Pulmonary Function Test: Difference between revisions
No edit summary |
No edit summary |
||
| Line 5: | Line 5: | ||
</div> | </div> | ||
== Description == | == Description == | ||
PFTs can be used in a variety of settings, and they are generally ordered to: | |||
* Look for evidence of respiratory disease when patients present with respiratory symptoms (e.g. dyspnea, cough, cyanosis, wheezing, etc.); | |||
* Assess for any progression of lung disease; | |||
* Monitor the efficacy of a given treatment; | |||
* Evaluate patients pre-operatively; and | |||
* Monitor for potentially toxic side effects of certain drugs (e.g. amiodarone) | |||
The components of PFTs include: Lung volumes; Spirometry and flow volume loops; Diffusing capacity<ref name=":0" /> | |||
== Different Pulmonary Function Tests == | == Different Pulmonary Function Tests == | ||
[[File:Spirometry1.jpg|right|frameless|399x399px]] | |||
[[Spirometry]] Records the flow of air in and out of a patient's lungs plotted against the volume of air inhaled and exhaled during various respiratory maneuvers | [[Spirometry]] Records the flow of air in and out of a patient's lungs plotted against the volume of air inhaled and exhaled during various respiratory maneuvers | ||
| Line 45: | Line 23: | ||
** An FEV1/FVC <80% suggests obstructive lung disease, while restrictive lung disease typically has normal or increased FEV1/FVC | ** An FEV1/FVC <80% suggests obstructive lung disease, while restrictive lung disease typically has normal or increased FEV1/FVC | ||
** Other useful data from spirometry include measures of flow, such as peak inspiratory flow (PIF) and peak expiratory flow (PEF) *** | ** Other useful data from spirometry include measures of flow, such as peak inspiratory flow (PIF) and peak expiratory flow (PEF) *** | ||
# '''Techniques for measuring Residual volume (RV) and Functional residual capacity (FRC)''': Nitrogen Washout Technique ( in this test, the patient breathes in pure oxygen, the gas he or she exhales is collected, and the nitrogren concentration in the exhaled gas is measured. The volume of nitrogen-containing gas that was present at the beginning of the test (i.e. the FRC) can be calculated from the initial concentration of nitrogen (atmospheric) and the amount of nitrogen washed out from the lungs); Helium Dilution Technique ( in this test, the patient breathes in a known amount and concentration of helium (an inert gas that has poor solubility in blood and lung tissues), and the spirometer measures the new concentration of helium after an equilibrium between the spirometer and the patient's lungs is reached. The FRC can then be calculated according to the relationship ''C1V1 = C2V2'', where ''C'' = concentration and ''V''= volume); Body Plethysmography ( Body plethysmography is a technique based on Boyle's law (''P1V1 = P2V2'') that can be used to determine a patient's FRC, which can then be used to determine RV and TLC. With this technique, the patient sits in a closed chamber with a fixed volume and inhales through a closed mouthpiece, causing increased pressure in the box as his or her lungs expand) | #'''Techniques for measuring Residual volume (RV) and Functional residual capacity (FRC)''': Nitrogen Washout Technique ( in this test, the patient breathes in pure oxygen, the gas he or she exhales is collected, and the nitrogren concentration in the exhaled gas is measured. The volume of nitrogen-containing gas that was present at the beginning of the test (i.e. the FRC) can be calculated from the initial concentration of nitrogen (atmospheric) and the amount of nitrogen washed out from the lungs); Helium Dilution Technique ( in this test, the patient breathes in a known amount and concentration of helium (an inert gas that has poor solubility in blood and lung tissues), and the spirometer measures the new concentration of helium after an equilibrium between the spirometer and the patient's lungs is reached. The FRC can then be calculated according to the relationship ''C1V1 = C2V2'', where ''C'' = concentration and ''V''= volume); Body Plethysmography ( Body plethysmography is a technique based on Boyle's law (''P1V1 = P2V2'') that can be used to determine a patient's FRC, which can then be used to determine RV and TLC. With this technique, the patient sits in a closed chamber with a fixed volume and inhales through a closed mouthpiece, causing increased pressure in the box as his or her lungs expand) | ||
# '''Diffusing Capacity of Carbon monoxide (DLCo) Oxygen'''. Diffusing capacity is a measure of the ability of the lungs to transfer gas into the blood. Diffusion of gas to blood in the lungs is the most efficient when there is a high surface area for transfer, and when the blood is able to accept the gas being transferred. The diffusing capacity is helpful primarily in distinguishing between types of obstructive lung disease. For example, the diffusing capacity will generally be normal or increased in asthma, while it will be decreased in emphysema<ref name=":0">University of Iowa [https://medicine.uiowa.edu/iowaprotocols/pulmonary-function-testing-pft-made-simple Head and neck protocols] Available from: https://medicine.uiowa.edu/iowaprotocols/pulmonary-function-testing-pft-made-simple (accessed 15.5.21)</ref>. | #'''Diffusing Capacity of Carbon monoxide (DLCo) Oxygen'''. Diffusing capacity is a measure of the ability of the lungs to transfer gas into the blood. Diffusion of gas to blood in the lungs is the most efficient when there is a high surface area for transfer, and when the blood is able to accept the gas being transferred. The diffusing capacity is helpful primarily in distinguishing between types of obstructive lung disease. For example, the diffusing capacity will generally be normal or increased in asthma, while it will be decreased in emphysema<ref name=":0">University of Iowa [https://medicine.uiowa.edu/iowaprotocols/pulmonary-function-testing-pft-made-simple Head and neck protocols] Available from: https://medicine.uiowa.edu/iowaprotocols/pulmonary-function-testing-pft-made-simple (accessed 15.5.21)</ref>. | ||
# '''Peak Expiratory flow Meter Reading to generate a flow volume loop'''. | #'''Peak Expiratory flow Meter Reading to generate a flow volume loop'''. | ||
#[[Arterial Blood Gases|Arterial Blood Gas Analysis]] | #[[Arterial Blood Gases|Arterial Blood Gas Analysis]] | ||
# '''Bronchodilator Test'''. Used to test for eg Asthma. One of the defining characteristics of asthma is an increase in the responsiveness of the airways to a number of stimuli. If lung function is normal but the patient experiences intermittent episodes of cough, dyspnea, or wheezing, the demonstration of bronchial hyper-responsiveness may be useful in establishing a diagnosis of asthma. Two general types of bronchoprovocation studies exist: direct and indirect. Direct testing employs pharmacologic agents that directly stimulate airway smooth muscle receptors to cause bronchoconstriction (most commonly utilized drugs in direct testing are methacholine and histamine). Indirect testing incorporates agents that stimulate release of pro-inflammatory mediators, which ultimately induce bronchoconstriction. Indirect tests employ hypertonic saline or mannitol or are based on exercise protocols used to elicit [[Exercise Induced Asthma|exercise-induced]]<ref>Pulmonary Advisor PFT Available from: https://www.pulmonologyadvisor.com/home/decision-support-in-medicine/pulmonary-medicine/pulmonary-function-testing/ (accessed 15.5.21)</ref> [[Exercise Induced Asthma|asthma]] or eucapnic voluntary hyperpnea. | # [[File:Asthma inhaler use.png|right|frameless|300x300px]]'''Bronchodilator Test'''. Used to test for eg Asthma. One of the defining characteristics of asthma is an increase in the responsiveness of the airways to a number of stimuli. If lung function is normal but the patient experiences intermittent episodes of cough, dyspnea, or wheezing, the demonstration of bronchial hyper-responsiveness may be useful in establishing a diagnosis of asthma. Two general types of bronchoprovocation studies exist: direct and indirect. Direct testing employs pharmacologic agents that directly stimulate airway smooth muscle receptors to cause bronchoconstriction (most commonly utilized drugs in direct testing are methacholine and histamine). Indirect testing incorporates agents that stimulate release of pro-inflammatory mediators, which ultimately induce bronchoconstriction. Indirect tests employ hypertonic saline or mannitol or are based on exercise protocols used to elicit [[Exercise Induced Asthma|exercise-induced]]<ref>Pulmonary Advisor PFT Available from: https://www.pulmonologyadvisor.com/home/decision-support-in-medicine/pulmonary-medicine/pulmonary-function-testing/ (accessed 15.5.21)</ref> [[Exercise Induced Asthma|asthma]] or eucapnic voluntary hyperpnea. | ||
#[[Cardiopulmonary Exercise Testing (CPET) In Adults|Cardiorespiratory Exercise Test]] <ref>Guazzi M, Bandera F, Ozemek C, Systrom D, Arena R.Cardiopulmonary Exercise Testing; What Is its Value?Journal of the American College of Cardiology. 2017;70(13) DOI: 10.1016/j.jacc.2017.08.012 | #[[Cardiopulmonary Exercise Testing (CPET) In Adults|Cardiorespiratory Exercise Test]] <ref>Guazzi M, Bandera F, Ozemek C, Systrom D, Arena R.Cardiopulmonary Exercise Testing; What Is its Value?Journal of the American College of Cardiology. 2017;70(13) DOI: 10.1016/j.jacc.2017.08.012 | ||
</ref> | </ref> | ||
# '''Oximetry''': the measuring of the percentage of oxygen-saturated hemoglobin in the blood by means of an oximeter. Readings below 90 percent may be indicative of impaired lung function or infection. In noninvasive pulse oximetry , a small device placed on a fingertip or earlobe uses light waves to measure the oxygen saturation in arterial blood.<ref>Dictionary.com Oximetry Available from: https://www.dictionary.com/browse/oximetry (accessed 15.5.21)</ref> | #'''Oximetry''': the measuring of the percentage of oxygen-saturated hemoglobin in the blood by means of an oximeter. Readings below 90 percent may be indicative of impaired lung function or infection. In noninvasive pulse oximetry , a small device placed on a fingertip or earlobe uses light waves to measure the oxygen saturation in arterial blood.<ref>Dictionary.com Oximetry Available from: https://www.dictionary.com/browse/oximetry (accessed 15.5.21)</ref> | ||
# '''Respiratory Muscle Function Test'''. Maximal inspiratory and expiratory pressures (MIP/MEPs) are measured by having the patient perform maximal inspiratory and expiratory efforts against a closed valve and measuring the static pressures that are generated. The maximal voluntary ventilation is often coupled with spirometry by having the patient breathe in as deeply and as quickly as possible for ten to fifteen seconds and then extrapolating that volume to one minute<ref name=":0" />. | #'''Respiratory Muscle Function Test'''. Maximal inspiratory and expiratory pressures (MIP/MEPs) are measured by having the patient perform maximal inspiratory and expiratory efforts against a closed valve and measuring the static pressures that are generated. The maximal voluntary ventilation is often coupled with spirometry by having the patient breathe in as deeply and as quickly as possible for ten to fifteen seconds and then extrapolating that volume to one minute<ref name=":0" />. | ||
==== Patterns of Respiratory Diseases ==== | ==== Patterns of Respiratory Diseases ==== | ||
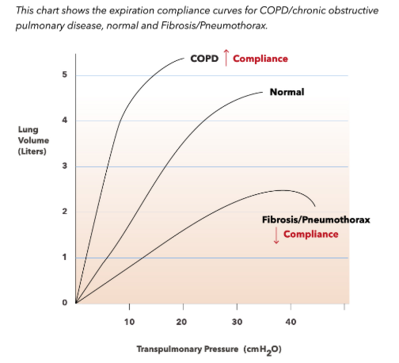
* Obstructive pattern | * [[File:Lung Compliance Transpulmonary Pressure.png|right|frameless|399x399px]]Obstructive pattern | ||
** Decreased FEV1, normal or decreased FVC, and decreased FEV1/FVC | ** Decreased FEV1, normal or decreased FVC, and decreased FEV1/FVC | ||
** Classically, these are the patients with asthma, chronic bronchitis, or emphysema | ** Classically, these are the patients with asthma, chronic bronchitis, or emphysema | ||
| Line 72: | Line 50: | ||
** The flow volume loop is generally normal in appearance, but has low lung volumes | ** The flow volume loop is generally normal in appearance, but has low lung volumes | ||
== | == Indication == | ||
* | * Investigation of a patient with sign/symptoms that shows respiratory problems. e.g. wheezing, coughing, [[Lung Sounds|crackles]] and abnormal [[Chest X-Rays|chest xray]] e.t.c. | ||
* Monitoring of patients with respiratory condition for disease progression and response to treatment. | |||
* Evaluation of degree of cardio-respiratory disability | |||
* Preoperative evaluation for patient that will undergo thoracic and abdominal surgery | |||
* Montoring of patients at risk of pulmonary complications | |||
* Routine assessment for individual with high exposure to pulmonary toxic agent e.g abestos, dust and fumes | |||
== Contraindication == | |||
* [[Myocardial Infarction]] in the last month | |||
* Unstable Angina | |||
* Recent thoracic and abdominal surgeries | |||
* Recent Opthalmic surgery | |||
* Abdominal, thoracic and cerebral Aureysms | |||
* Active Hemoptysis | |||
* [[Pneumothorax]] | |||
FEV1 | == Interpretation == | ||
'''Step 1: FEV1/FVC ratio''' | |||
FEV1 | * FEV1/FVC <70% (or less than the Lower limit of normal) : Obstructive Pattern (COPD, Asthma) | ||
* ≥70%: Normal or Restrictive disease | |||
'''Step 2:''' | |||
'''Severity of obstruction (GOLD Criteria for COPD)''' | |||
FEV1 <50% with right side heart failure: Very severe (Stage 4) | * FEV1 80-100% predicted: Mild (Stage 1) | ||
* FEV1 50- 80% predicted: Moderate (Stage 2) | |||
* FEV1 30- <50% predicted: Severe (Stage 3) | |||
* FEV1 <30% predicted: Very severe (Stage 4) | |||
* FEV1 <50% with right side heart failure: Very severe (Stage 4) | |||
'''Severity of obstruction (ATS General Criteria)''' | '''Severity of obstruction (ATS General Criteria)''' | ||
FEV1 over 70% predicted: MILD | * FEV1 over 70% predicted: MILD | ||
* FEV1 60-70%predicted: MODERATE | |||
FEV1 60-70%predicted: MODERATE | * FEV1 50-60% predicted: MODERATELY SEVERE | ||
* FEV1 35-50% predicted: SEVERE | |||
FEV1 50-60% predicted: MODERATELY SEVERE | * FEV1 <35% predicted: VERY SEVERE | ||
FEV1 35-50% predicted: SEVERE | |||
FEV1 <35% predicted: VERY SEVERE | |||
'''Step 3''' | |||
* ≥12% increase AND an absolute improvement of at least 200ml after inhaling a beta agonist. | |||
* | * FEV1, OR FVC is considered a significant response. | ||
* | |||
'''Step 4: Total Lung Capacity (TLC) (Normal range: 80-120% of predicted)''' | |||
* TLC >120 = Hyperinflation | |||
* '''TLC <80% = Restrictive disease (ATS criteria for severity)''' | |||
* 70-80% predicted: MILD | |||
* 60-70% predicted: MODERATE | |||
* 50-60% predicted: MODERATELY SEVERE | |||
* <50% predicted: SEVERE | |||
Normal or | '''Step 5: RV/TLC ratio (Normal range: <35% or < predicted)''' | ||
* RV/TLC >35% or > predicted indicates Air trapping | |||
'''Step 6: DLCO (Normal range: 80-120% of predicted)''' | |||
Normal in non-parenchymal (e.g. chest wall) restriction<ref>Dweik AR. Interpretation of Common Lung Function Tests.Cleveland Clinic. 2011.https://www.clevelandclinicmeded.com/live/owork/us-state/MDpres2/16.0830.Dweik.Pulm.A.PFTs.CME.v2.pdf</ref> | * '''In obstructive disease:''' | ||
* Decreased in Emphysema | |||
* Normal in chronic bronchitis | |||
* Normal or increased in Asthma | |||
* '''In restrictive disease:''' | |||
* Decreased in parenchymal disease | |||
* Normal in non-parenchymal (e.g. chest wall) restriction<ref>Dweik AR. Interpretation of Common Lung Function Tests.Cleveland Clinic. 2011.https://www.clevelandclinicmeded.com/live/owork/us-state/MDpres2/16.0830.Dweik.Pulm.A.PFTs.CME.v2.pdf</ref> | |||
== References == | == References == | ||
Revision as of 03:42, 15 May 2021
Original Editor - Uchechukwu Chukwuemeka
Top Contributors - Lucinda hampton, Kim Jackson and Admin
Description[edit | edit source]
PFTs can be used in a variety of settings, and they are generally ordered to:
- Look for evidence of respiratory disease when patients present with respiratory symptoms (e.g. dyspnea, cough, cyanosis, wheezing, etc.);
- Assess for any progression of lung disease;
- Monitor the efficacy of a given treatment;
- Evaluate patients pre-operatively; and
- Monitor for potentially toxic side effects of certain drugs (e.g. amiodarone)
The components of PFTs include: Lung volumes; Spirometry and flow volume loops; Diffusing capacity[1]
Different Pulmonary Function Tests[edit | edit source]

Spirometry Records the flow of air in and out of a patient's lungs plotted against the volume of air inhaled and exhaled during various respiratory maneuvers
The values obtained from a given patient are compared with normal values established from reference patients that are matched in size, age, gender, and ethnicity.
- Data obtained from spirometry
- The most commonly used measures include the forced vital capacity (FVC), the forced expiratory volume in one second (FEV1), and the ratio of the two (FEV1/FVC), which should be about 80% in normal patients
- An FEV1/FVC <80% suggests obstructive lung disease, while restrictive lung disease typically has normal or increased FEV1/FVC
- Other useful data from spirometry include measures of flow, such as peak inspiratory flow (PIF) and peak expiratory flow (PEF) ***
- Techniques for measuring Residual volume (RV) and Functional residual capacity (FRC): Nitrogen Washout Technique ( in this test, the patient breathes in pure oxygen, the gas he or she exhales is collected, and the nitrogren concentration in the exhaled gas is measured. The volume of nitrogen-containing gas that was present at the beginning of the test (i.e. the FRC) can be calculated from the initial concentration of nitrogen (atmospheric) and the amount of nitrogen washed out from the lungs); Helium Dilution Technique ( in this test, the patient breathes in a known amount and concentration of helium (an inert gas that has poor solubility in blood and lung tissues), and the spirometer measures the new concentration of helium after an equilibrium between the spirometer and the patient's lungs is reached. The FRC can then be calculated according to the relationship C1V1 = C2V2, where C = concentration and V= volume); Body Plethysmography ( Body plethysmography is a technique based on Boyle's law (P1V1 = P2V2) that can be used to determine a patient's FRC, which can then be used to determine RV and TLC. With this technique, the patient sits in a closed chamber with a fixed volume and inhales through a closed mouthpiece, causing increased pressure in the box as his or her lungs expand)
- Diffusing Capacity of Carbon monoxide (DLCo) Oxygen. Diffusing capacity is a measure of the ability of the lungs to transfer gas into the blood. Diffusion of gas to blood in the lungs is the most efficient when there is a high surface area for transfer, and when the blood is able to accept the gas being transferred. The diffusing capacity is helpful primarily in distinguishing between types of obstructive lung disease. For example, the diffusing capacity will generally be normal or increased in asthma, while it will be decreased in emphysema[1].
- Peak Expiratory flow Meter Reading to generate a flow volume loop.
- Arterial Blood Gas Analysis
- Bronchodilator Test. Used to test for eg Asthma. One of the defining characteristics of asthma is an increase in the responsiveness of the airways to a number of stimuli. If lung function is normal but the patient experiences intermittent episodes of cough, dyspnea, or wheezing, the demonstration of bronchial hyper-responsiveness may be useful in establishing a diagnosis of asthma. Two general types of bronchoprovocation studies exist: direct and indirect. Direct testing employs pharmacologic agents that directly stimulate airway smooth muscle receptors to cause bronchoconstriction (most commonly utilized drugs in direct testing are methacholine and histamine). Indirect testing incorporates agents that stimulate release of pro-inflammatory mediators, which ultimately induce bronchoconstriction. Indirect tests employ hypertonic saline or mannitol or are based on exercise protocols used to elicit exercise-induced[2] asthma or eucapnic voluntary hyperpnea.

- Cardiorespiratory Exercise Test [3]
- Oximetry: the measuring of the percentage of oxygen-saturated hemoglobin in the blood by means of an oximeter. Readings below 90 percent may be indicative of impaired lung function or infection. In noninvasive pulse oximetry , a small device placed on a fingertip or earlobe uses light waves to measure the oxygen saturation in arterial blood.[4]
- Respiratory Muscle Function Test. Maximal inspiratory and expiratory pressures (MIP/MEPs) are measured by having the patient perform maximal inspiratory and expiratory efforts against a closed valve and measuring the static pressures that are generated. The maximal voluntary ventilation is often coupled with spirometry by having the patient breathe in as deeply and as quickly as possible for ten to fifteen seconds and then extrapolating that volume to one minute[1].

Patterns of Respiratory Diseases[edit | edit source]
- Obstructive pattern
- Decreased FEV1, normal or decreased FVC, and decreased FEV1/FVC
- Classically, these are the patients with asthma, chronic bronchitis, or emphysema
- PFTs can help further distinguish between the above three:
- Bronchodilator responsiveness - an increase in the FEV1 by 12% following bronchodilator use suggests asthma
- Bronchial provocation - inducing asthmatic obstruction of reactive lower airways by administering methacholine, histamine, or adenosine monophosphate
- DLCO will be decreased in patients with emphysema, and can be normal or increased in patients with asthma
- PFTs can help further distinguish between the above three:
- Lower airway obstruction vs. upper airway obstruction
- Lower airway obstruction typically displays impaired expiratory capacity (see image below), while upper airway obstruction has impaired inspiratory capacity, which can be evident on the flow volume loop (seen as flattening of the inspiratory arm)

- Restrictive pattern
- Decreased TLC, FEV1, and FVC with a normal FEV1/FVC, and a low DLCO
- Typically these are patients with interstitial lung disease, severe skeletal abnormalities, or diaphragmatic paralysis
- The flow volume loop is generally normal in appearance, but has low lung volumes
Indication[edit | edit source]
- Investigation of a patient with sign/symptoms that shows respiratory problems. e.g. wheezing, coughing, crackles and abnormal chest xray e.t.c.
- Monitoring of patients with respiratory condition for disease progression and response to treatment.
- Evaluation of degree of cardio-respiratory disability
- Preoperative evaluation for patient that will undergo thoracic and abdominal surgery
- Montoring of patients at risk of pulmonary complications
- Routine assessment for individual with high exposure to pulmonary toxic agent e.g abestos, dust and fumes
Contraindication[edit | edit source]
- Myocardial Infarction in the last month
- Unstable Angina
- Recent thoracic and abdominal surgeries
- Recent Opthalmic surgery
- Abdominal, thoracic and cerebral Aureysms
- Active Hemoptysis
- Pneumothorax
Interpretation[edit | edit source]
Step 1: FEV1/FVC ratio
- FEV1/FVC <70% (or less than the Lower limit of normal) : Obstructive Pattern (COPD, Asthma)
- ≥70%: Normal or Restrictive disease
Step 2: Severity of obstruction (GOLD Criteria for COPD)
- FEV1 80-100% predicted: Mild (Stage 1)
- FEV1 50- 80% predicted: Moderate (Stage 2)
- FEV1 30- <50% predicted: Severe (Stage 3)
- FEV1 <30% predicted: Very severe (Stage 4)
- FEV1 <50% with right side heart failure: Very severe (Stage 4)
Severity of obstruction (ATS General Criteria)
- FEV1 over 70% predicted: MILD
- FEV1 60-70%predicted: MODERATE
- FEV1 50-60% predicted: MODERATELY SEVERE
- FEV1 35-50% predicted: SEVERE
- FEV1 <35% predicted: VERY SEVERE
Step 3
- ≥12% increase AND an absolute improvement of at least 200ml after inhaling a beta agonist.
- FEV1, OR FVC is considered a significant response.
Step 4: Total Lung Capacity (TLC) (Normal range: 80-120% of predicted)
- TLC >120 = Hyperinflation
- TLC <80% = Restrictive disease (ATS criteria for severity)
- 70-80% predicted: MILD
- 60-70% predicted: MODERATE
- 50-60% predicted: MODERATELY SEVERE
- <50% predicted: SEVERE
Step 5: RV/TLC ratio (Normal range: <35% or < predicted)
- RV/TLC >35% or > predicted indicates Air trapping
Step 6: DLCO (Normal range: 80-120% of predicted)
- In obstructive disease:
- Decreased in Emphysema
- Normal in chronic bronchitis
- Normal or increased in Asthma
- In restrictive disease:
- Decreased in parenchymal disease
- Normal in non-parenchymal (e.g. chest wall) restriction[5]
References[edit | edit source]
- ↑ 1.0 1.1 1.2 University of Iowa Head and neck protocols Available from: https://medicine.uiowa.edu/iowaprotocols/pulmonary-function-testing-pft-made-simple (accessed 15.5.21)
- ↑ Pulmonary Advisor PFT Available from: https://www.pulmonologyadvisor.com/home/decision-support-in-medicine/pulmonary-medicine/pulmonary-function-testing/ (accessed 15.5.21)
- ↑ Guazzi M, Bandera F, Ozemek C, Systrom D, Arena R.Cardiopulmonary Exercise Testing; What Is its Value?Journal of the American College of Cardiology. 2017;70(13) DOI: 10.1016/j.jacc.2017.08.012
- ↑ Dictionary.com Oximetry Available from: https://www.dictionary.com/browse/oximetry (accessed 15.5.21)
- ↑ Dweik AR. Interpretation of Common Lung Function Tests.Cleveland Clinic. 2011.https://www.clevelandclinicmeded.com/live/owork/us-state/MDpres2/16.0830.Dweik.Pulm.A.PFTs.CME.v2.pdf

