ↑ 3.0 3.1 3.2 3.3 3.4 Cutts S, Prempeh M, Drew S. Anterior shoulder dislocation. Ann R Coll Surg Engl. 2009:91:2-7.
- ↑ 4.00 4.01 4.02 4.03 4.04 4.05 4.06 4.07 4.08 4.09 4.10 4.11 4.12 4.13 4.14 4.15 4.16 4.17 4.18 Duralde X. Neurologic injuries in the athlete’s shoulder. Journal of Athletic Training. 2000;35(3):316-328.
- ↑ 5.0 5.1 5.2 5.3 5.4 Handoll HHG, Hanchard NCA, Goodchild LM, Feary J. Conservative management following closed reduction of traumatic ; anterior dislocation of the shoulder (review). Cochrane Database of Systematic Review. 2006;1:1-26.
- ↑ 6.00 6.01 6.02 6.03 6.04 6.05 6.06 6.07 6.08 6.09 6.10 6.11 6.12 6.13 6.14 6.15 6.16 Miller T. Peripheral nerve injuries at the shoulder. The Journal of Manipulative Therapy. 1998;6(4)170-183.
- ↑ 7.00 7.01 7.02 7.03 7.04 7.05 7.06 7.07 7.08 7.09 7.10 7.11 7.12 7.13 7.14 7.15 Neal S, Fields K. Peripheral nerve entrapment and injury in the upper extremity. American Family Physician. 2010; 81(2): 147-155.
- ↑ 8.00 8.01 8.02 8.03 8.04 8.05 8.06 8.07 8.08 8.09 8.10 Payne M, Doherty T, Sequeira K, Miller T. Peripheral nerve injury associated with shoulder trauma: a retrospective study and review of literature. Journal of Clinical Neuromuscular Disease. 2002; 4(1): 1-6.
- ↑ 9.00 9.01 9.02 9.03 9.04 9.05 9.06 9.07 9.08 9.09 9.10 9.11 9.12 9.13 9.14 9.15 9.16 9.17 9.18 9.19 9.20 9.21 9.22 9.23 9.24 9.25 9.26 9.27 Perlmutter G, Apruzzese W. Axillary nerve injuries in contact sports: recommendations for treatment and rehabilitation. Sports Med. 1998;26(5): 351-360.
- ↑ 10.00 10.01 10.02 10.03 10.04 10.05 10.06 10.07 10.08 10.09 10.10 10.11 10.12 Visser C, Coene L, Brand R, Tavy D. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery a prospective clinical and emg study. Journal of Bone and Joint Surgery. British volume. 1999; 81-B(4). 679-685.
- ↑ Cox C, Kuhn J. Operatice versus nonoperative treatment of acute shoulder dislocation in the athlete. Current Sports Medicine Reports. 2008;7(5): 263-268.
- ↑ McFarland E, Caicedo J, Kim T, Banchasuek P. Axillary nerve injury in anterior shoulder reconstructions: use of a subscapularis muscle- splitting technique and a review of the literature. Am J Sports Med. 2002;30:601-606.
- ↑ 13.00 13.01 13.02 13.03 13.04 13.05 13.06 13.07 13.08 13.09 13.10 13.11 Kazemi M. Acute traumatic anterior glenohumeral dislocation complicated by axillary nerve damage: a case report. Journal of the Canadian Chiropractic Association. 1998;42(3):150-155.
- ↑ 14.00 14.01 14.02 14.03 14.04 14.05 14.06 14.07 14.08 14.09 14.10 14.11 Safran M. Nerve injury about the shoulder in athletes, Part 1: Suprascapular nerve and axillary nerve. Am J Sports Med . 2004;32(3):803-819.
- ↑ 15.00 15.01 15.02 15.03 15.04 15.05 15.06 15.07 15.08 15.09 15.10 Vitanzo P, Kenneally B. Diagnosis of isolated axillary neuropathy in athletes:case studies. The Journal of Musculoskeletal Medicine. 2009; 26:307-311.
- ↑ 16.00 16.01 16.02 16.03 16.04 16.05 16.06 16.07 16.08 16.09 16.10 Miller T. Axillary neuropathy following traumatic dislocation of the shoulder: a case study. The Journal of Manual & Manipulative Therapy. 1998;6(4):184-185.
- ↑ 17.0 17.1 17.2 17.3 17.4 17.5 17.6 17.7 17.8 17.9 Manske R, Sumler A, Runge J. Quadrilateral space syndrome. Humen Kinetics-ATTI.2009;14(2):45-47.
- ↑ 18.0 18.1 Mamula C, Erhard R, Piva S. Cervical radiculopathy or parsonage-turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. Journal of Orthopaedic Sports Physical Therapy. 2005; 55(10): 659-664.
- ↑ 19.0 19.1 Hertel R, Lambert SM, Ballmer FT. The deltoid extension lag sign for diagnosis and grading of axillary nerve palsy. J Shoulder & Elbow Surgery 1998;7(1):97-108.
- ↑ Wainner R, Fritz J, Irrgang J, Boninger M, Delitto A, Allison S. Reliability and diagnositic accuracy of the clinical examination and patient self report measures for cervical radiculopathy. SPINE. 2003; 28(1):52-62.
- ↑ Park H, Yokota A, Gill H, Rassi G, McFarland E. Diagnostic accuracy of clinical tests for the differential degrees of subacromial impingement syndrome. The Journal of Bone and Joint Surgery. 2005;87-A(7): 1446-1455.
- ↑ Chernchujit, B. Sulcus Sign Shoulder Dislocation Instability Examination [Video]. YouTube. http://www.youtube.com/watch?v=cTDoZo3HPz4. Published May 18, 2008. Accessed November 28, 2010
- ↑ Apprehension Test [Video]. YouTube. http://www.youtube.com/watch?v=gLBX8vUnCo0. Published June 2, 2007. Accessed November 28, 2010.
- ↑ 24.0 24.1 24.2 24.3 24.4 Handoll HHG, Al-Maiyah MA. Surgical versus non-surgical treatment for acute anterior shoulder dislocation.Cochrane Database of Systematic Review. 2004;1:1-37.
- ↑ 25.0 25.1 25.2 25.3 25.4 25.5 Deyle G, Nagel K. Prolonged immobilization in abduction and neutral rotation for a first-episode anterior shoulder dislocation. Journal of orthopedic sports physical therapy. 2007; 37(4): 192-198.
- ↑ Gibson K, Growse A, Korda L, Wray E, MacDermid J. The effectiveness of rehabilitation for nonoperative management of shoulder instability: a systematic review. Journal of Hand Therapy. 2004; 17(2): 229-242
- ↑ 27.0 27.1 Robinson M, Howes J, Murdoch H, Will E. Graham C. After primary traumatic anterior shoulder dislocation in young patients. The Journal of Bone Surgery. 2006;88(11): 2326-2336.
- ↑ 28.0 28.1 Mahaffey B, Smith P. Shoulder instability in young athletes. American Family Physician. 1999;59(10): 2773-2782.


{kind=link}