Iliocostalis Lumborum: Difference between revisions
No edit summary |
Abbey Wright (talk | contribs) No edit summary |
||
| Line 7: | Line 7: | ||
== Description == | == Description == | ||
[[Image:250px-Iliostalis.png|iliocostalis | [[Image:250px-Iliostalis.png|Image 1: Deep muscles of the back. (Iliocostalis lumborum visible at bottom right, iliocostalis dorsi visible at centre)|alt=|frame]] | ||
Iliocostalis is a dorsal [[muscle]] situated deep to the fleshy section of [[Serratus Anterior|serratus anterior.]] Iliocostalis lumborum is the lower (lumbar) portion of that muscle. | Iliocostalis is a dorsal [[muscle]] situated deep to the fleshy section of [[Serratus Anterior|serratus anterior.]] Iliocostalis lumborum is the lower (lumbar) portion of that muscle. | ||
Iliocostalis lumborum is part of the [[Erector Spinae|erector spinae]] muscle group which includes iliocostalis, [[Longissimus Thoracis|longissimus]], and [[Spinalis Thoracis|spinalis]]. The muscle bulk formed by this muscle group can be felt running parallel to the spine over the transverse processes of each vertebra. These muscles are vital for allowing free movement of the spine. | |||
Injury to iliocostalis lumborum may be indicated by [[Pain Behaviours|pain]] concentrated in the lower back or pain in the buttocks. Common daily activities may cause injury to the muscle including lifting a heavy object, rotating while lifting, or even sitting immobile for extended periods of time. | |||
Injury to iliocostalis lumborum may be indicated by [[Pain Behaviours|pain]] concentrated in the lower back or pain in the buttocks. Common daily activities may cause injury to the muscle including lifting a heavy object, rotating while lifting, or even sitting immobile for extended periods of time | |||
If there is a significant discrepancy between the strength of the [[Abdominal Muscles|abdominal muscles]] and the lumbar muscles of the back, it may result in a condition known as [[Low Back Pain Related to Hyperlordosis|lumbar hyperlordosis]]. This condition can be successfully reversed through targeted [[Stretching|stretches]] and [[Exercises for Lumbar Instability|exercises]] aimed at strengthening the deficient muscles.<ref>rehab my patients Iliocostalis Lumborum Available: https://www.rehabmypatient.com/lumbar-spine/iliocostalis-lumborum (accessed 1.12.2021)</ref> | If there is a significant discrepancy between the strength of the [[Abdominal Muscles|abdominal muscles]] and the lumbar muscles of the back, it may result in a condition known as [[Low Back Pain Related to Hyperlordosis|lumbar hyperlordosis]]. This condition can be successfully reversed through targeted [[Stretching|stretches]] and [[Exercises for Lumbar Instability|exercises]] aimed at strengthening the deficient muscles.<ref>rehab my patients Iliocostalis Lumborum Available: https://www.rehabmypatient.com/lumbar-spine/iliocostalis-lumborum (accessed 1.12.2021)</ref> | ||
Revision as of 13:49, 1 December 2021
Original Editor - Oyemi Sillo
Lead Editors - Vidya Acharya, Oyemi Sillo, Kim Jackson, Abbey Wright, Lucinda hampton, Evan Thomas, WikiSysop and 127.0.0.1
Description[edit | edit source]

Iliocostalis is a dorsal muscle situated deep to the fleshy section of serratus anterior. Iliocostalis lumborum is the lower (lumbar) portion of that muscle.
Iliocostalis lumborum is part of the erector spinae muscle group which includes iliocostalis, longissimus, and spinalis. The muscle bulk formed by this muscle group can be felt running parallel to the spine over the transverse processes of each vertebra. These muscles are vital for allowing free movement of the spine.
Injury to iliocostalis lumborum may be indicated by pain concentrated in the lower back or pain in the buttocks. Common daily activities may cause injury to the muscle including lifting a heavy object, rotating while lifting, or even sitting immobile for extended periods of time.
If there is a significant discrepancy between the strength of the abdominal muscles and the lumbar muscles of the back, it may result in a condition known as lumbar hyperlordosis. This condition can be successfully reversed through targeted stretches and exercises aimed at strengthening the deficient muscles.[1]
Anatomy[edit | edit source]
Origin[edit | edit source]
- Anterior surface of a broad and thick tendon w attached to the medial crest of the sacrum,
- Spinous processes of the lumbar vertebrae,
- 11th and 12th thoracic vertebrae,
- Posterior part of the medial lip of iliac crest, supra-spinous ligament and the lateral crest of sacrum[2].
Insertion[edit | edit source]
By tendons into inferior borders of the angles of the lower 6 or 7 ribs[2]
Nerve Supply[edit | edit source]
Dorsal rami of thoracic and lumbar spinal nerves (T7 to L3)[3]
Blood Supply[edit | edit source]
Dorsal branches of the lumbar arteries from the aorta. Dorsal branches of the lateral sacral artery from the internal iliac artery.[3]
Muscle Fibre[edit | edit source]
Characterised by Type 1 muscle fibre, indicating the tonic holding and stabilisation function.[4]
Action[edit | edit source]
- Extension of Spine: Acting bilaterally, extension and hyperextension of the spine. Acting unilaterally, laterally flexes the spine[5]
- Respiration: It assists as an accessory muscle of expiration, due to its insertion on the ribs[6]
- Stabilization of Spine: Iliocostalis lumborum along with multifidus contribute to support and control the orientation of lumbar spine.[4]
Clinical Relevance:[edit | edit source]
- Myofascial pain[7] of Iliocostalis Thoracis- Lumborum muscle causes anterior torso pain. The pain of myofascial origin is a well-recognized pathology characterized by the presence of two components: referred pain; which is often distant from its source and specific to each muscle, and the trigger point, a localized hyperirritable band present in the affected muscle and able to reproduce the referred pain when stimulated. The most common locations of pain were the right-lower quadrant and the left side of the chest. Unsurprisingly, since the referred pain of myofascial pain of the Iliocostalis muscle is located at the frontal aspect of the torso (chest, abdomen, and pelvis), it is a clinical challenge even to seasoned clinicians. The anterior torso pain often results in extensive workups before Iliocostalis Lumborum myofascial pain diagnosis is made. Trigger point injections are diagnostic and therapeutic of Iliocostalis Thoracis-Lumborum myofascial pain.
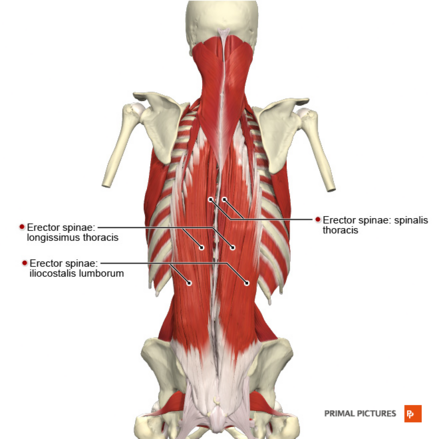

Image R: Muscles of the back erector spinae group
- Investigative studies like EMG[8] have shown the involvement of Iliocostalis Lumborum along with external obliques in Pisa Syndrome, which is defined as a reversible lateral bending of the trunk with a tendency to lean to one side[9]. This is a frequent and often disabling complication of Parkinson's. As some forms of Pisa syndrome are potentially reversible, there is growing consensus on the importance of its early recognition and the importance of pharmacological adjustment and rehabilitation.[10]
Assessment[2][edit | edit source]
Power
- Position: Prone with hands clasped behind buttocks or head.
- Fixation: Examiner must stabilize the legs firmly on the table.
- Test: Trunk extension
Pressure: If performed with hands behind back no pressure is needed.
Weakness
- Bilateral weakness of low back muscles results in a lumbar kyphosis and increased thoracic kyphosis.
- Unilateral weakness results in lateral curvature with convexity towards the weak side.
Length
- Bilateral contracture of low back muscles results in lordosis.
- Unilateral contracture results in scoliosis with convexity to the opposite side.
Treatment[edit | edit source]
Strengthening exercises:[edit | edit source]
1. Prone extension exercise[11]:
a) In prone lying, have the patient tuck in the chin and lift the head, thorax of the plinth.
b) To progress further, the patient can vary the arm position. Resistance can be added by using hand-held weights.
c) Patient can further progress by lifting one leg off the mat alternately, and progress to both legs simultaneously.
d) Further progression can be made - spine extension with both upper limbs and lower limbs lifted off the mat.
2. Prone exercises on a stability ball.
3. Plank and quadruped exercises to develop control and strength in spinal extensors.
4.Postural exercises.
Stretching exercises:[edit | edit source]
Trunk lateral bending exercises to the opposite side of tightness and flexion exercises help in stretching the tight muscles.
References[edit | edit source]
- ↑ rehab my patients Iliocostalis Lumborum Available: https://www.rehabmypatient.com/lumbar-spine/iliocostalis-lumborum (accessed 1.12.2021)
- ↑ 2.0 2.1 2.2 Muscle Testing and Function;4th Edition; Kendall, McCreary, Provance; Page No.138.
- ↑ 3.0 3.1 Anatomy EXPERT; Iliocostalis lumborumhttp://www.anatomyexpert.com/app/structure/5243/ (accessed on 2.07.18)
- ↑ 4.0 4.1 Therapeutic Exercise for Spine Segmental Stabilization in Low Back Pain; Richardson, Jull, Hodges, Hides; Scientific Basis; Page No.24.
- ↑ Wheeless Textbook of Orthopaedics; Iliocostalis Lumborum http://www.wheelessonline.com/ortho/iliocostalis_lumborum_1 (accessed on 2.07.18)
- ↑ Muscles Testing and Function;4th Edition; Kendall, McCreary, Provance; Accessory Muscles of Respiration, Page No.330.
- ↑ Roldan CJ, Huh BK. Iliocostalis Thoracis-Lumborum Myofascial Pain: Reviewing a Subgroup of a Prospective, Randomized, Blinded Trial. A Challenging Diagnosis with Clinical Implications. Pain physician. 2016 Aug 1;19:363-72.https://www.ncbi.nlm.nih.gov/pubmed/27454266
- ↑ Geroin C, Squintani G, Morini A, Donato F, Smania N, Gandolfi M, Tamburin S, Fasano A, Tinazzi M. Pisa syndrome in Parkinson’s disease: electromyographic quantification of paraspinal and non-paraspinal muscle activity. Functional neurology. 2017 Jul;32(3):143.https://www.ncbi.nlm.nih.gov/pubmed/29042003
- ↑ Barone P, Santangelo G, Amboni M, Pellecchia MT, Vitale C. Pisa syndrome in Parkinson's and parkinsonism: clinical features, pathophysiology, and treatment. The Lancet Neurology. 2016 Sep 1;15(10):1063-74.https://www.ncbi.nlm.nih.gov/pubmed/27571158
- ↑ Tinazzi M, Geroin C, Gandolfi M, Smania N, Tamburin S, Morgante F, Fasano A. Pisa syndrome in Parkinson's: An integrated approach from pathophysiology to management. Movement Disorders. 2016 Dec 1;31(12):1785-95.https://www.ncbi.nlm.nih.gov/pubmed/27779784
- ↑ Therapeutic Exercise; Third Edition; Kisner & Colby; The Spine: Subacute, Chronic, and Postural Problems; Page No.562

