Thoracic Examination: Difference between revisions
(deleted defunct presentation) |
No edit summary |
||
| (5 intermediate revisions by 3 users not shown) | |||
| Line 6: | Line 6: | ||
== Introduction == | == Introduction == | ||
[[File:Thoracic grade 2 T6 PA mobilisations.png|right|frameless]] | [[File:Thoracic grade 2 T6 PA mobilisations.png|right|frameless]] | ||
The | The [[Thoracic Anatomy|Thoracic Spine]] has a complex and often overlooked role within the body. It is a key area of load transfer between the upper and lower body and for rotational movement within the body. | ||
* Should be assessed and treated as a functional unit including not only the spine but the rib cage. | * Should be assessed and treated as a functional unit including not only the spine but the [[Ribs|rib]] cage. | ||
* The thoracic region provides a site for muscle and connective tissue attachments from the head, neck, shoulder blade, clavicle, lumbar spine and pelvis as well as connections to organs in the rib cage and abdomen. | * The thoracic region provides a site for [[Thoracic Spine Major Muscles|muscle]] and connective tissue attachments from the head, neck, shoulder blade, clavicle, lumbar spine and pelvis as well as connections to organs in the rib cage and abdomen. | ||
* It has a role in breathing, is protection for vital organs, and has a relationship to emotions and the nerves that control the ‘fight or flight’ response. | * It has a role in breathing, is protection for vital organs, and has a relationship to emotions and the nerves that control the ‘fight or flight’ response. | ||
Watch this 5 minute showing of a thoracic examination by a physiotherapist | Watch this 5-minute showing of a thoracic examination by a physiotherapist | ||
{{#ev:youtube|https://www.youtube.com/watch?v=FJtjB6lnObU&app=desktop|width}}<ref>PTN Thoracic examination Available from:https://www.youtube.com/watch?v=FJtjB6lnObU&app=desktop (last accessed 15.4.2020)</ref> | {{#ev:youtube|https://www.youtube.com/watch?v=FJtjB6lnObU&app=desktop|width}}<ref>PTN Thoracic examination Available from:https://www.youtube.com/watch?v=FJtjB6lnObU&app=desktop (last accessed 15.4.2020)</ref> | ||
== | == Initial Diagnosis == | ||
When observing and assessing client be aware of the common causes of thoracic spine pain, so you can screen for them, beginning the elimination process towards diagnosis. | When observing and assessing client be aware of the common causes of thoracic spine pain, so you can screen for them, beginning the elimination process towards diagnosis. | ||
* Sprain or strain; Spinal joint sprain involving the disc or zygapophyseal (facet) joint; rib joint sprain; muscle strain. | * [[Ligament Sprain|Sprain]] or strain; Spinal joint sprain involving the disc or zygapophyseal (facet) joint; rib joint sprain; [[Muscle Strain|muscle strain]]. | ||
* Reduced thoracic mobility may be due to; rib cage, spinous processes, zygapophyseal joint capsules, ligamentum flavum, dimensions of the vertebral bodies. | * Reduced thoracic mobility may be due to; rib cage, spinous processes, [[Facet Joints|zygapophyseal]] joint capsules, [[ligamentum flavum]], dimensions of the vertebral bodies. | ||
* [[Scheuermanns Disease|Scheuermanns]] syndrome in adolescents | * [[Scheuermanns Disease|Scheuermanns]] syndrome in adolescents | ||
* [[Posture|Postural]] and overuse syndromes in students and office based workers | * [[Posture|Postural]] and overuse syndromes in students and office-based workers | ||
* Less common causes - [[Ribs|Rib]] or [[Osteoporotic Vertebral Fractures|compression fractures]], [[Thoracic Outlet Syndrome (TOS)|thoracic outlet syndrome]] and [[T4 Syndrome|T4 syndrome]]. | * Less common causes - [[Ribs|Rib]] or [[Osteoporotic Vertebral Fractures|compression fractures]], [[Thoracic Outlet Syndrome (TOS)|thoracic outlet syndrome]] and [[T4 Syndrome|T4 syndrome]]. | ||
* [[ | * [[Thoracic Back Pain Red Flags|Red flags]] eg cardiac or lung conditions ([[pneumothorax]], [[Pulmonary Embolism|pulmonary embolism]]), peptic ulcers, tumours and mesothelioma after exposure to asbestos.<ref>Lifecare North sports Clinic [https://www.lifecare.com.au/clinic/northern-sports-physiotherapy-clinic/news/thoracic-spine/ Thoracic spine] Available from: https://www.lifecare.com.au/clinic/northern-sports-physiotherapy-clinic/news/thoracic-spine/ (last accessed 15.4.2020)</ref> | ||
== Functional Anatomy == | == Functional Anatomy == | ||
[[File:Thoracic spondylolysis.png|461x461px|<ref>[[Thoracic Vertebrae]]</ref>|right|frameless]]The function of the [[Thoracic Anatomy|thoracic spine and ribcage]] is the: | [[File:Thoracic spondylolysis.png|461x461px|<ref>[[Thoracic Vertebrae]]</ref>|right|frameless]]The function of the [[Thoracic Anatomy|thoracic spine and ribcage]] is the: | ||
* protection of the heart, lungs and viscera, ventilation of the lungs | * protection of the heart, [[Lung Anatomy|lungs]] and viscera, ventilation of the lungs | ||
* provide a stable base for the attachment of muscles of the upper limbs, head and neck, vertebral column and the pelvis.<ref name=":1">Oliver, J., Middleditch, A., (1991), Functional Anatomy of the Spine, Butterworth-Heinemann, Oxford</ref> <ref name=":2">Levangie P, Norkin C, (2001), Joint Structure and Function; A Comprehensive Analysis, 3 rd Edition, F.A. Davis Company, Philadelphia</ref>(at the expense of mobility). | * provide a stable base for the attachment of muscles of the upper limbs, head and neck, vertebral column and the [[pelvis]].<ref name=":1">Oliver, J., Middleditch, A., (1991), Functional Anatomy of the Spine, Butterworth-Heinemann, Oxford</ref> <ref name=":2">Levangie P, Norkin C, (2001), Joint Structure and Function; A Comprehensive Analysis, 3 rd Edition, F.A. Davis Company, Philadelphia</ref>(at the expense of mobility). | ||
# The thoracic spine: | # The thoracic spine: | ||
* lies between the superior cervical spine and the inferior [[Lumbar|lumbar spine]]. It | * lies between the superior cervical spine and the inferior [[Lumbar|lumbar spine]]. It | ||
* consists of [[Thoracic Vertebrae|12 vertebrae]], the bodies of the thoracic vertebrae are medium sized and heart shaped,<ref name=":0">Thoracic Vertebrae. (2018, January 15). ''Physiopedia,'' . Retrieved 13:45, January 28, 2018 from https://www.physio-pedia.com/index.php?title=Thoracic_Vertebrae&oldid=182308.</ref> generally increase in size from superiorly to inferiorly to support increase the increases in weight that needs to be supported. | * consists of [[Thoracic Vertebrae|12 vertebrae]], the bodies of the thoracic vertebrae are medium-sized and heart-shaped,<ref name=":0">Thoracic Vertebrae. (2018, January 15). ''Physiopedia,'' . Retrieved 13:45, January 28, 2018 from https://www.physio-pedia.com/index.php?title=Thoracic_Vertebrae&oldid=182308.</ref> generally increase in size from superiorly to inferiorly to support increase the increases in weight that needs to be supported. | ||
* possess articular facets on their sides for articulation with the heads of the ribs.<ref name=":0" /><ref name=":2" /> | * possess articular facets on their sides for articulation with the heads of the ribs.<ref name=":0" /><ref name=":2" /> | ||
2. The rib cage consists of 12 pairs of [[ribs]]: | 2. The rib cage consists of 12 pairs of [[ribs]]: | ||
* [[First Rib|1 st]] – | * [[First Rib|1 st]] – 7th ribs: (true) attach directly to the sternum | ||
* | * 8th – 10th ribs: articulate with sternum via the costal [[cartilage]]<nowiki/>s above them | ||
* | * 11th and 12th ribs: floating ribs as they do not attach to sternum<ref name=":1" /> | ||
== Subjective Assessment == | == Subjective Assessment == | ||
Area | === Symptoms (Recorded on a Body Chart) === | ||
==== Area ==== | |||
* Distribution | * Distribution | ||
** May follow course of rib or run horizontally across chest. | ** May follow course of rib or run horizontally across the chest. | ||
** Thoracic spine, [[scapula]] or sternum | ** Thoracic spine, [[scapula]] or sternum | ||
** Upper limbs (upper cervical spine) | ** Upper limbs (upper cervical spine) | ||
** Lower limbs (lower cervical spine) | ** Lower limbs (lower cervical spine) | ||
** Clear all other relevant areas and mark with ticks<ref name=":3">Magee, D, (2002) Orthopedic Physical Assessment, 4 th Edition, Saunders, London</ref> | ** Clear all other relevant areas and mark with ticks<ref name=":3">Magee, D, (2002) Orthopedic Physical Assessment, 4 th Edition, Saunders, London</ref> | ||
Type | |||
==== Type ==== | |||
* Quality | * Quality | ||
| Line 54: | Line 56: | ||
* Depth | * Depth | ||
* Abnormal | * Abnormal sensation | ||
** Paraesthesia | ** Paraesthesia | ||
** Numbness | ** Numbness | ||
| Line 71: | Line 73: | ||
* Severity and irritability | * Severity and irritability | ||
** Used to identify those who will not be able to tolerate a full objective examination | ** Used to identify those who will not be able to tolerate a full objective examination | ||
** Severity - If patient is able to sustain a position that reproduces the symptoms then condition is considered non-severe. If patient cannot sustain the position, the condition is considered severe and no overpressures should be attempted | ** Severity - If a patient is able to sustain a position that reproduces the symptoms then the condition is considered non-severe. If the patient cannot sustain the position, the condition is considered severe and no overpressures should be attempted | ||
* Irritability- If symptoms ease immediately after provocation then the condition is considered to be non-irritable and all movements can be tested. If symptoms take a few minutes to ease, the symptoms are irritable and only a few movements should be attempted to avoid exacerbating the patients’ symptoms | * Irritability- If symptoms ease immediately after provocation then the condition is considered to be non-irritable and all movements can be tested. If symptoms take a few minutes to ease, the symptoms are irritable and only a few movements should be attempted to avoid exacerbating the patients’ symptoms | ||
| Line 78: | Line 80: | ||
* Improving, staying the same, getting worse<ref name=":3" /> | * Improving, staying the same, getting worse<ref name=":3" /> | ||
Special questions are used to identify precautions or absolute contraindications to examination or treatment | === Special Questions === | ||
[[File:National-cancer-institute-0YBIMOqQzt0-unsplash.jpg|right|frameless|200x200px]] | |||
Special questions are used to identify precautions or absolute contraindications to examination or treatment | |||
* General health | * General health | ||
* Weight loss | * Weight loss | ||
| Line 87: | Line 90: | ||
* X-rays and medical imaging | * X-rays and medical imaging | ||
* Neurological symptoms | * Neurological symptoms | ||
=== History of Present Condition (HPC) === | |||
* Known or unknown cause | * Known or unknown cause | ||
* Sudden/slow onset | * Sudden/slow onset | ||
* How long ago did symptoms start | * How long ago did symptoms start | ||
* Route to physiotherapy | * Route to physiotherapy | ||
=== Past Medical History (PMH) === | |||
* Relevant medical history | * Relevant medical history | ||
* Previous episodes | * Previous episodes | ||
* Previous Rx | * Previous Rx | ||
=== Social History === | |||
* Employment, dependants, leisure activities etc. | * Employment, dependants, leisure activities etc. | ||
The thoracic area is a common place for the cervical spine to refer symptoms, so screen the cervical spine including assessing for previous neck pain or neck trauma is necessary to rule | === Region-Specific Historical Examination === | ||
The thoracic area is a common place for the cervical spine to refer symptoms, so screen the cervical spine including assessing for previous neck pain or neck trauma is necessary to rule out cervical spine involvement.<ref>Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. [https://journals.lww.com/spinejournal/fulltext/2003/01010/reliability_and_diagnostic_accuracy_of_the.14.aspx Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy.] Spine. 2003 Jan 1;28(1):52-62.</ref><ref name=":2" /> eg “Do neck movements improve your symptoms?” “Where is the pain most bothersome?” | |||
<br> | <br> | ||
=== Special Questions | === Special Questions === | ||
[[File:Red flag photo.jpg|right|frameless|300x300px]] | |||
| | |||
| | |||
| | |||
| | ==== Red [[The Flag System|Flags]] ==== | ||
*[[Thoracic Anatomy|Thoracic spine]] pain and visceral pain can mimic the other due to the shared afferent innervation of the ANS sympathetics, which originate from T1-L2 afferents from the spinal cord.<ref>Benhamou CL, Roux C, Tourliere D, Gervais T, Viala JF, Amor B. [https://journals.lww.com/spinejournal/Citation/1993/05000/Pseudovisceral_Pain_Referred_From_Costovertebral.24.aspx Pseudovisceral pain referred from costovertebral arthropathies: twenty-eight cases.] Spine. 1993 May 1;18(6):790-5.</ref> | |||
*Segments T4-T7 have the potential to cause pseudoanginal pain as well as symptoms generated by a cough, sneeze, deep breath, movement of the trunk, palpation, and compression.<ref>Hamberg J, Lindahl O. [https://onlinelibrary.wiley.com/doi/abs/10.1111/j.0954-6820.1981.tb03130.x Angina pectoris symptoms caused by thoracic spine disorders.] Clinical examination and treatment. Acta Medica Scandinavica. 1981 Jan 12;209(S644):84-6.</ref> | |||
*See also [[Thoracic Back Pain Red Flags]] | |||
==== Yellow Flags ==== | |||
*[http://www.physio-pedia.com/index.php5?title=Fear%E2%80%90Avoidance_Belief_Questionnaire Fear-Avoidance Beliefs Questionnaire] (FABQ) can be used to screen for behaviours that may require a consult or an increase in treatment duration. | |||
*Patients involved in on-going litigation have been found to have reduced changes in quality of life and higher rates of disability with the physical gains made in therapy.<ref>Blake C, Garrett M. [https://link.springer.com/article/10.1007/BF02943586 Impact of litigation on quality of life outcomes in patients with chronic low back pain.] Irish journal of medical science. 1997 Jul 1;166(3):124-6.</ref> | |||
*[http://www.physio-pedia.com/index.php5?title=Fear%E2%80%90Avoidance_Belief_Questionnaire Fear-Avoidance Beliefs Questionnaire] (FABQ) can be used to screen for | |||
*Patients involved in on-going litigation have been found to have reduced changes in quality of life and higher rates of disability with the physical gains made in therapy.<ref>Blake C, Garrett M. Impact of litigation on quality of life outcomes in patients with chronic low back pain. | |||
=== Investigations === | === Investigations === | ||
| Line 152: | Line 127: | ||
*Radiographs are sensitive to assess for acute compression fractures; however, if the patient’s initial radiographs were read as normal and they are still experiencing extreme pain or symptoms consider a referral for advanced imaging such as CT or MRI. | *Radiographs are sensitive to assess for acute compression fractures; however, if the patient’s initial radiographs were read as normal and they are still experiencing extreme pain or symptoms consider a referral for advanced imaging such as CT or MRI. | ||
*Patients with red flags for cancer should be referred for imaging to rule out cancer. | *Patients with red flags for cancer should be referred for imaging to rule out cancer. | ||
*Patients with suspected Ankylosing Spondylitis are typically referred for radiographs of the sacroiliac joints and lab studies including assessing for the presence of HLA-B27. | *Patients with suspected Ankylosing Spondylitis are typically referred for radiographs of the sacroiliac joints and lab studies including assessing for the presence of HLA-B27. | ||
== Objective Examination == | == Objective Examination == | ||
=== Observation === | |||
*The examiners observe the patient’s thoracic spine region and | [[File:Thoracic kyphosis.png|right|frameless]] | ||
This should occur from in front, behind and from the side in sitting and standing<ref name=":2" /><ref name=":4">Petty, N, Moore, A, (2002), Neuromuscular Examination and Assessment A Handbook For Therapists, 2 nd Edition, Churchill Livingstone, Edinburgh</ref> | |||
*The examiners observe the patient’s thoracic spine region and assess for the presence of deviation from normal including the thoracic spine curvatures in the frontal and sagittal planes. | |||
*The overall impression of inter-rater reliability for postural observation of kyphosis and label either excessive, normal or decrease range from moderate to substantial according to a study performed by Cleland et al.<ref name="Cleland">Cleland JA, Childs JD, Fritz JM, Whitman JM. Interrater Reliability of the History and Physical Examination in Patients With Mechanical Neck Pain. Arch Phys Med Rehabil 2006 10;87(10):1388-1395.</ref> | *The overall impression of inter-rater reliability for postural observation of kyphosis and label either excessive, normal or decrease range from moderate to substantial according to a study performed by Cleland et al.<ref name="Cleland">Cleland JA, Childs JD, Fritz JM, Whitman JM. Interrater Reliability of the History and Physical Examination in Patients With Mechanical Neck Pain. Arch Phys Med Rehabil 2006 10;87(10):1388-1395.</ref> | ||
*Paying attention to some of the following; symmetry, Cx/Tx/Lx curvatures, deviations of the spine, shoulder levels, shoulder girdle, scapula position, GH joint position, level of the pelvis, limb position | *Paying attention to some of the following; symmetry, Cx/Tx/Lx curvatures, deviations of the spine, shoulder levels, shoulder girdle, scapula position, GH joint position, level of the pelvis, limb position | ||
| Line 166: | Line 142: | ||
*Attitudes and feelings<ref name=":3" /><br> | *Attitudes and feelings<ref name=":3" /><br> | ||
=== Movement Patterns === | |||
The examiner can ask the patient to perform the following movements to check for any change symptoms; looking up, transferring from sit to stand, lifting one or both arms overhead, and any other movements that aggravate or relieve symptoms. While the patient performs these movements watch for any deviations, compensations, or discrepancies between sides. If applicable, any of these movement patterns can be used as asterisk or comparable signs for reassessment after a trial intervention. <ref name=":4" /> | The examiner can ask the patient to perform the following movements to check for any change symptoms; looking up, transferring from sit to stand, lifting one or both arms overhead, and any other movements that aggravate or relieve symptoms. While the patient performs these movements watch for any deviations, compensations, or discrepancies between sides. If applicable, any of these movement patterns can be used as an asterisk or comparable signs for reassessment after a trial intervention. <ref name=":4" /> | ||
=== Palpation === | |||
To begin, palpate superficial structures and then move to the deeper structures of the thorax. Feel for any changes in temperature, texture, and moisture, as well as lymph node and soft tissue swelling. Check for symmetry between bony landmarks including the rib angles and attachments, this can also be done through observation.<ref>Flynn TW, Cleland JA, Whitman JM, Users’ Guide to the Musculoskeletal Examination. Cervicothoracic spine examination. Evidence in Motion, 2008. p72-102.</ref> | To begin, palpate superficial structures and then move to the deeper structures of the thorax. Feel for any changes in temperature, texture, and moisture, as well as lymph node and soft tissue swelling. Check for symmetry between bony landmarks including the rib angles and attachments, this can also be done through observation.<ref>Flynn TW, Cleland JA, Whitman JM, Users’ Guide to the Musculoskeletal Examination. Cervicothoracic spine examination. Evidence in Motion, 2008. p72-102.</ref> | ||
Assessment of skin temperature, soft tissues, muscle tone, tenderness, increased or decreased prominence of bones, position of vertebrae and ribs<br> | Assessment of skin temperature, soft tissues, muscle tone, tenderness, increased or decreased prominence of bones, the position of vertebrae and ribs<br> | ||
*Supine- sternum, ribs, clavicle, sternocostal and costochondral joints | *Supine- sternum, ribs, clavicle, sternocostal and costochondral joints | ||
*Prone- spinous process, costotransverse and costovertebral *Note thoracic facet and costotransverse joints refer pain locally or 1 level above or below | *Prone- spinous process, costotransverse and costovertebral *Note thoracic facet and costotransverse joints refer pain locally or 1 level above or below | ||
*Seated- 1st rib anteriorly and posteriorly<ref name=":3" /><ref name=":4" /> | *Seated- 1st rib anteriorly and posteriorly<ref name=":3" /><ref name=":4" /> | ||
=== Movement Testing === | |||
[[File:Scheuermanns disease.jpg|right|frameless]] | |||
Thoracic Spine AROM, PROM, and Overpressure | Thoracic Spine AROM, PROM, and Overpressure | ||
*Flexion | *Flexion | ||
| Line 185: | Line 161: | ||
*Side-bending | *Side-bending | ||
*Rotation | *Rotation | ||
*Combined Movements (rotation with extension) | *Combined Movements (rotation with extension) | ||
*Assess for baseline symptoms including intensity and location prior to testing. Note changes in intensity and location of symptoms and where in the range they occur during test. | *Assess for baseline symptoms including intensity and location prior to testing. Note changes in intensity and location of symptoms and where in the range they occur during test. | ||
| Line 194: | Line 170: | ||
*Flexion, extension and side-bending may be measured with a double inclinometer method, but no normative values have been found, and reliability of these measurements has not been researched. | *Flexion, extension and side-bending may be measured with a double inclinometer method, but no normative values have been found, and reliability of these measurements has not been researched. | ||
*Rotation and combined movements measured purely on observation.<ref name=":5">Maitland, G, (1991), Vertebral Manipulation, 3 rd Edition, Butterworth Heinemann, London</ref><ref name=":4" /> | *Rotation and combined movements measured purely on observation.<ref name=":5">Maitland, G, (1991), Vertebral Manipulation, 3 rd Edition, Butterworth Heinemann, London</ref><ref name=":4" /> | ||
==== Passive Intervertebral Motion ==== | |||
To access accessory intervertebral motion apply pressure in a posterior to anterior direction to the thoracic spine either centrally directly on the spinous process (central) or unilaterally located just lateral to the spinous process. | To access accessory intervertebral motion apply pressure in a posterior to anterior direction to the thoracic spine either centrally directly on the spinous process (central) or unilaterally located just lateral to the spinous process. | ||
| Line 205: | Line 181: | ||
Thoracic Spine Central PA assessment | Thoracic Spine Central PA assessment | ||
*Intra-rater and inter-rater reliability in the thoracic spine when determining mobility dysfunction was fair when using strict agreement of spinal levels. When the expanded agreement to include one segment above or below intra-rater and inter-rater reliability increased to good to moderate.<ref name="he">Heiderscheit B, Boissonnault W. Reliability of | *Intra-rater and inter-rater reliability in the thoracic spine when determining mobility dysfunction was fair when using strict agreement of spinal levels. When the expanded agreement to include one segment above or below intra-rater and inter-rater reliability increased to good to moderate.<ref name="he">Heiderscheit B, Boissonnault W. [https://www.tandfonline.com/doi/abs/10.1179/106698108790818369 Reliability of joint mobility and pain assessment of the thoracic spine and rib cage in asymptomatic individuals.] Journal of Manual & Manipulative Therapy. 2008 Oct 1;16(4):210-6.</ref> | ||
*Cleland found thoracic spine mobility testing ranged from fair agreement to substantial agreement between each separate segment of the thoracic spine.<ref name="Cleland" /> | *Cleland found thoracic spine mobility testing ranged from fair agreement to substantial agreement between each separate segment of the thoracic spine.<ref name="Cleland" /> | ||
*In the study by Potter, testing for thoracic joint dysfunction using postural observation, active and passive range of motion, palpation, and PAs was rated as poor to moderate for intra-rater reliability.<ref>Potter L, McCarthy C, Oldham J. Intraexaminer Reliability of Identifying a Dysfunctional Segment in the Thoracic and Lumbar Spine. J Manipulative Physiol Ther 2006 4;29(3):203-207.</ref><ref name=":5" /> | *In the study by Potter, testing for thoracic joint dysfunction using postural observation, active and passive range of motion, palpation, and PAs was rated as poor to moderate for intra-rater reliability.<ref>Potter L, McCarthy C, Oldham J. Intraexaminer Reliability of Identifying a Dysfunctional Segment in the Thoracic and Lumbar Spine. J Manipulative Physiol Ther 2006 4;29(3):203-207.</ref><ref name=":5" /> | ||
| Line 222: | Line 198: | ||
*Strict agreement the intra-rater reliability ranged from no agreement to moderate and no agreement for the inter-rater reliability. When the agreement was expanded both intra-rater and inter-rater reliability increased to complete agreement and good respectively.<ref name="he" /> <br> | *Strict agreement the intra-rater reliability ranged from no agreement to moderate and no agreement for the inter-rater reliability. When the agreement was expanded both intra-rater and inter-rater reliability increased to complete agreement and good respectively.<ref name="he" /> <br> | ||
=== Muscle Testing === | |||
Testing both [[muscle]] length and strength is important to identify functional limitations and compensations of each muscle. The measurement serves as a baseline to aid in tracking progress and allows the therapist to properly target impairment with interventions.<br> | Testing both [[muscle]] length and strength is important to identify functional limitations and compensations of each muscle. The measurement serves as a baseline to aid in tracking progress and allows the therapist to properly target impairment with interventions.<br> | ||
<u>Muscle Length Testing</u><ref name=":4" /><ref name="Cleland" /> | <u>Muscle Length Testing</u><ref name=":4" /><ref name="Cleland" /> | ||
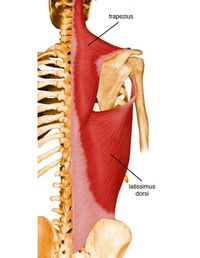
*[[Latissimus Dorsi Muscle|Latissimus Dorsi]] - moderate to substantial inter-rater reliability | *[[File:Latissimus+Dorsi+Origin+Spinous+processes+of+inferior+6+thoracic+vertebrae,+thoracolumbar+fascia,+iliac+crest,+and+inferior+3+or+4+ribs..jpg|right|frameless|258x258px]][[Latissimus Dorsi Muscle|Latissimus Dorsi]] - moderate to substantial inter-rater reliability | ||
*[[Pectoralis major|Pectoralis Major]]- fair to substantial inter-rater reliability | *[[Pectoralis major|Pectoralis Major]]- fair to substantial inter-rater reliability | ||
*[[Pectoralis Minor]]- moderate to substantial inter-rater reliability<br> | *[[Pectoralis Minor]]- moderate to substantial inter-rater reliability<br> | ||
| Line 234: | Line 210: | ||
*Lower Trapezius- no inter-rater reliability | *Lower Trapezius- no inter-rater reliability | ||
*[[Serratus Anterior|Seratus Anterior]]- fair to substantial inter-rater reliability | *[[Serratus Anterior|Seratus Anterior]]- fair to substantial inter-rater reliability | ||
*[[Rhomboids]]- moderate inter-rater reliability<ref name=":3" /><br> | *[[Rhomboids]]- moderate inter-rater reliability<ref name=":3" /><br> | ||
=== Neurologic Assessment === | |||
Questions to help determine the direction of the neurological screen. | Questions to help determine the direction of the neurological screen. | ||
| Line 255: | Line 231: | ||
====Neural Tissue Provocation Tests==== | ====Neural Tissue Provocation Tests==== | ||
* Passive neck flexion | * Passive neck flexion | ||
* Neural tissue provocation tests for the upper limb | * [[Upper Limb Tension Tests (ULTTs)|Neural tissue provocation tests for the upper limb]] | ||
* [[Straight Leg Raise Test|Straight leg raise]] | * [[Straight Leg Raise Test|Straight leg raise]] | ||
* Passive knee bend | * Passive knee bend | ||
* [[Slump Test|Slump]] test<ref name=":4" /> | * [[Slump Test|Slump]] test<ref name=":4" /> | ||
=== Special Tests === | |||
{| class="FCK__ShowTableBorders" width="40%" cellspacing="1" cellpadding="1" border="0" align="right" | {| class="FCK__ShowTableBorders" width="40%" cellspacing="1" cellpadding="1" border="0" align="right" | ||
|- | |- | ||
| Line 271: | Line 248: | ||
*''Kehr’s sign''- With the patient in supine and legs elevated, a report of pain in the supraclavicular area can be secondary to irritants or blood in the peritoneal cavity rather than musculoskeletal involvement. It is a classic symptom for a ruptured spleen and can result from other splenic injuries, renal calculi, diaphragmatic lesions, peridiaphragmatic lesions, or an ectopic pregnancy. | *''Kehr’s sign''- With the patient in supine and legs elevated, a report of pain in the supraclavicular area can be secondary to irritants or blood in the peritoneal cavity rather than musculoskeletal involvement. It is a classic symptom for a ruptured spleen and can result from other splenic injuries, renal calculi, diaphragmatic lesions, peridiaphragmatic lesions, or an ectopic pregnancy. | ||
*"Cervicothoracic tests" - to provoke the patient’s symptoms of neck pain. These clinical tests are part of the examination proceeded in order to establish the differential diagnosis | *"Cervicothoracic tests" - to provoke the patient’s symptoms of neck pain. These clinical tests are part of the examination proceeded in order to establish the differential diagnosis | ||
*''Murphy’s Percussion''- Place hand over costovertebral angle of the back and thump hand with the other fist. If there is a reproduction of back or flank pain this is a positive test and indicative of kidney involvement. | *''Murphy’s Percussion''- Place hand over the costovertebral angle of the back and thump hand with the other fist. If there is a reproduction of back or flank pain this is a positive test and indicative of kidney involvement. | ||
*''Palpate Abdomen:'' | *''Palpate Abdomen:'' | ||
-Right Upper Quadrant: Liver, gallbladder, duodenum, head of pancreas, right kidney and the hepatic flexure of the colon. | -Right Upper Quadrant: Liver, gallbladder, duodenum, head of pancreas, right kidney and the hepatic flexure of the colon. | ||
-Left Upper Quadrant: Stomach, spleen, left lobe of liver, body of pancreas, left kidney and adrenal gland, splenic | -Left Upper Quadrant: Stomach, spleen, left lobe of liver, body of pancreas, left kidney and adrenal gland, splenic flexure of colon, and parts of the transverse descending colon. | ||
-Right Lower Quadrant: Cecum, appendix, ascending colon, right ovary and fallopian tube and right ureter. | -Right Lower Quadrant: Cecum, appendix, ascending colon, right ovary and fallopian tube and right ureter. | ||
| Line 286: | Line 263: | ||
*''Thoracic Excursion''- Thoracic excursion can be measured on a patient you suspect decreased chest expansion, including ankylosing spondylitis. Using a cloth measuring tape and standardized measuring locations (5th thoracic spinous process/3rd intercostal space and 10th thoracic spinous process/xyphoid process) have the patient exhale completely and take the measurement, then have them inhale to their full capacity and record the measurement. <ref name=":3" /> | *''Thoracic Excursion''- Thoracic excursion can be measured on a patient you suspect decreased chest expansion, including ankylosing spondylitis. Using a cloth measuring tape and standardized measuring locations (5th thoracic spinous process/3rd intercostal space and 10th thoracic spinous process/xyphoid process) have the patient exhale completely and take the measurement, then have them inhale to their full capacity and record the measurement. <ref name=":3" /> | ||
== Outcome Measures == | |||
There are no validated region specific outcome tools for the thoracic spine, the following are recommended but require validation for use with patients with primary thoracic disorders:<br> | There are no validated region specific outcome tools for the thoracic spine, the following are recommended but require validation for use with patients with primary thoracic disorders:<br> | ||
*[[Neck Disability Index]] (NDI) for upper thoracic complaints | *[[Neck Disability Index]] (NDI) for upper thoracic complaints | ||
*[[Occiput to Wall Distance OWD|Occiput to Wall Distance]] | |||
*[[Oswestry Disability Index]] (ODI) for lower thoracic complaints | *[[Oswestry Disability Index]] (ODI) for lower thoracic complaints | ||
*[[Numeric Pain Rating Scale]] (NPRS) where patient is able to rate their pain on a scale of 0 (none) to 10 (severe). | *[[Numeric Pain Rating Scale]] (NPRS) where patient is able to rate their pain on a scale of 0 (none) to 10 (severe). | ||
*[[Patient Specific Functional Scale]] (PSFS) can be used to measure activity limitations and to compare progress from the baseline measurement. | *[[Patient Specific Functional Scale]] (PSFS) can be used to measure activity limitations and to compare progress from the baseline measurement. | ||
*[[Fingertips to Floor Distance - Special Test|Fingertips to floor]] (special test) | |||
== Conclusion == | == Conclusion == | ||
Latest revision as of 00:01, 11 December 2020
Original Editor - Cassidy Lake and Kristen Templin as part of the Temple University EBP Project
Top Contributors - Cassidy Lake, Kristen Templin, Lucinda hampton, Kim Jackson, Admin, Adam Vallely Farrell, George Prudden, Rachael Lowe, Evan Thomas, Naomi O'Reilly, Kai A. Sigel, WikiSysop, Scott A Burns, Laura Ritchie, Joshua Samuel, Wanda van Niekerk, Khloud Shreif, Tony Lowe and Aminat Abolade
Introduction[edit | edit source]

The Thoracic Spine has a complex and often overlooked role within the body. It is a key area of load transfer between the upper and lower body and for rotational movement within the body.
- Should be assessed and treated as a functional unit including not only the spine but the rib cage.
- The thoracic region provides a site for muscle and connective tissue attachments from the head, neck, shoulder blade, clavicle, lumbar spine and pelvis as well as connections to organs in the rib cage and abdomen.
- It has a role in breathing, is protection for vital organs, and has a relationship to emotions and the nerves that control the ‘fight or flight’ response.
Watch this 5-minute showing of a thoracic examination by a physiotherapist
Initial Diagnosis[edit | edit source]
When observing and assessing client be aware of the common causes of thoracic spine pain, so you can screen for them, beginning the elimination process towards diagnosis.
- Sprain or strain; Spinal joint sprain involving the disc or zygapophyseal (facet) joint; rib joint sprain; muscle strain.
- Reduced thoracic mobility may be due to; rib cage, spinous processes, zygapophyseal joint capsules, ligamentum flavum, dimensions of the vertebral bodies.
- Scheuermanns syndrome in adolescents
- Postural and overuse syndromes in students and office-based workers
- Less common causes - Rib or compression fractures, thoracic outlet syndrome and T4 syndrome.
- Red flags eg cardiac or lung conditions (pneumothorax, pulmonary embolism), peptic ulcers, tumours and mesothelioma after exposure to asbestos.[2]
Functional Anatomy[edit | edit source]
![[3]](/File:Thoracic_spondylolysis.png)
The function of the thoracic spine and ribcage is the:
- protection of the heart, lungs and viscera, ventilation of the lungs
- provide a stable base for the attachment of muscles of the upper limbs, head and neck, vertebral column and the pelvis.[4] [5](at the expense of mobility).
- The thoracic spine:
- lies between the superior cervical spine and the inferior lumbar spine. It
- consists of 12 vertebrae, the bodies of the thoracic vertebrae are medium-sized and heart-shaped,[6] generally increase in size from superiorly to inferiorly to support increase the increases in weight that needs to be supported.
- possess articular facets on their sides for articulation with the heads of the ribs.[6][5]
2. The rib cage consists of 12 pairs of ribs:
- 1 st – 7th ribs: (true) attach directly to the sternum
- 8th – 10th ribs: articulate with sternum via the costal cartilages above them
- 11th and 12th ribs: floating ribs as they do not attach to sternum[4]
Subjective Assessment[edit | edit source]
Symptoms (Recorded on a Body Chart)[edit | edit source]
Area[edit | edit source]
- Distribution
Type[edit | edit source]
- Quality
- Intensity
- VAS
- Pain diary may be useful for chronic pain patients
- Depth
- Abnormal sensation
- Paraesthesia
- Numbness
- Constant/Intermittent
- If, constant, check whether there is variation in the intensity of symptoms
- Constant unremitting pain may be indicative of neoplastic disease
Behaviour[7][edit | edit source]
- Aggravating factors
- Deep breathing, rotation of the thorax
- Easing factors
- Thoracic extension
- Severity and irritability
- Used to identify those who will not be able to tolerate a full objective examination
- Severity - If a patient is able to sustain a position that reproduces the symptoms then the condition is considered non-severe. If the patient cannot sustain the position, the condition is considered severe and no overpressures should be attempted
- Irritability- If symptoms ease immediately after provocation then the condition is considered to be non-irritable and all movements can be tested. If symptoms take a few minutes to ease, the symptoms are irritable and only a few movements should be attempted to avoid exacerbating the patients’ symptoms
- 24hr symptoms- Night, morning and evening symptoms (morning stiffness for a few minutes suggests spondylosis, stiffness and pain for a few hours suggests inflammatory processes such as A.S.) Position of sleep, no. of pillows, do symptoms affect sleep? Soft or firm mattress?
- Improving, staying the same, getting worse[7]
Special Questions[edit | edit source]

Special questions are used to identify precautions or absolute contraindications to examination or treatment
- General health
- Weight loss
- RA
- Drug therapy
- X-rays and medical imaging
- Neurological symptoms
History of Present Condition (HPC)[edit | edit source]
- Known or unknown cause
- Sudden/slow onset
- How long ago did symptoms start
- Route to physiotherapy
Past Medical History (PMH)[edit | edit source]
- Relevant medical history
- Previous episodes
- Previous Rx
Social History[edit | edit source]
- Employment, dependants, leisure activities etc.
Region-Specific Historical Examination[edit | edit source]
The thoracic area is a common place for the cervical spine to refer symptoms, so screen the cervical spine including assessing for previous neck pain or neck trauma is necessary to rule out cervical spine involvement.[8][5] eg “Do neck movements improve your symptoms?” “Where is the pain most bothersome?”
Special Questions[edit | edit source]

Red Flags[edit | edit source]
- Thoracic spine pain and visceral pain can mimic the other due to the shared afferent innervation of the ANS sympathetics, which originate from T1-L2 afferents from the spinal cord.[9]
- Segments T4-T7 have the potential to cause pseudoanginal pain as well as symptoms generated by a cough, sneeze, deep breath, movement of the trunk, palpation, and compression.[10]
- See also Thoracic Back Pain Red Flags
Yellow Flags[edit | edit source]
- Fear-Avoidance Beliefs Questionnaire (FABQ) can be used to screen for behaviours that may require a consult or an increase in treatment duration.
- Patients involved in on-going litigation have been found to have reduced changes in quality of life and higher rates of disability with the physical gains made in therapy.[11]
Investigations[edit | edit source]
Looking for serious pathology
- Diagnostic Imaging Considerations- Patients that present with acute thoracic spine pain with risk factors for osteoporotic compression fractures should have standard thoracic spine radiographs.
- Radiographs are sensitive to assess for acute compression fractures; however, if the patient’s initial radiographs were read as normal and they are still experiencing extreme pain or symptoms consider a referral for advanced imaging such as CT or MRI.
- Patients with red flags for cancer should be referred for imaging to rule out cancer.
- Patients with suspected Ankylosing Spondylitis are typically referred for radiographs of the sacroiliac joints and lab studies including assessing for the presence of HLA-B27.
Objective Examination[edit | edit source]
Observation[edit | edit source]

This should occur from in front, behind and from the side in sitting and standing[5][12]
- The examiners observe the patient’s thoracic spine region and assess for the presence of deviation from normal including the thoracic spine curvatures in the frontal and sagittal planes.
- The overall impression of inter-rater reliability for postural observation of kyphosis and label either excessive, normal or decrease range from moderate to substantial according to a study performed by Cleland et al.[13]
- Paying attention to some of the following; symmetry, Cx/Tx/Lx curvatures, deviations of the spine, shoulder levels, shoulder girdle, scapula position, GH joint position, level of the pelvis, limb position
- Muscle bulk and tone (compare sides, hand dominance)
- Soft tissues (Skin colour and quality, Swelling, scars)
- Gait (Trendelenburg gait, short leg gait)
- Attitudes and feelings[7]
Movement Patterns[edit | edit source]
The examiner can ask the patient to perform the following movements to check for any change symptoms; looking up, transferring from sit to stand, lifting one or both arms overhead, and any other movements that aggravate or relieve symptoms. While the patient performs these movements watch for any deviations, compensations, or discrepancies between sides. If applicable, any of these movement patterns can be used as an asterisk or comparable signs for reassessment after a trial intervention. [12]
Palpation[edit | edit source]
To begin, palpate superficial structures and then move to the deeper structures of the thorax. Feel for any changes in temperature, texture, and moisture, as well as lymph node and soft tissue swelling. Check for symmetry between bony landmarks including the rib angles and attachments, this can also be done through observation.[14]
Assessment of skin temperature, soft tissues, muscle tone, tenderness, increased or decreased prominence of bones, the position of vertebrae and ribs
- Supine- sternum, ribs, clavicle, sternocostal and costochondral joints
- Prone- spinous process, costotransverse and costovertebral *Note thoracic facet and costotransverse joints refer pain locally or 1 level above or below
- Seated- 1st rib anteriorly and posteriorly[7][12]
Movement Testing[edit | edit source]

Thoracic Spine AROM, PROM, and Overpressure
- Flexion
- Extension
- Side-bending
- Rotation
- Combined Movements (rotation with extension)
- Assess for baseline symptoms including intensity and location prior to testing. Note changes in intensity and location of symptoms and where in the range they occur during test.
- Ensure the motion is purely thoracic by ensuring the patient is not compensating with lumbar and pelvis movement.
- Repeated motion may be performed to assess for centralization of symptoms or a directional preference.
- Repeated motion testing has been predominately studied for lumbar and cervical spine at this time.
- The normal end feel for all the motions listed is firm.
- Flexion, extension and side-bending may be measured with a double inclinometer method, but no normative values have been found, and reliability of these measurements has not been researched.
- Rotation and combined movements measured purely on observation.[15][12]
Passive Intervertebral Motion[edit | edit source]
To access accessory intervertebral motion apply pressure in a posterior to anterior direction to the thoracic spine either centrally directly on the spinous process (central) or unilaterally located just lateral to the spinous process.
Rib motion may be accessed in two locations, posterior to anterior pressure applied to the rib angles and anterior to posterior pressure applied at the costosternal joints.
The examiner assesses for pain provocation and mobility of each joint and determines whether it is hypomobile, hypermobile or normal. Also note pain provocation.[15]
Reliability of Thoracic Spine Passive Accessory[edit | edit source]
Thoracic Spine Central PA assessment
- Intra-rater and inter-rater reliability in the thoracic spine when determining mobility dysfunction was fair when using strict agreement of spinal levels. When the expanded agreement to include one segment above or below intra-rater and inter-rater reliability increased to good to moderate.[16]
- Cleland found thoracic spine mobility testing ranged from fair agreement to substantial agreement between each separate segment of the thoracic spine.[13]
- In the study by Potter, testing for thoracic joint dysfunction using postural observation, active and passive range of motion, palpation, and PAs was rated as poor to moderate for intra-rater reliability.[17][15]
Rib Cage
- The intra-rater reliability was found to be fair with strict agreement and increased to good with expanded agreement.[16]
Reliability of Pain Provocation[edit | edit source]
Central Thoracic PAs
- Intra-rater pain provocation with strict agreement ranged from fair to good and inter-rater reliability was fair. When the agreement was expanded intra-rater reliability was increased to very good and inter-rater reliability increased to good.[16]
- Pain provocation had a similar variance across the thoracic spine with a range from no agreement to substantial agreement.[13][15]
Rib Cage
- Strict agreement the intra-rater reliability ranged from no agreement to moderate and no agreement for the inter-rater reliability. When the agreement was expanded both intra-rater and inter-rater reliability increased to complete agreement and good respectively.[16]
Muscle Testing[edit | edit source]
Testing both muscle length and strength is important to identify functional limitations and compensations of each muscle. The measurement serves as a baseline to aid in tracking progress and allows the therapist to properly target impairment with interventions.
- Latissimus Dorsi - moderate to substantial inter-rater reliability
- Pectoralis Major- fair to substantial inter-rater reliability
- Pectoralis Minor- moderate to substantial inter-rater reliability

- Middle Trapezius- no inter-rater reliability
- Lower Trapezius- no inter-rater reliability
- Seratus Anterior- fair to substantial inter-rater reliability
- Rhomboids- moderate inter-rater reliability[7]
Neurologic Assessment[edit | edit source]
Questions to help determine the direction of the neurological screen.
- Do you get symptoms into the legs or low back with neck movements?
If yes, perform a detailed neurological examination
- Have you experienced any bilateral upper extremity symptoms or occasional loss of balance or lack of coordination in the lower extremities?
If yes, perform a detailed neurological examination
- Upper Motor Neuron Reflexes (Hoffman, Babinski, Clonus)
- Sensory Testing: T1 dermatome (medial forearm)
- T1 Nerve Root Level: first dorsal interossei
- Upper Quarter Neurologic Screen for upper thoracic
- Lower Quarter Neurologic Screen for lower thoracic
Neural Tissue Provocation Tests[edit | edit source]
- Passive neck flexion
- Neural tissue provocation tests for the upper limb
- Straight leg raise
- Passive knee bend
- Slump test[12]
Special Tests[edit | edit source]
| [18] |
- Cervical Rotation Lateral Flexion (CRLF) Test- If first rib elevation or hypomobility is suspected.
- Slump Test- To determine neural tension.
- Adsons test - provocative test for Thoracic Outlet Syndrome accompanied by compression of the Subclavian artery by a cervical rib or tightened anterior and middle scalene muscles
- Kehr’s sign- With the patient in supine and legs elevated, a report of pain in the supraclavicular area can be secondary to irritants or blood in the peritoneal cavity rather than musculoskeletal involvement. It is a classic symptom for a ruptured spleen and can result from other splenic injuries, renal calculi, diaphragmatic lesions, peridiaphragmatic lesions, or an ectopic pregnancy.
- "Cervicothoracic tests" - to provoke the patient’s symptoms of neck pain. These clinical tests are part of the examination proceeded in order to establish the differential diagnosis
- Murphy’s Percussion- Place hand over the costovertebral angle of the back and thump hand with the other fist. If there is a reproduction of back or flank pain this is a positive test and indicative of kidney involvement.
- Palpate Abdomen:
-Right Upper Quadrant: Liver, gallbladder, duodenum, head of pancreas, right kidney and the hepatic flexure of the colon.
-Left Upper Quadrant: Stomach, spleen, left lobe of liver, body of pancreas, left kidney and adrenal gland, splenic flexure of colon, and parts of the transverse descending colon.
-Right Lower Quadrant: Cecum, appendix, ascending colon, right ovary and fallopian tube and right ureter.
-Left Lower Quadrant: Left ovary and fallopian tube, left ureter, descending colon and sigmoid colon.
- Palpation of the Aortic Pulse in the Abdomen- Use this test on patients at risk for an abdominal aortic aneurysm. Place the patient in a supine hooklying position with the abdominal muscles on slack. Palpate to the left of the patient’s navel feeling for a pulse, once felt continue laterally until the pulse can no longer be detected. If the distance the pulse is detected is > 2.5 cm refer the patient for additional diagnostic studies.
- Rebound Tenderness- Place hand on abdomen in an area away from suspected inflammation, slowly and deeply palpate. Quickly remove hand. If the patient feels pain on release this is called rebound tenderness and can be indicative of an inflamed peritoneum.
- Thoracic Excursion- Thoracic excursion can be measured on a patient you suspect decreased chest expansion, including ankylosing spondylitis. Using a cloth measuring tape and standardized measuring locations (5th thoracic spinous process/3rd intercostal space and 10th thoracic spinous process/xyphoid process) have the patient exhale completely and take the measurement, then have them inhale to their full capacity and record the measurement. [7]
Outcome Measures[edit | edit source]
There are no validated region specific outcome tools for the thoracic spine, the following are recommended but require validation for use with patients with primary thoracic disorders:
- Neck Disability Index (NDI) for upper thoracic complaints
- Occiput to Wall Distance
- Oswestry Disability Index (ODI) for lower thoracic complaints
- Numeric Pain Rating Scale (NPRS) where patient is able to rate their pain on a scale of 0 (none) to 10 (severe).
- Patient Specific Functional Scale (PSFS) can be used to measure activity limitations and to compare progress from the baseline measurement.
- Fingertips to floor (special test)
Conclusion[edit | edit source]
Pain in the upper part of their back (the thoracic spine) is a common complaint.
- This is sometimes present in the thorax alone
- Often accompanied by symptoms in the neck or lumbar spine.
- Symptoms range from feelings of stiffness to burning muscular pain, pain often associated with the retention of static postures.
- Assessment of the region which links the cervical and lumbar spines is crucial and yet overlooked by many therapists.
If you are new to using ROM tests, and when you are first practicing, it is always useful to ask clients to perform the movements in the same order. That way you are unlikely to miss out any movement. However, as you become more experienced, one tip is to leave the movement that you think might be most aggravating until last. You are likely to have some idea as to which movement this might be based on what your client has told you during your consultation.[19]
References[edit | edit source]
- ↑ PTN Thoracic examination Available from:https://www.youtube.com/watch?v=FJtjB6lnObU&app=desktop (last accessed 15.4.2020)
- ↑ Lifecare North sports Clinic Thoracic spine Available from: https://www.lifecare.com.au/clinic/northern-sports-physiotherapy-clinic/news/thoracic-spine/ (last accessed 15.4.2020)
- ↑ Thoracic Vertebrae
- ↑ 4.0 4.1 Oliver, J., Middleditch, A., (1991), Functional Anatomy of the Spine, Butterworth-Heinemann, Oxford
- ↑ 5.0 5.1 5.2 5.3 Levangie P, Norkin C, (2001), Joint Structure and Function; A Comprehensive Analysis, 3 rd Edition, F.A. Davis Company, Philadelphia
- ↑ 6.0 6.1 Thoracic Vertebrae. (2018, January 15). Physiopedia, . Retrieved 13:45, January 28, 2018 from https://www.physio-pedia.com/index.php?title=Thoracic_Vertebrae&oldid=182308.
- ↑ 7.0 7.1 7.2 7.3 7.4 7.5 7.6 Magee, D, (2002) Orthopedic Physical Assessment, 4 th Edition, Saunders, London
- ↑ Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. Reliability and diagnostic accuracy of the clinical examination and patient self-report measures for cervical radiculopathy. Spine. 2003 Jan 1;28(1):52-62.
- ↑ Benhamou CL, Roux C, Tourliere D, Gervais T, Viala JF, Amor B. Pseudovisceral pain referred from costovertebral arthropathies: twenty-eight cases. Spine. 1993 May 1;18(6):790-5.
- ↑ Hamberg J, Lindahl O. Angina pectoris symptoms caused by thoracic spine disorders. Clinical examination and treatment. Acta Medica Scandinavica. 1981 Jan 12;209(S644):84-6.
- ↑ Blake C, Garrett M. Impact of litigation on quality of life outcomes in patients with chronic low back pain. Irish journal of medical science. 1997 Jul 1;166(3):124-6.
- ↑ 12.0 12.1 12.2 12.3 12.4 12.5 12.6 Petty, N, Moore, A, (2002), Neuromuscular Examination and Assessment A Handbook For Therapists, 2 nd Edition, Churchill Livingstone, Edinburgh
- ↑ 13.0 13.1 13.2 13.3 13.4 Cleland JA, Childs JD, Fritz JM, Whitman JM. Interrater Reliability of the History and Physical Examination in Patients With Mechanical Neck Pain. Arch Phys Med Rehabil 2006 10;87(10):1388-1395.
- ↑ Flynn TW, Cleland JA, Whitman JM, Users’ Guide to the Musculoskeletal Examination. Cervicothoracic spine examination. Evidence in Motion, 2008. p72-102.
- ↑ 15.0 15.1 15.2 15.3 Maitland, G, (1991), Vertebral Manipulation, 3 rd Edition, Butterworth Heinemann, London
- ↑ 16.0 16.1 16.2 16.3 Heiderscheit B, Boissonnault W. Reliability of joint mobility and pain assessment of the thoracic spine and rib cage in asymptomatic individuals. Journal of Manual & Manipulative Therapy. 2008 Oct 1;16(4):210-6.
- ↑ Potter L, McCarthy C, Oldham J. Intraexaminer Reliability of Identifying a Dysfunctional Segment in the Thoracic and Lumbar Spine. J Manipulative Physiol Ther 2006 4;29(3):203-207.
- ↑ Physical Therapy Nation. Lindgren's Test for First Rib Dysfunction. Available from: http://www.youtube.com/watch?v=U7ZRo09Vn04 [last accessed 14/12/13]
- ↑ Musculoskeletal Thoracic assessment Available from:https://musculoskeletalkey.com/thoracic-assessment/ (last accessed 15.4.2020)

