Assessment of Overuse Injury in Runners: Difference between revisions
No edit summary |
No edit summary |
||
| Line 133: | Line 133: | ||
* The [[Visual Analogue Scale|visual analogue scale]] for quantifiable feedback on symptoms | * The [[Visual Analogue Scale|visual analogue scale]] for quantifiable feedback on symptoms | ||
* The [[Borg Rating Of Perceived Exertion|Borg scale]] for perceived exertion is used to quantify the perceived working load or intensity of a run<ref>Benson LC, Owoeye O, Räisänen AM, Stilling C, Edwards WB, Emery CA. Magnitude, Frequency, and Accumulation: Workload Among Injured and Uninjured Youth Basketball Players. Frontiers in Sports and Active Living. 2021 Apr 6;3:49.</ref> | * The [[Borg Rating Of Perceived Exertion|Borg scale]] for perceived exertion is used to quantify the perceived working load or intensity of a run<ref>Benson LC, Owoeye O, Räisänen AM, Stilling C, Edwards WB, Emery CA. Magnitude, Frequency, and Accumulation: Workload Among Injured and Uninjured Youth Basketball Players. Frontiers in Sports and Active Living. 2021 Apr 6;3:49.</ref> | ||
<gallery widths=" | <gallery widths="350px" heights="350px"> | ||
File:Adapted VAS.png|Visual Analogue Scale | File:Adapted VAS.png|Visual Analogue Scale | ||
File:Borg Rating of Perceived Exertion.png|Borg Rating of Perceived Exertion </gallery> | File:Borg Rating of Perceived Exertion.png|Borg Rating of Perceived Exertion </gallery> | ||
Revision as of 17:01, 29 March 2022
This article or area is currently under construction and may only be partially complete. Please come back soon to see the finished work! (29/03/2022)
Original Editor - Wanda van Niekerk based on the course by Merike Hopkins
Top Contributors - Wanda van Niekerk, Kim Jackson, Jess Bell, Lucinda hampton, Aminat Abolade and Ewa Jaraczewska
Introduction[edit | edit source]
Running is a popular physical activity all over the world.[1] The benefits of running include: improved endurance, decreased risk of cardiovascular disease and weight loss. In recent years the number of runners has increased. In the United States 15% of the population take part in some form of running and in the UK statistics show that 6 million people run once a week. Unfortunately, there is also the risk of injury. Approximately 80% of running-related injuries are related to overload.[2] Structures that are slow at adaptation to training load such as tendons and ligaments are mainly at risk of injury.[3]
Assessment and Treatment Continuum[edit | edit source]
Assessment is always a process, especially in managing overuse injuries. The assessment process is tailormade in an optimal way and continues throughout the rehabilitation process until the patient/athlete is discharged and fully functional.[4] The diagram below indicates the progression in the assessment and treatment continuum.

Overuse Injury in Runners[edit | edit source]
Definition of Overuse Injury[edit | edit source]
Overuse injuries are characterised by the absence of a single, identifiable or traumatic cause. There is a gradual onset and injury is caused by repeated micro-trauma.[5] The term "overuse" is used as the onset of these type of injuries are usually precipitated by a period of inappropriate tissue loading such as:[6]
- Excessive magnitude or volume of load
- Insufficient recovery between bouts of load
Why Does Overuse Lead to Injury?[edit | edit source]
An overuse injury is usually caused by repetitive activities over a period of time. This repetitive microtrauma overloads the capacity of the tissue to repair itself.[6] During exercise, the various tissues such as muscles, tendons, bones and ligaments, are being loaded and experience excessive physiological stress. After the specific exercise activity, the tissues undergo adaptation in order to strengthen and to be able to withstand similar stress in the future. If the adaptive capability of a specific tissue type is exceeded and injury occurs, this is most often an overuse injury. Therefore, in overzealous athletes, that do not allow adequate time for adaptation to occur before the next workout or training session, the cumulative tissue damage eventually exceeds the threshold that the tissue can handle and this causes pain and dysfunction.[6]
Read more about overuse injury:
Running Surfaces and Overuse Injury[edit | edit source]
Surface also plays a role in overuse injuries in running. The common misconception is that running on a softer surface will reduce impact and therefore reduce the risk of injury. However, different running surfaces will simply change the biomechanical demands on the body. For instance, running on softer surface will reduce impact loading rates, but there will be an increased demand on musculoskeletal structures such as muscles and tendons. A change in running surface may reduce stress on one area of the body, but it may increase injury risk in other areas.[7]
Patient Education and Overuse Injury[edit | edit source]

A helpful imagery to use in educating patients about their overuse injury is the image of two tugboats pulling against each other.[4] The green tugboat (good) will drive the overuse injury into healing and return to function or sport, whereas the red tugboat will draw the overuse injury away from healing and into more serious pathology. The key is to find the balance and fuelling the green tugboat with all the necessary interventions to facilitate healing, but not in a way that fuels the red tugboat and aggravates the pathology.[4]
Read more here: Physiotherapy and Overuse Injuries
Common Overuse Injuries in Runners[edit | edit source]
Overuse injuries commonly affect the knee, lower limb and foot in runners. In elite middle- and long-distance runners, the majority of injuries are in the lower leg and foot[8], whereas in recreational runners the most frequent area of injury is the knee.[9] Some of the common overuse injuries in runners include[7]:
- Medial tibial stress syndrome
- Posterior compartment syndrome
- Patellofemoral pain syndrome (Runner's knee)
- Achilles tendinopathy
- Peroneal tendinopathy
- Iliotibial band syndrome
- Hamstring tendinopathy
- Proximal Hamstring Tendinopathy
- Bursitis
- Plantar heel pain
- Calf muscle strain injuries
- Bone stress injuries
- For example a stress fracture of the tibia
- Other stress fracture sites: anterior tibial diaphysis, 5th metatarsal base, medial malleoli, lateral femoral neck, tarsal navicular, great toe sesamoid[10]
- Osgood Schlatter Disease (in younger athletes)
- Sever’s Disease (in younger athletes)
Even though it is useful to know all the common injuries of running, it is still crucial to have a systematic assessment of your runner and to follow the process in order the make the correct diagnosis.[4]
Subjective Assessment/Clinical History[edit | edit source]
Clinical Reasoning[edit | edit source]
Factors to consider in the clinical reasoning process:
- The importance of understanding work load and how that relates to mechanical load[11]
- Knowledgeable about common injuries
- Understand risk/predisposing factors that can influence injury
- Don’t arrive at a conclusion too soon – keep an open mind in your assessment
- Gradual onset may be a clue, but some overuse injuries can have an acute onset
- Look out for underlying medical conditions and red flags to clear
- Good anatomy and pathophysiology knowledge is necessary
- Consider biomechanics such as:
- The mechanism of injury
- Intrinsic and Extrinsic forces on structures
- Surface
- Shoes
Subjective Clinical History Considerations[edit | edit source]
- Listen well, but also ask crucial important questions
- Specifically ask about the runner’s volume of load and the intensity of load and any changes in these and document this very well and reassess regularly
- Consider not only the influences of forces when running, but also in activities of daily living and other sports or recreational activities
- Medical or general history
- Be aware of possible red flags and refer to members of the multi-disciplinary team
Predisposing/Risk factors[edit | edit source]
Common predisposing risk factors to consider:
- Age
- Increased age may be a risk factor for certain types of running-related injuries[12]
- Biological Sex
- Low quality evidence exist indicating that men are at higher risk of running-related injuries[12]
- Running experience
- Previous injury
- Load
- Lower running volume is a risk factor for overuse injuries among short-distance runners[1]
- Footwear
- The biomechanical stress placed on certain structures during running is influenced by the type of running shoe, but there is not evidence to show that a particular shoe will influence injury risk[7]
- Running surface
- Sudden changes in running surface may be a risk factor[7]
Investigating the Injury[edit | edit source]
- Be as specific and quantitative as possible[4]
- Questions to ask regarding the injury:
- Location of pain - Where does it hurt?
- Nature of pain - Type of pain
- Intensity of the pain
- Frequency of pain
- When did pain start – try and get specific answers
- Does it hurt with every run/every week/every month
- How far into the run does the pain start
- Does the pain get better when runner warms up
- Does the pain come back?
- Questions about activities of daily living and normal training routines
- Outcome measures such as the VISA -A scale for Achilles tendinopathy is a useful tool that can easily be administered
Consider that certain structures react in certain ways. For example, in tendinopathies the pain subsides after warming up and if severe enough the pain will return later in the run. In a runner with posterior compartment syndrome, the pain will progressively get worse with added symptoms such as pins and needles (paraesthesia). A bone stress injury will present as localised pain that gets worse over time.[4]
Volume Tool[edit | edit source]
- This can provide a visual aspect for your patients and is an easy to use tool.
- This tool is utilised to quantify symptoms and systematically report volume, intensity (speed or hill training) for serial reassessment.
- Patient education is key and with the assessment of overuse injuries we rely strongly on the feedback from the patient to monitor the progress. It is therefore advisable to make it easy to interpret feedback for both the clinician as well as the patient.
- With this tool, answers to the questions guiding the physiotherapist to a working diagnosis are quantified where possible and this helps to monitor progress on the road to recovery.
The volume tool makes use of other validated outcome measures:
- The visual analogue scale for quantifiable feedback on symptoms
- The Borg scale for perceived exertion is used to quantify the perceived working load or intensity of a run[16]
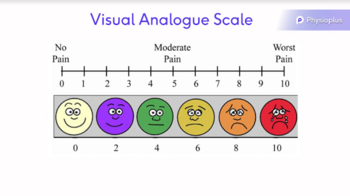
Visual Analogue Scale

Borg Rating of Perceived Exertion


- The first part of the volume tool consists out of a few questions in table form that runners can log their daily run, the distance of the run, the time in the run when symptoms start and if/when symptoms reduce, as well as the intensity of the run.
- With the volume tool - there are some constants that should be kept the same. These are the volume of the run, the surface of the run and the duration of the run. This way the body's reaction to the same volume of load can be assessed and a trend towards improvement or decline will easily be detected.

- The volume tool can then be further individualised with specific questions
- Individualised volume tool
- Questions that are included in the serial assessment/volume tool:
- Did you have discomfort in affected area on getting up and if so, please rate it on VAS 1-10.
- How many minutes did you feel discomfort?
- When did you first feel discomfort in your run, please indicate as time in minutes into your run?
- How many minutes of discomfort?
- How bad was this first symptoms at its worst on VAS 1-10
- How many minutes did you run without comfortably without symptoms before symptoms returned?
- How bad was second bout of discomfort at its worst on VAS 1-10
- How hard was your run BORG?
- How long did you run in minutes?
- Patients keep a daily log with this volume tool. If possible, try and keep some constants such as the volume of the run, the surface and the duration of the run.
- Did you have discomfort in affected area on getting up and if so, please rate it on VAS 1-10.
- Questions that are included in the serial assessment/volume tool:
- Individualised volume tool

Asking these specific questions and tracking the nature of the pain with the daily log will provide a good overview of how the injured structure behaves. Keep in mind that as part of the physical examination certain structures will be evaluated in more detail to confirm the diagnosis. However, overuse injuries can be challenging and there may be situations where the patient’s pain/ symptoms cannot be elicited in the assessment. Think about experienced runners starting to complain of a slight niggle during their run. In these cases, it may be useful to use a treadmill or to ask the patient to go for a run before or during the assessment to try and find a comparable sign. When applying these methods though, bear in mind that overuse injuries are surface dependent and that a change in the runner’s normal running surface may aggravate the issue.[4]
All the answers in the Individualised Volume Tool have a numerical value as an answer and will be transferred into a excel table and provide graph representing these values as a function to show the trend of symptoms in relation to volume, intensity over time. This tool can assist in clinical reasoning for progression in optimal sport-specific loading for running.[4]
It is a visual representation of how one parameter that influence overuse, influence the symptoms of the injury over time. It is a helpful assessment and re-assessment tool both for clinicians as well as an educational tool to help patients provide their physiotherapists with high quality valid useful feedback to use in clinical reasoning to establish a diagnosis and to plan intervention for treatment and rehabilitation. In other words, the tool helps us better understand what patient specific optimal load is at the specific moment.[4]
Developing a Working Diagnosis[edit | edit source]
| Area | Complaints by runner | Possible structure involved | Possible diagnosis |
|---|---|---|---|
| Lower Leg |
|
Bone | Bone stress reaction or stress fracture |
| Lower Leg |
|
Tendons and ligaments | Tendinopathy |
| Lower Leg |
|
Muscle, nerve, fascia | Posterior compartment syndrome |
| Knee |
|
Iliotibial band syndrome | |
| Knee |
|
Patellofemoral pain syndrome | |
| Foot and Ankle |
|
Sever's Disease |
Resources[edit | edit source]
- bulleted list
- x
or
- numbered list
- x
References[edit | edit source]
- ↑ 1.0 1.1 1.2 van Poppel D, van der Worp M, Slabbekoorn A, van den Heuvel SS, van Middelkoop M, Koes BW, Verhagen AP, Scholten-Peeters GG. Risk factors for overuse injuries in short-and long-distance running: A systematic review. Journal of sport and health science. 2021 Jan 1;10(1):14-28.
- ↑ Hespanhol Junior LC, Van Mechelen W, Verhagen E. Health and economic burden of running-related injuries in Dutch trailrunners: a prospective cohort study. Sports Medicine. 2017 Feb;47(2):367-77.
- ↑ Walther M, Reuter I, Leonhard T, Engelhardt M. Injuries and response to overload stress in running as a sport. Der Orthopade. 2005 May 1;34(5):399-404.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 4.7 4.8 4.9 Hopkins, M. Assessment of overuse injury in runners. Physioplus, Course. 2022.
- ↑ Chéron C, Le Scanff C, Leboeuf-Yde C. Association between sports type and overuse injuries of extremities in adults: a systematic review. Chiropractic & manual therapies. 2017 Dec;25(1):1-0.
- ↑ 6.0 6.1 6.2 Clarsen B. Overuse injuries in sport: development, validation and application of a new surveillance method.(dissertation). Oslo Sports Trauma Research Centre. Norwegian School of Sports Sciences. 2015
- ↑ 7.0 7.1 7.2 7.3 Bramah CA. Common Overuse Injuries in Runners and Injury Risk Factors. InThe Science and Practice of Middle and Long Distance Running 2021 Mar 29 (pp. 28-46). Routledge.
- ↑ Edouard P, Navarro L, Branco P, Gremeaux V, Timpka T, Junge A. Injury frequency and characteristics (location, type, cause and severity) differed significantly among athletics (‘track and field’) disciplines during 14 international championships (2007–2018): implications for medical service planning. British journal of sports medicine. 2020 Feb 1;54(3):159-67.
- ↑ Kluitenberg B, van Middelkoop M, Smits DW, Verhagen E, Hartgens F, Diercks R, van der Worp H. The NL start2run study: Incidence and risk factors of running‐related injuries in novice runners. Scandinavian journal of medicine & science in sports. 2015 Oct;25(5):e515-23
- ↑ Greg A J Robertson and Alexander M Wood; Lower limb stress fractures in sport: Optimising their management and outcome; World Journal Orthop. 2017 Mar 18; 8(3): 242–255.
- ↑ Lauren C. Benson, Oluwatoyosi B. A. Owoeye,Anu M. Räisänen, Carlyn Stilling, W. Brent Edwards, and Carolyn A. Emery; Magnitude, Frequency, and Accumulation: Workload Among Injured and Uninjured Youth Basketball Players; Front Sports Act Living. 2021; 3: 607205.
- ↑ 12.0 12.1 12.2 Van der Worp MP, Ten Haaf DS, van Cingel R, de Wijer A, Nijhuis-van der Sanden MW, Staal JB. Injuries in runners; a systematic review on risk factors and sex differences. PloS one. 2015 Feb 23;10(2):e0114937.
- ↑ Kemler E, Blokland D, Backx F, Huisstede B. Differences in injury risk and characteristics of injuries between novice and experienced runners over a 4-year period. The Physician and sportsmedicine. 2018 Oct 2;46(4):485-91
- ↑ Linton L, Valentin S. Running with injury: A study of UK novice and recreational runners and factors associated with running related injury. Journal of science and medicine in sport. 2018 Dec 1;21(12):1221-5
- ↑ Hulme A, Nielsen RO, Timpka T, Verhagen E, Finch C. Risk and protective factors for middle-and long-distance running-related injury. Sports Medicine. 2017 May;47(5):869-86
- ↑ Benson LC, Owoeye O, Räisänen AM, Stilling C, Edwards WB, Emery CA. Magnitude, Frequency, and Accumulation: Workload Among Injured and Uninjured Youth Basketball Players. Frontiers in Sports and Active Living. 2021 Apr 6;3:49.

