Meniere's Disease: Difference between revisions
No edit summary |
No edit summary |
||
| (19 intermediate revisions by 4 users not shown) | |||
| Line 1: | Line 1: | ||
<div class="editorbox"> | <div class="editorbox"> | ||
'''Original Editors '''-[[User:Elaine Lonnemann|Elaine Lonnemann]] | '''Original Editors '''-[[User:Elaine Lonnemann|Elaine Lonnemann]] | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
</div> | |||
</div> | |||
== Introduction == | == Introduction == | ||
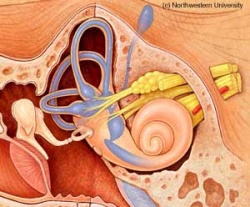
[[File:Ear Anatomy.png|Blausen.com staff (2014). &quot;Medical gallery of Blausen Medical 2014"|right|frameless]]Meniere disease (or idiopathic endolymphatic hydrops) is a disorder of the inner ear characterized by hearing loss, [[tinnitus]], and vertigo. It is named after the French physician Prosper Ménière (1799-1862) who first recognised vertigo as an inner ear disorder. | [[File:Ear Anatomy.png|Blausen.com staff (2014). &quot;Medical gallery of Blausen Medical 2014"|right|frameless]]Meniere disease (or idiopathic endolymphatic hydrops) is a disorder of the inner ear characterized by hearing loss, [[tinnitus]], and [[vertigo]]. It is named after the French physician Prosper Ménière (1799-1862) who first recognised vertigo as an inner ear disorder. | ||
* In most cases, it is slowly progressive and has a significant impact on the social functioning of the individual affected. | * In most cases, it is slowly progressive and has a significant impact on the social functioning of the individual affected. | ||
* | * It is an inner ear disorder and as such can affect balance and hearing<ref name=":1">Radiopedia [https://radiopaedia.org/articles/meniere-disease Meniere Disease] Available from:https://radiopaedia.org/articles/meniere-disease (last accessed 2.8.2020)</ref>. | ||
* Primarily a unilateral disorder, however, the opposite ear can be affected in 2-50% of people diagnosed with Meniere's disease.<ref name="Goodman">Goodman CC, Fuller KS. Pathology: implications for the physical therapist. St. Louis, MO: Elsevier Saunders; 2015; pp 1055-1069.</ref> | * Primarily a unilateral disorder, however, the opposite ear can be affected in 2-50% of people diagnosed with Meniere's disease.<ref name="Goodman">Goodman CC, Fuller KS. Pathology: implications for the physical therapist. St. Louis, MO: Elsevier Saunders; 2015; pp 1055-1069.</ref> | ||
The 2 minute 45 second video below fives a good summary{{#ev:youtube|v=qrk7OyAB_ss}}<ref>Fauquier ENT Meniere's Disease - What Happens in the Inner Ear?Available from https://www.youtube.com/watchv=qrk7OyAB_ss</ref> | The 2 minute 45 second video below fives a good summary{{#ev:youtube|v=qrk7OyAB_ss}}<ref>Fauquier ENT Meniere's Disease - What Happens in the Inner Ear?Available from https://www.youtube.com/watchv=qrk7OyAB_ss</ref> | ||
== | == Epidemiology == | ||
The prevalence of Meniere disease varies between 3.5 per 100.000 and 513 per 100.000 and occurs more often in older, white and female patients. | The prevalence of Meniere disease varies between 3.5 per 100.000 and 513 per 100.000 and occurs more often in older, white and female patients. | ||
The identification of several comorbidities which occur in an increased fashion in patients with Meniere disease gave rise to new theories about the origins of the disease. | The identification of several comorbidities which occur in an increased fashion in patients with Meniere disease gave rise to new theories about the origins of the disease. | ||
* [[Migraine Headache|Migraine]]: Migraine occurs more often in patients diagnosed with Meniere disease although there might be an overlap between basilar migraine wrongly diagnosed as Meniere disease. | * [[Migraine Headache|Migraine]]: Migraine occurs more often in patients diagnosed with Meniere disease although there might be an overlap between basilar migraine wrongly diagnosed as Meniere disease. | ||
* [[Autoimmune Disorders|Autoimmune Disease]]<nowiki/>s: Several autoimmune diseases are associated with Meniere disease namely [[Rheumatoid Arthritis|rheumatoid arthritis]], [[Systemic Lupus Erythematosus|systemic lupus erythematosus]] and [[Ankylosing Spondylitis|ankylosing spondylitis]] | * [[Autoimmune Disorders|Autoimmune Disease]]<nowiki/>s: Several autoimmune diseases are associated with Meniere disease namely [[Rheumatoid Arthritis|rheumatoid arthritis]], [[Systemic Lupus Erythematosus|systemic lupus erythematosus]] and [[Ankylosing Spondylitis (Axial Spondyloarthritis)|ankylosing spondylitis]] | ||
== Etiology == | == Etiology == | ||
| Line 26: | Line 28: | ||
* Although considered to be idiopathic, there is an association with inner ear effusions and endolymphatic hydrops<ref name=":1" />. | * Although considered to be idiopathic, there is an association with inner ear effusions and endolymphatic hydrops<ref name=":1" />. | ||
[[File:Engorged.jpg|right|frameless|250x250px]] | [[File:Engorged.jpg|right|frameless|250x250px]] | ||
<ref name="Dizziness" /><br> Images R Normal Labyrinth and below Dilated Labyrinth- such as in Ménière's | <ref name="Dizziness">Timothy C Hain. Meniere's Disease. Accessed on 9/2/2020 from https://www.dizziness-and-balance.com/disorders/menieres/menieres.html | ||
</ref><br> Images R Normal Labyrinth and below Dilated Labyrinth- such as in Ménière's | |||
'''Related conditions<ref name="PubMed">PubMed Health. Ménière’s Disease [internet]. Bethesda, MD: A.D.A.M. Inc., National Center for Biotechnology Information, U.S. National Library of Medicine; 2012 [updated 2011 Aug 31; cited 2012 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001721/</ref>''' | '''Related conditions<ref name="PubMed">PubMed Health. Ménière’s Disease [internet]. Bethesda, MD: A.D.A.M. Inc., National Center for Biotechnology Information, U.S. National Library of Medicine; 2012 [updated 2011 Aug 31; cited 2012 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001721/</ref>''' | ||
*Head Injury | *[[Overview of Traumatic Brain Injury|Head Injury]] | ||
*Middle or Inner Ear Infection | *Middle or Inner Ear Infection | ||
*Fibrosis | *Fibrosis | ||
| Line 39: | Line 42: | ||
*Allergies | *Allergies | ||
*Alcohol Use | *[[Alcoholism|Alcohol]] Use | ||
*Genetic abnormalities | *Genetic abnormalities | ||
*Family History | *Family History | ||
| Line 45: | Line 48: | ||
*Recent Viral Illness | *Recent Viral Illness | ||
*Respiratory Infection | *Respiratory Infection | ||
*Smoking | *[[Smoking Cessation and Brief Intervention|Smoking]] | ||
*Stress | *[[Stress and Health|Stress]] | ||
*Use of Certain Medications | *Use of Certain Medications | ||
== Characteristics/Clinical Presentation == | == Characteristics/Clinical Presentation == | ||
One or both ears can be affected. The chief symptoms are: | One or both ears can be affected. The chief symptoms are: | ||
* Vertigo. This is the main symptom of Ménière's disease and is commonly the most debilitating part of an attack. This feeling of dizziness can last anywhere from 20 minutes to a few days, with the average attack being two to four hours. During an attack of vertigo, the room seems to be spinning and the person feels imbalanced. This sensation may produce nystagmus(beating of the eyes from side to side), nausea, vomiting or sweating. An attack of vertigo can persist with a constant intensity or may gradually increase in intensity<ref name="Mayo Symptoms">Meniere’s disease Symptoms – Mayo Clinic [Internet]. Mayo Clinic. 2017 [cited 2 Apr 2017]. Available from http://www.mayoclinic.org/diseases-conditions/menieres-disease/basics/symptoms/con-20028251.</ref>. Recurrent vertigo often affects patients' daily activities even during periods of remission. The episodes often force a person to lie down for several hours and lose time from work or leisure activities. Vertigo can increase risk of falls, accidents while driving a car or operating heavy machinery<ref name="Hain AHRF" />.<ref name=":1" /> | * [[Vertigo]]. This is the main symptom of Ménière's disease and is commonly the most debilitating part of an attack. This feeling of dizziness can last anywhere from 20 minutes to a few days, with the average attack being two to four hours. During an attack of vertigo, the room seems to be spinning and the person feels imbalanced. This sensation may produce nystagmus(beating of the eyes from side to side), nausea, vomiting or sweating. An attack of vertigo can persist with a constant intensity or may gradually increase in intensity<ref name="Mayo Symptoms">Meniere’s disease Symptoms – Mayo Clinic [Internet]. Mayo Clinic. 2017 [cited 2 Apr 2017]. Available from http://www.mayoclinic.org/diseases-conditions/menieres-disease/basics/symptoms/con-20028251.</ref>. Recurrent vertigo often affects patients' daily activities even during periods of remission. The episodes often force a person to lie down for several hours and lose time from work or leisure activities. Vertigo can increase risk of [[Falls Risk Assessment Tool (FRAT): An Overview to Assist Understanding and Conduction|falls]], accidents while driving a car or operating heavy machinery<ref name="Hain AHRF">Hain T. American Hearing Research Foundation. Ménière’s disease [internet]; [updated 2012 Oct; cited 2017 Apr 1]. Available from: http://www.american-hearing.org/disorders/menieres-disease/</ref>.<ref name=":1" /> | ||
* Hearing loss. Usually affects one ear. The person will have a decline in ability to hear during an attack but will regain hearing when current episode has ended. When a person has had Ménière's for a prolonged period, the hearing loss may become permanent. Low frequency tones are most frequently lost, but all tones may be affected as the disease progresses.'''<ref name="Mayo Symptoms" />''' | * Hearing loss. Usually affects one ear. The person will have a decline in ability to hear during an attack but will regain hearing when current episode has ended. When a person has had Ménière's for a prolonged period, the hearing loss may become permanent. Low frequency tones are most frequently lost, but all tones may be affected as the disease progresses.'''<ref name="Mayo Symptoms" />''' | ||
* [[Tinnitus]] | * [[Tinnitus]] i.e. sustained, loud ringing or buzzing in the ears. The intensity of this may vary, but the symptom is continual in people diagnosed with Ménière's'''<ref name="Mayo Symptoms" />'''. | ||
* Sensation of fullness in the ears. Typically the first symptom experienced preceding an acute attack. This feeling is similar to what is felt when changing altitudes (such as in an airplane) but cannot be relieved by swallowing'''<ref name="Mayo Symptoms" />'''. | * Sensation of fullness in the ears. Typically the first symptom experienced preceding an acute attack. This feeling is similar to what is felt when changing altitudes (such as in an airplane) but cannot be relieved by swallowing'''<ref name="Mayo Symptoms" />'''. | ||
* Tullio phenomenon occasionally experienced (the precipitation of vertigo and nystagmus by a loud noise). | * Tullio phenomenon occasionally experienced (the precipitation of vertigo and nystagmus by a loud noise). | ||
* Other Symptoms ; Diarrhoea; | * Other Symptoms ; Diarrhoea; [[Headache]]<nowiki/>s; [[Pain-Modulation|Pain]]/discomfort in the abdomen; Uncontrollable Eye Movements | ||
== Evaluation == | == Evaluation == | ||
The American Academy of Otolaryngology-Head and Neck Surgery Committee on Hearing and Equilibrium set criteria for diagnosing Ménière disease, most recently revised in 1995: | The American Academy of Otolaryngology-Head and Neck Surgery Committee on Hearing and Equilibrium set criteria for diagnosing Ménière disease, most recently revised in 1995: | ||
| Line 75: | Line 66: | ||
* probable: only one definitive episode of vertigo and the other symptoms and signs | * probable: only one definitive episode of vertigo and the other symptoms and signs | ||
* possible: definitive vertigo with no associated hearing loss<ref name=":1" /> | * possible: definitive vertigo with no associated hearing loss<ref name=":1" /> | ||
The role of imaging is controversial, but improved spatial resolution in CT and MRI is likely to show where the endolymphatic flow is impaired<ref name=":1" />. | The role of imaging is controversial, but improved spatial resolution in [[CT Scans|CT]] and [[MRI Scans|MRI]] is likely to show where the endolymphatic flow is impaired<ref name=":1" />. | ||
* Some advocate patients with one-sided hearing loss should undergo magnetic resonance imaging (MRI) to rule out retrocochlear pathology.<ref name=":0" /> | * Some advocate patients with one-sided hearing loss should undergo magnetic resonance imaging (MRI) to rule out retrocochlear pathology.<ref name=":0" /> | ||
Audiometric evaluation is mandatory in all patients with Meniere disease. | Audiometric evaluation is mandatory in all patients with Meniere disease. | ||
* Fluctuating low frequency unilateral sensorineural hearing loss is characteristic for the disease. The hearing loss can progress to all frequencies. Tinnitus is common and ipsilateral. | * Fluctuating low frequency unilateral sensorineural hearing loss is characteristic for the disease. The hearing loss can progress to all frequencies. Tinnitus is common and ipsilateral. | ||
Vestibular (caloric) function testing may show a significantly under-functioning affected organ in 42% to 74% and a full loss of function in 6% to 11%<br>Balance Test | Vestibular (caloric) function testing may show a significantly under-functioning affected organ in 42% to 74% and a full loss of function in 6% to 11%<br>[[Balance Evaluation Systems Test (BESTest)|Balance]] Test | ||
* The visual and vestibular systems interact with each other to maintain visual clarity of objects during head movement. Head movement or other stimulation of the inner ear sends signals to the muscles of the [[Eye muscle exercise|eyes]] via the nervous system, which is called the [[Vestibular Oculomotor Motor Screening (VOMS) Assessment|vestibulo-ocular reflex]] (VOR). The VOR normally generates eye movements that maintain clear vision with head movement. [[Balance]] tests are used to determine which ear is affected, assess the level of balance lost, and assess the brain’s compensation for the damage in the ear.<ref name="vestibular">Vestibular Disorders Association. Ménière’s Disease [internet]. Portland, OR; [updated 2011 Mar 11; cited 2012 Mar 15]. Available from: http://www.vestibular.org/</ref> See [[Vestibular Oculomotor Motor Screening (VOMS) Assessment]] | |||
The visual and vestibular systems interact with each other to maintain visual clarity of objects during head movement. Head movement or other stimulation of the inner ear sends signals to the muscles of the eyes via the nervous system, which is called the [[Vestibular | |||
== Differential Diagnosis == | == Differential Diagnosis == | ||
Other conditions can produce the same symptoms as Ménière’s disease and must be ruled out in order to develop an accurate diagnosis. The differential diagnosis is broad and includes:<ref name="Ear Surgery" /> | Other conditions can produce the same symptoms as Ménière’s disease and must be ruled out in order to develop an accurate diagnosis. The differential diagnosis is broad and includes:<ref name="Ear Surgery">Levenson M. Ménière’s Disease [internet]. Saratoga Springs, NY: The Ear Surgery Information Center; 2017[cited 2017 Apr 1]. Available from http://www.earsurgery.org/?s=meniere%27s+disease</ref> | ||
*Perilymph fistula, | *Perilymph fistula, | ||
*Recurrent labyrinthitis, | *Recurrent labyrinthitis, | ||
* | *[[Migraine Headache|Migraine ]](bilateral hearing fluctuation), | ||
*Congenital ear malformations, | *Congenital ear malformations, | ||
* | *[[Multiple Sclerosis (MS)|Multiple sclerosis,]] | ||
*Posterior fossa arachnoid cysts, | *Posterior fossa arachnoid cysts, | ||
*Stroke in the distribution of the anterior inferior cerebellar artery may cause symptoms similar to Ménière’s (fluctuating hearing, tinnitus, vertigo), | *[[Stroke]] in the distribution of the anterior inferior cerebellar artery may cause symptoms similar to Ménière’s (fluctuating hearing, tinnitus, vertigo), | ||
*Infections of the inner ear, such as syphillis and Lyme disease (episodes of vertigo and hearing loss but usually bilateral) | *Infections of the inner ear, such as syphillis and [[Lyme Disease|Lyme disease]] (episodes of vertigo and hearing loss but usually bilateral) | ||
*Tumors, especially acoustic neuromas, | *Tumors, especially acoustic neuromas, of the inner ear nerve ([[Cranial Nerves|Cranial]] Nerve Eight), compresses the nerve and creates hearing loss, but with no periods of improvement. Imbalance is felt more than vertigo, | ||
*Cholesteatomas (cystic growth) or other infections of middle ear, | *Cholesteatomas (cystic growth) or other infections of middle ear, | ||
*Autoimmune disorder - the system producing antibodies which attack the inner ear. | *[[Autoimmune Disorders|Autoimmune disorder]] - the system producing antibodies which attack the inner ear. <ref name="Dizziness" /> | ||
== Management == | |||
Different treatment options for Meniere disease exist with substantial variability between countries. None of the treatment options cure the disease. | |||
As many treatments have a significant impact on the functioning of surrounding structures, start with non-invasive approaches with the fewest possible side effects and proceed to more invasive steps. | |||
* Sodium restriction diet: Low-level evidence suggests that restricting the sodium intake may help to prevent Meniere attacks. | |||
* Betahistine (used for vertigo and Meniere's disease). It helps to reduce the episodes of vertigo associated with Meniere's disease.: A Cochrane review found low-level evidence to support the use of betahistin with substantial variability between studies. Medical therapy in many medical centers often starts with betahistine orally. | |||
* Intratympanic steroid injections may reduce the number of vertigo attacks in patients with Meniere disease. | |||
* Intratympanic gentamycin injections: Gentamycin has strong ablative properties towards vestibular cells. Side effects are a sensorineural hearing loss because of a certain amount of toxicity towards cochlear cells. | |||
* Surgery with vestibular nerve section or labyrinthectomy: Nerve section is a therapeutic option in patients who failed the conservative treatment options and labyrinthectomy when surgical options failed. Labyrinthectomy leads to a complete hearing loss in the affected side<ref name=":0" /> | |||
Lifestyle Modifications | |||
* Salt restriction helps to reduce excess fluid in ears over time. This helps to limit attacks. | |||
* Caffeine stimulates nerves and can affect Ménière's, so a reduction in caffeine can be helpful. | |||
* Smoking constricts the blood vessels and restricts blood flow to the nerve endings. | |||
* Keeping stress and anxiety levels low can also help to prevent attacks. Fear of an attack could be an added stress that the person will want to learn to control. | |||
Hearing Aid | |||
* Hearing aids can be useful in patients with Ménière's that have progressive hearing loss. Hearing aids can help the person hear to the best of their ability for as long as possible. | |||
== Physical Therapy Management == | == Physical Therapy Management == | ||
Despite the fact that physical therapy cannot address the underlying cause of Ménière’s disease physiotherapy management can assist patients in several ways:<ref name="Hain PT">Hain, T. C., Physical Therapy for Meniere's Disease, 2008 [cited 1 Apr 2017]. Available from: http://www.dizziness-and-balance.com/treatment/rehab/menieresPT.html.</ref><br> | Despite the fact that physical therapy cannot address the underlying cause of Ménière’s disease physiotherapy management can assist patients in several ways:<ref name="Hain PT">Hain, T. C., Physical Therapy for Meniere's Disease, 2008 [cited 1 Apr 2017]. Available from: http://www.dizziness-and-balance.com/treatment/rehab/menieresPT.html.</ref><br> | ||
#Improve and help maintain adequate balance | #Improve and help maintain adequate balance e.g. Vestibular rehabilitation (an [[Therapeutic Exercise|exercise-based program]], designed by a specialty-trained vestibular physical therapist, to improve balance and reduce problems related to dizziness) includes: [[Balance Training|Balance]] and/or leg strength/flexibility exercises; [[Gait]] training; Visual stability and training; Neck mobility and neck and arm [[Strength and Conditioning|strength]] techniques. The goal of treatment plan is to improve any deficits, in turn, will improve ability to function in [[Activities of Daily Living|activities of everyday living]], reduce risk for [[Falls|falling]] and ultimately, improve [[Quality of Life|quality of life]]<ref>Cleveland Clinic [https://my.clevelandclinic.org/health/treatments/15298-vestibular-rehabilitation Vestibular rehab]. Available from:https://my.clevelandclinic.org/health/treatments/15298-vestibular-rehabilitation (last accessed 2.8.2020)</ref>[[Quality of Life|.]] | ||
#Educate patients on how to avoid injury due to imbalance or vertigo, techniques on how to fall to minimize injury | #Educate patients on how to avoid injury due to imbalance or vertigo, techniques on how to fall to minimize injury | ||
#Rehabilitate patients after destructive treatments that result in static unilateral or bilateral vestibular loss. | #Rehabilitate patients after destructive treatments that result in static unilateral or bilateral vestibular loss. | ||
| Line 120: | Line 115: | ||
##Visual dependence for balance | ##Visual dependence for balance | ||
##Neck stiffness caused by a common balance coping strategy | ##Neck stiffness caused by a common balance coping strategy | ||
##Recognize the signs and symptoms of depression and anxiety, and make referrals when appropriate | ##Recognize the signs and symptoms of depression and anxiety, and make referrals when appropriate | ||
'''Home Modification''' is often an overlooked physical therapy management tool for Meniere’s disease and other vestibular diseases. However, it is very important to the patient’s safety, especially since people with Meniere’s disease have a hard time predicting when an episode of vertigo will occur. All physical therapist who work with Meniere’s patients should be able to explain Home Safety. | |||
To help safeguard against dangerous falls, suggest the following household improvements are suggested:<ref name="Home">Babb R, Hafner W. Balancing act - the role of vestibular rehabilitation in treating meniere's disease. PTProductsOnline.com. 2011; 20-23.</ref> | |||
*Add grab bars to the shower or tub, both horizontal and vertical | *Add grab bars to the shower or tub, both horizontal and vertical | ||
*Add a shower or tub seat | *Add a shower or tub seat | ||
*Add anti-slip strips in showers or tubs | *Add anti-slip strips in showers or tubs | ||
*Consider an elevated toilet seat | *Consider an elevated toilet seat | ||
*Add ramps and reduce threshold heights in doorways for anyone ambulating with the assistance of a wheeled device (rolling walkers, wheelchairs, scooters, etc) | *Add ramps and reduce threshold heights in doorways for anyone ambulating with the assistance of a wheeled device (rolling walkers, wheelchairs, scooters, etc.) | ||
*Add handrails or secure hand holds at steps or stairs | *Add handrails or secure hand holds at steps or stairs | ||
*Place risers or blocks under the legs of couches or chairs | *Place risers or blocks under the legs of couches or chairs | ||
*Remove throw rugs throughout the house | *Remove throw rugs throughout the house | ||
*Clear out clutter. Set a goal to clear a pathway 36 inches wide, which leaves enough room to easily handle a walker or wheelchair | *Clear out clutter. Set a goal to clear a pathway 36 inches wide, which leaves enough room to easily handle a walker or [[Wheelchair Assessment|wheelchair]] | ||
*Add light sensor night-lights in hallways and bathrooms | *Add light sensor night-lights in hallways and bathrooms | ||
*Add motion-sensor alarms that alert care providers when loved ones start to get out of bed | *Add motion-sensor alarms that alert care providers when loved ones start to get out of bed | ||
*Carry small loads, as heavy ones throw off your balance | *Carry small loads, as heavy ones throw off your balance | ||
*Keep items you use often in easy-to-reach places | *Keep items you use often in easy-to-reach places | ||
== Case Reports/ Case Studies == | |||
Real Clinical Case Example of a Patient with Meniere's Disease: | |||
An 82 year-old female patient presents with severe dizziness and ringing in the ears. She reports having frequent attacks of dizziness with an insidious onset. The patient stated that the first attack of dizziness she experienced was in November of 1968 when she was 34 years old. It was election day and as she got off the couch to go vote, she became very dizzy. | |||
After the first attack, she had recurring attacks once every four to five years until the mid-2000's when they started to become more frequent. Her doctor gave her a medication that made her sleep, but she didn't have any other medical treatments. In 2012, the attacks became more severe causing her to seek further medical attention. Her primary care provider prescribed her Meclizine to help control the dizziness and nausea. The medication helped to | After the first attack, she had recurring attacks once every four to five years until the mid-2000's when they started to become more frequent. Her doctor gave her a medication that made her sleep, but she didn't have any other medical treatments. In 2012, the attacks became more severe causing her to seek further medical attention. Her primary care provider prescribed her Meclizine to help control the dizziness and nausea. The medication helped to control the attacks for awhile, but soon they became more severe and lasted from 48-72 hours as she developed a tolerance to Meclizine. | ||
In 2015, she went to an Ear, Nose & Throat (ENT) doctor that specialized in hearing disorders. A CT scan and MRI were performed to rule out other pathologies and both came back negative. After a series of hearing, vision and vestibular testing, the ENT diagnosed the patient with Meniere's disease. The doctor gave her a steroid injection into the eardrum which significantly helped to manage the dizziness and tinnitus. The patient now receives yearly steroid injections and was fitted | In 2015, she went to an Ear, Nose & Throat (ENT) doctor that specialized in hearing disorders. A CT scan and MRI were performed to rule out other pathologies and both came back negative. After a series of hearing, vision and vestibular testing, the ENT diagnosed the patient with Meniere's disease. The doctor gave her a steroid injection into the eardrum which significantly helped to manage the dizziness and tinnitus. The patient now receives yearly steroid injections and was fitted with a hearing aid to help with the hearing loss due to the disease. The patient also takes Meclizine every day as a preventative measure. | ||
The patient has been diagnosed for two years now and has learned to self-manage the attacks. She is also better at detecting when an attack is about to happen based on the tinnitus. When the ringing in her ears turns into a rushing water sound or sounds like someone walking through mud, she knows she needs to stop what she is doing and take a break until the symptoms go away. Laying down in a dark room and listening to classical music on headphones helps to prevent a severe attack. The disease has also impacted her activities of daily living as she can no longer drive and she is very sensitive to busy backgrounds with a lot of visual input. All of this impacts her ability to go to the store and be a passenger in a car. | The patient has been diagnosed for two years now and has learned to self-manage the attacks. She is also better at detecting when an attack is about to happen based on the tinnitus. When the ringing in her ears turns into a rushing water sound or sounds like someone walking through mud, she knows she needs to stop what she is doing and take a break until the symptoms go away. Laying down in a dark room and listening to classical music on headphones helps to prevent a severe attack. The disease has also impacted her activities of daily living as she can no longer drive and she is very sensitive to busy backgrounds with a lot of visual input. All of this impacts her ability to go to the store and be a passenger in a car. | ||
| Line 281: | Line 165: | ||
[[Category:Medical]] | [[Category:Medical]] | ||
[[Category:Bellarmine_Student_Project]] | [[Category:Bellarmine_Student_Project]] | ||
[[Category:Balance]] | |||
[[Category:Older People/Geriatrics]] | |||
Latest revision as of 17:03, 17 January 2023
Original Editors -Elaine Lonnemann
Top Contributors - Mercedes Nelson, Mary Glorighian, Deborah Bruckman, Lucinda hampton, Tony Lowe, Kim Jackson, Elaine Lonnemann, Vidya Acharya, Admin, Wendy Walker, 127.0.0.1, Hayley Lawler, Mande Jooste, Aminat Abolade, Laura Ritchie, Scott Buxton, Naomi O'Reilly, Magdalena Hytros, WikiSysop and Uchechukwu Chukwuemeka
Introduction[edit | edit source]

Meniere disease (or idiopathic endolymphatic hydrops) is a disorder of the inner ear characterized by hearing loss, tinnitus, and vertigo. It is named after the French physician Prosper Ménière (1799-1862) who first recognised vertigo as an inner ear disorder.
- In most cases, it is slowly progressive and has a significant impact on the social functioning of the individual affected.
- It is an inner ear disorder and as such can affect balance and hearing[1].
- Primarily a unilateral disorder, however, the opposite ear can be affected in 2-50% of people diagnosed with Meniere's disease.[2]
The 2 minute 45 second video below fives a good summary
Epidemiology[edit | edit source]
The prevalence of Meniere disease varies between 3.5 per 100.000 and 513 per 100.000 and occurs more often in older, white and female patients.
The identification of several comorbidities which occur in an increased fashion in patients with Meniere disease gave rise to new theories about the origins of the disease.
- Migraine: Migraine occurs more often in patients diagnosed with Meniere disease although there might be an overlap between basilar migraine wrongly diagnosed as Meniere disease.
- Autoimmune Diseases: Several autoimmune diseases are associated with Meniere disease namely rheumatoid arthritis, systemic lupus erythematosus and ankylosing spondylitis
Etiology[edit | edit source]
- Studies of the temporal bone revealed endolymphatic accumulation in the cochlea and the vestibular organ in patients with Meniere disease.
- Current research links endolymphatic hydrops to a hearing loss of >40dB. Vertigo may or may not be associated.
- Endolymphatic hydrops is not entirely specific for Meniere disease and can be found in cases of idiopathic sensorineural hearing loss.

The exact etiology of Meniere disease remains unclear. Different theories exist, but genetic and environmental factors play a role. The relation to common comorbidities remains elusive[4].
- Although considered to be idiopathic, there is an association with inner ear effusions and endolymphatic hydrops[1].

[5]
Images R Normal Labyrinth and below Dilated Labyrinth- such as in Ménière's
Related conditions[6]
- Head Injury
- Middle or Inner Ear Infection
- Fibrosis
- Atrophy of the endolymphatic sac
- Obstruction of the endolymphatic duct
Risk Factors[6]
- Allergies
- Alcohol Use
- Genetic abnormalities
- Family History
- Fatigue
- Recent Viral Illness
- Respiratory Infection
- Smoking
- Stress
- Use of Certain Medications
Characteristics/Clinical Presentation[edit | edit source]
One or both ears can be affected. The chief symptoms are:
- Vertigo. This is the main symptom of Ménière's disease and is commonly the most debilitating part of an attack. This feeling of dizziness can last anywhere from 20 minutes to a few days, with the average attack being two to four hours. During an attack of vertigo, the room seems to be spinning and the person feels imbalanced. This sensation may produce nystagmus(beating of the eyes from side to side), nausea, vomiting or sweating. An attack of vertigo can persist with a constant intensity or may gradually increase in intensity[7]. Recurrent vertigo often affects patients' daily activities even during periods of remission. The episodes often force a person to lie down for several hours and lose time from work or leisure activities. Vertigo can increase risk of falls, accidents while driving a car or operating heavy machinery[8].[1]
- Hearing loss. Usually affects one ear. The person will have a decline in ability to hear during an attack but will regain hearing when current episode has ended. When a person has had Ménière's for a prolonged period, the hearing loss may become permanent. Low frequency tones are most frequently lost, but all tones may be affected as the disease progresses.[7]
- Tinnitus i.e. sustained, loud ringing or buzzing in the ears. The intensity of this may vary, but the symptom is continual in people diagnosed with Ménière's[7].
- Sensation of fullness in the ears. Typically the first symptom experienced preceding an acute attack. This feeling is similar to what is felt when changing altitudes (such as in an airplane) but cannot be relieved by swallowing[7].
- Tullio phenomenon occasionally experienced (the precipitation of vertigo and nystagmus by a loud noise).
- Other Symptoms ; Diarrhoea; Headaches; Pain/discomfort in the abdomen; Uncontrollable Eye Movements
Evaluation[edit | edit source]
The American Academy of Otolaryngology-Head and Neck Surgery Committee on Hearing and Equilibrium set criteria for diagnosing Ménière disease, most recently revised in 1995:
- certain: a definite disease with histopathological confirmation
- definite: requires two or more definitive episodes of vertigo with a hearing loss plus tinnitus and/or aural fullness
- probable: only one definitive episode of vertigo and the other symptoms and signs
- possible: definitive vertigo with no associated hearing loss[1]
The role of imaging is controversial, but improved spatial resolution in CT and MRI is likely to show where the endolymphatic flow is impaired[1].
- Some advocate patients with one-sided hearing loss should undergo magnetic resonance imaging (MRI) to rule out retrocochlear pathology.[4]
Audiometric evaluation is mandatory in all patients with Meniere disease.
- Fluctuating low frequency unilateral sensorineural hearing loss is characteristic for the disease. The hearing loss can progress to all frequencies. Tinnitus is common and ipsilateral.
Vestibular (caloric) function testing may show a significantly under-functioning affected organ in 42% to 74% and a full loss of function in 6% to 11%
Balance Test
- The visual and vestibular systems interact with each other to maintain visual clarity of objects during head movement. Head movement or other stimulation of the inner ear sends signals to the muscles of the eyes via the nervous system, which is called the vestibulo-ocular reflex (VOR). The VOR normally generates eye movements that maintain clear vision with head movement. Balance tests are used to determine which ear is affected, assess the level of balance lost, and assess the brain’s compensation for the damage in the ear.[9] See Vestibular Oculomotor Motor Screening (VOMS) Assessment
Differential Diagnosis[edit | edit source]
Other conditions can produce the same symptoms as Ménière’s disease and must be ruled out in order to develop an accurate diagnosis. The differential diagnosis is broad and includes:[10]
- Perilymph fistula,
- Recurrent labyrinthitis,
- Migraine (bilateral hearing fluctuation),
- Congenital ear malformations,
- Multiple sclerosis,
- Posterior fossa arachnoid cysts,
- Stroke in the distribution of the anterior inferior cerebellar artery may cause symptoms similar to Ménière’s (fluctuating hearing, tinnitus, vertigo),
- Infections of the inner ear, such as syphillis and Lyme disease (episodes of vertigo and hearing loss but usually bilateral)
- Tumors, especially acoustic neuromas, of the inner ear nerve (Cranial Nerve Eight), compresses the nerve and creates hearing loss, but with no periods of improvement. Imbalance is felt more than vertigo,
- Cholesteatomas (cystic growth) or other infections of middle ear,
- Autoimmune disorder - the system producing antibodies which attack the inner ear. [5]
Management[edit | edit source]
Different treatment options for Meniere disease exist with substantial variability between countries. None of the treatment options cure the disease.
As many treatments have a significant impact on the functioning of surrounding structures, start with non-invasive approaches with the fewest possible side effects and proceed to more invasive steps.
- Sodium restriction diet: Low-level evidence suggests that restricting the sodium intake may help to prevent Meniere attacks.
- Betahistine (used for vertigo and Meniere's disease). It helps to reduce the episodes of vertigo associated with Meniere's disease.: A Cochrane review found low-level evidence to support the use of betahistin with substantial variability between studies. Medical therapy in many medical centers often starts with betahistine orally.
- Intratympanic steroid injections may reduce the number of vertigo attacks in patients with Meniere disease.
- Intratympanic gentamycin injections: Gentamycin has strong ablative properties towards vestibular cells. Side effects are a sensorineural hearing loss because of a certain amount of toxicity towards cochlear cells.
- Surgery with vestibular nerve section or labyrinthectomy: Nerve section is a therapeutic option in patients who failed the conservative treatment options and labyrinthectomy when surgical options failed. Labyrinthectomy leads to a complete hearing loss in the affected side[4]
Lifestyle Modifications
- Salt restriction helps to reduce excess fluid in ears over time. This helps to limit attacks.
- Caffeine stimulates nerves and can affect Ménière's, so a reduction in caffeine can be helpful.
- Smoking constricts the blood vessels and restricts blood flow to the nerve endings.
- Keeping stress and anxiety levels low can also help to prevent attacks. Fear of an attack could be an added stress that the person will want to learn to control.
Hearing Aid
- Hearing aids can be useful in patients with Ménière's that have progressive hearing loss. Hearing aids can help the person hear to the best of their ability for as long as possible.
Physical Therapy Management[edit | edit source]
Despite the fact that physical therapy cannot address the underlying cause of Ménière’s disease physiotherapy management can assist patients in several ways:[11]
- Improve and help maintain adequate balance e.g. Vestibular rehabilitation (an exercise-based program, designed by a specialty-trained vestibular physical therapist, to improve balance and reduce problems related to dizziness) includes: Balance and/or leg strength/flexibility exercises; Gait training; Visual stability and training; Neck mobility and neck and arm strength techniques. The goal of treatment plan is to improve any deficits, in turn, will improve ability to function in activities of everyday living, reduce risk for falling and ultimately, improve quality of life[12].
- Educate patients on how to avoid injury due to imbalance or vertigo, techniques on how to fall to minimize injury
- Rehabilitate patients after destructive treatments that result in static unilateral or bilateral vestibular loss.
- Treat the “spin-offs” of Meniere’s disease (see the notes by Timothy Hain MD):
- Visual dependence for balance
- Neck stiffness caused by a common balance coping strategy
- Recognize the signs and symptoms of depression and anxiety, and make referrals when appropriate
Home Modification is often an overlooked physical therapy management tool for Meniere’s disease and other vestibular diseases. However, it is very important to the patient’s safety, especially since people with Meniere’s disease have a hard time predicting when an episode of vertigo will occur. All physical therapist who work with Meniere’s patients should be able to explain Home Safety.
To help safeguard against dangerous falls, suggest the following household improvements are suggested:[13]
- Add grab bars to the shower or tub, both horizontal and vertical
- Add a shower or tub seat
- Add anti-slip strips in showers or tubs
- Consider an elevated toilet seat
- Add ramps and reduce threshold heights in doorways for anyone ambulating with the assistance of a wheeled device (rolling walkers, wheelchairs, scooters, etc.)
- Add handrails or secure hand holds at steps or stairs
- Place risers or blocks under the legs of couches or chairs
- Remove throw rugs throughout the house
- Clear out clutter. Set a goal to clear a pathway 36 inches wide, which leaves enough room to easily handle a walker or wheelchair
- Add light sensor night-lights in hallways and bathrooms
- Add motion-sensor alarms that alert care providers when loved ones start to get out of bed
- Carry small loads, as heavy ones throw off your balance
- Keep items you use often in easy-to-reach places
Case Reports/ Case Studies[edit | edit source]
Real Clinical Case Example of a Patient with Meniere's Disease:
An 82 year-old female patient presents with severe dizziness and ringing in the ears. She reports having frequent attacks of dizziness with an insidious onset. The patient stated that the first attack of dizziness she experienced was in November of 1968 when she was 34 years old. It was election day and as she got off the couch to go vote, she became very dizzy.
After the first attack, she had recurring attacks once every four to five years until the mid-2000's when they started to become more frequent. Her doctor gave her a medication that made her sleep, but she didn't have any other medical treatments. In 2012, the attacks became more severe causing her to seek further medical attention. Her primary care provider prescribed her Meclizine to help control the dizziness and nausea. The medication helped to control the attacks for awhile, but soon they became more severe and lasted from 48-72 hours as she developed a tolerance to Meclizine.
In 2015, she went to an Ear, Nose & Throat (ENT) doctor that specialized in hearing disorders. A CT scan and MRI were performed to rule out other pathologies and both came back negative. After a series of hearing, vision and vestibular testing, the ENT diagnosed the patient with Meniere's disease. The doctor gave her a steroid injection into the eardrum which significantly helped to manage the dizziness and tinnitus. The patient now receives yearly steroid injections and was fitted with a hearing aid to help with the hearing loss due to the disease. The patient also takes Meclizine every day as a preventative measure.
The patient has been diagnosed for two years now and has learned to self-manage the attacks. She is also better at detecting when an attack is about to happen based on the tinnitus. When the ringing in her ears turns into a rushing water sound or sounds like someone walking through mud, she knows she needs to stop what she is doing and take a break until the symptoms go away. Laying down in a dark room and listening to classical music on headphones helps to prevent a severe attack. The disease has also impacted her activities of daily living as she can no longer drive and she is very sensitive to busy backgrounds with a lot of visual input. All of this impacts her ability to go to the store and be a passenger in a car.
Resources[edit | edit source]
- Directory of Organizations
- Information on vestibular disorders for patients and health professionals, support group, and book: Ménière’s Disease : What you need to know by P.J. Haybach, Jerry Underwood. Click here
- Information on Ménière’s disease
- American Academy of Otolaryngology — Head and Neck Surgery website to help patients find an ENT
- Coping information and support group for patients
- Support group and forum for patients with Ménière’s disease
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 Radiopedia Meniere Disease Available from:https://radiopaedia.org/articles/meniere-disease (last accessed 2.8.2020)
- ↑ Goodman CC, Fuller KS. Pathology: implications for the physical therapist. St. Louis, MO: Elsevier Saunders; 2015; pp 1055-1069.
- ↑ Fauquier ENT Meniere's Disease - What Happens in the Inner Ear?Available from https://www.youtube.com/watchv=qrk7OyAB_ss
- ↑ 4.0 4.1 4.2 Koenen L, Andaloro C. Meniere Disease.June 2020 Available from:https://www.ncbi.nlm.nih.gov/books/NBK536955/ (lat accessed 2.8.2020)
- ↑ 5.0 5.1 Timothy C Hain. Meniere's Disease. Accessed on 9/2/2020 from https://www.dizziness-and-balance.com/disorders/menieres/menieres.html
- ↑ 6.0 6.1 PubMed Health. Ménière’s Disease [internet]. Bethesda, MD: A.D.A.M. Inc., National Center for Biotechnology Information, U.S. National Library of Medicine; 2012 [updated 2011 Aug 31; cited 2012 Mar 15]. Available from: http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001721/
- ↑ 7.0 7.1 7.2 7.3 Meniere’s disease Symptoms – Mayo Clinic [Internet]. Mayo Clinic. 2017 [cited 2 Apr 2017]. Available from http://www.mayoclinic.org/diseases-conditions/menieres-disease/basics/symptoms/con-20028251.
- ↑ Hain T. American Hearing Research Foundation. Ménière’s disease [internet]; [updated 2012 Oct; cited 2017 Apr 1]. Available from: http://www.american-hearing.org/disorders/menieres-disease/
- ↑ Vestibular Disorders Association. Ménière’s Disease [internet]. Portland, OR; [updated 2011 Mar 11; cited 2012 Mar 15]. Available from: http://www.vestibular.org/
- ↑ Levenson M. Ménière’s Disease [internet]. Saratoga Springs, NY: The Ear Surgery Information Center; 2017[cited 2017 Apr 1]. Available from http://www.earsurgery.org/?s=meniere%27s+disease
- ↑ Hain, T. C., Physical Therapy for Meniere's Disease, 2008 [cited 1 Apr 2017]. Available from: http://www.dizziness-and-balance.com/treatment/rehab/menieresPT.html.
- ↑ Cleveland Clinic Vestibular rehab. Available from:https://my.clevelandclinic.org/health/treatments/15298-vestibular-rehabilitation (last accessed 2.8.2020)
- ↑ Babb R, Hafner W. Balancing act - the role of vestibular rehabilitation in treating meniere's disease. PTProductsOnline.com. 2011; 20-23.
- ↑ Gibson B. YouTube. menieresresearch; 2010 [updated 2010 Apr 27; cited 2012 Apr 4]. Available from: http://www.youtube.com/watch?v=TFksAtUpTfg

