Deltoid: Difference between revisions
No edit summary |
No edit summary |
||
| Line 8: | Line 8: | ||
The Deltoid muscle is a large triangular shaped muscle which lies over the [[Glenohumeral Joint|glenohumeral joint]] and which gives the [[shoulder]] its rounded contour. | The Deltoid muscle is a large triangular shaped muscle which lies over the [[Glenohumeral Joint|glenohumeral joint]] and which gives the [[shoulder]] its rounded contour. | ||
* | * It is comprised of three distinct portions (anterior or clavicular, middle or acromial, and posterior or spinal) | ||
* | * Acts mainly as an abductor of the shoulder and stabiliser of the humeral head. as well as assists in forward elevation<ref name=":1">Moser T, Lecours J, Michaud J, Bureau NJ, Guillin R, Cardinal É. [https://pubmed.ncbi.nlm.nih.gov/23784480/ The deltoid, a forgotten muscle of the shoulder.] Skeletal radiology. 2013 Oct;42(10):1361-75.Available:https://pubmed.ncbi.nlm.nih.gov/23784480/ (accessed 5.1.2022)</ref>. | ||
* The deltoid is a very powerful muscle and is used in many types | * The deltoid is a very powerful muscle and is used in many ADL's (eg putting clothes in line, carrying shopping types, washing hair) and many athletic activities. eg netball, swimming, water polo.<ref>Sports MD [https://www.sportsmd.com/sports-injuries/shoulder-injuries/deltoid-strain/ Deltoid strain] Available: https://www.sportsmd.com/sports-injuries/shoulder-injuries/deltoid-strain/<nowiki/>(accessed 5.1.2021)</ref> | ||
Image 1: Deltoid Muscle overlying shoulder complex. | Image 1: Deltoid Muscle overlying shoulder complex. | ||
== Anatomy == | == Anatomy == | ||
=== Origin === | === Origin === | ||
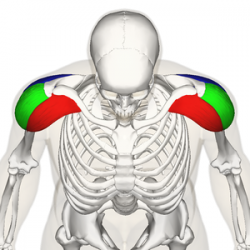
'''Anterior Fibres/Head''' | # [[File:Deltoid_muscle_Wikipedia.png|alt=|right|250x250px]]'''Anterior Fibres/Head:''' Lateral third, Anterior Surface of the Clavicle (close to the lateral fibres of pectoralis major). | ||
# '''Mid/Lateral Head:''' Acromion Process, Superior Surface. | |||
Lateral third, Anterior Surface of the Clavicle (close to the lateral fibres of pectoralis major). | # '''Posterior Head:''' Spine of the [[Scapula]], Posterior Border. | ||
'''Mid/Lateral Head''' | |||
Acromion Process, Superior Surface. | |||
'''Posterior Head''' | |||
Spine of the [[Scapula]], Posterior Border. | |||
=== Insertion === | === Insertion === | ||
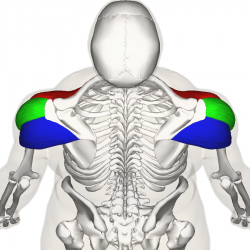
Fibres from all heads converge to insert into the deltoid tuberosity on the humerus. | * [[File:Deltoid_Muscle_top9.png|alt=|right|250x250px]]Fibres from all heads converge to insert into the deltoid tuberosity on the humerus. | ||
* The deltoid fascia is continuous with the brachial fascia and connects to the medial and lateral intermuscular septa<ref>Rispoli, Damian M.; Athwal, George S.; Sperling, John W.; Cofield, Robert H. (2009). "The anatomy of the deltoid insertion". J Shoulder Elbow Surg 18: 386–390</ref>. | |||
The deltoid fascia is continuous with the brachial fascia and connects to the medial and lateral intermuscular septa<ref>Rispoli, Damian M.; Athwal, George S.; Sperling, John W.; Cofield, Robert H. (2009). "The anatomy of the deltoid insertion". J Shoulder Elbow Surg 18: 386–390</ref>. | |||
=== Nerve Supply === | === Nerve Supply === | ||
Axillary Nerve, C5 & 6, posterior cord of the [[brachial plexus]]. | [[Axillary Nerve Injury|Axillary Nerve]], C5 & 6, posterior cord of the [[brachial plexus]]. | ||
=== Blood Supply === | === Blood Supply === | ||
| Line 53: | Line 37: | ||
An important function of deltoid is the prevention of subluxation or even dislocation of the head of the humerus particularly when carrying a load. Deltoid is the prime mover of shoulder abduction. | An important function of deltoid is the prevention of subluxation or even dislocation of the head of the humerus particularly when carrying a load. Deltoid is the prime mover of shoulder abduction. | ||
Clinical relevance: Rotator cuff tears place more strain on the deltoid to prevent abduction motion loss. Fatigue or injury to the deltoid may result in a precipitous decline in abduction.<ref>Dyrna F, Kumar NS, Obopilwe E, Scheiderer B, Comer B, Nowak M, Romeo AA, Mazzocca AD, Beitzel K. [https://pubmed.ncbi.nlm.nih.gov/29741391/ Relationship between deltoid and rotator cuff muscles during dynamic shoulder abduction: a biomechanical study of rotator cuff tear progression.] The American journal of sports medicine. 2018 Jul;46(8):1919-26.Available: https://pubmed.ncbi.nlm.nih.gov/29741391/<nowiki/>(accessed 5.1.2022)</ref> | |||
=== Actions === | === Actions === | ||
| Line 68: | Line 54: | ||
== Clinical Relevance == | == Clinical Relevance == | ||
Deltoid pathologies can lead to functional disfunction of the shoulder complex | |||
* Tears are not infrequently associated with large or massive rotator cuff tears and may further jeopardize shoulder function. | |||
* A variety of other pathologies may affect the deltoid muscle including enthesitis, calcific tendinitis, myositis, infection, tumors, and chronic avulsion injury. | |||
* The deltoid muscle and its innervating axillary nerve may be injured during shoulder surgery, which may have disastrous functional consequences. | |||
* Axillary neuropathies leading to deltoid muscle dysfunction and cause denervation of the deltoid muscle. | |||
* Abnormalities of the deltoid may originate from nearby pathologies of subdeltoid bursa, acromion, and distal clavicle.<ref name=":1" /> | |||
* During dislocation of the shoulder or fracture of surgical neck of the humerus axillary nerve may be injured. The [[Axillary Nerve Injury|damage to axillary nerve]] leads to paralysis of deltoid muscle.<ref name=":0">Chaurasia BD. [https://www.pdfdrive.com/bd-chaurasia-books.html Human Anatomy Regional and Applied Dissection and Clinical]. Vol 1. CBS Publishers and Distributors Pvt Ltd, 2010</ref> | |||
== Trigger Point | == Trigger Point Referral Patterns == | ||
<div class="flex-row row"> | <div class="flex-row row"> | ||
Revision as of 05:39, 5 January 2022
Original Editor - Wendy Walker
Lead Editors - Lucinda hampton, Sai Kripa, Wendy Walker, Naomi O'Reilly, Joao Costa, Chrysolite Jyothi Kommu, Andeela Hafeez, Kim Jackson, Vidya Acharya, WikiSysop, Aminat Abolade, Admin, Evan Thomas, George Prudden, Uchechukwu Chukwuemeka and Wanda van Niekerk
Description[edit | edit source]

The Deltoid muscle is a large triangular shaped muscle which lies over the glenohumeral joint and which gives the shoulder its rounded contour.
- It is comprised of three distinct portions (anterior or clavicular, middle or acromial, and posterior or spinal)
- Acts mainly as an abductor of the shoulder and stabiliser of the humeral head. as well as assists in forward elevation[1].
- The deltoid is a very powerful muscle and is used in many ADL's (eg putting clothes in line, carrying shopping types, washing hair) and many athletic activities. eg netball, swimming, water polo.[2]
Image 1: Deltoid Muscle overlying shoulder complex.
Anatomy[edit | edit source]
Origin[edit | edit source]
- Anterior Fibres/Head: Lateral third, Anterior Surface of the Clavicle (close to the lateral fibres of pectoralis major).
- Mid/Lateral Head: Acromion Process, Superior Surface.
- Posterior Head: Spine of the Scapula, Posterior Border.

Insertion[edit | edit source]
- Fibres from all heads converge to insert into the deltoid tuberosity on the humerus.
- The deltoid fascia is continuous with the brachial fascia and connects to the medial and lateral intermuscular septa[3].

Nerve Supply[edit | edit source]
Axillary Nerve, C5 & 6, posterior cord of the brachial plexus.
Blood Supply[edit | edit source]
Deltoid receives its blood supply from the posterior circumflex humeral artery.
Function[edit | edit source]
An important function of deltoid is the prevention of subluxation or even dislocation of the head of the humerus particularly when carrying a load. Deltoid is the prime mover of shoulder abduction.
Clinical relevance: Rotator cuff tears place more strain on the deltoid to prevent abduction motion loss. Fatigue or injury to the deltoid may result in a precipitous decline in abduction.[4]
Actions [edit | edit source]
All heads of deltoid work together to produce abduction of the Shoulder Joint. In addition, each individual head produces the following:
Anterior Fibres
- Flexes, abducts, medially rotates, and horizontally flexes the arm at the shoulder joint
Posterior Fibres
- Extends, abducts, laterally rotates, and horizontally extends the arm at the shoulder joint.
Clinical Relevance[edit | edit source]
Deltoid pathologies can lead to functional disfunction of the shoulder complex
- Tears are not infrequently associated with large or massive rotator cuff tears and may further jeopardize shoulder function.
- A variety of other pathologies may affect the deltoid muscle including enthesitis, calcific tendinitis, myositis, infection, tumors, and chronic avulsion injury.
- The deltoid muscle and its innervating axillary nerve may be injured during shoulder surgery, which may have disastrous functional consequences.
- Axillary neuropathies leading to deltoid muscle dysfunction and cause denervation of the deltoid muscle.
- Abnormalities of the deltoid may originate from nearby pathologies of subdeltoid bursa, acromion, and distal clavicle.[1]
- During dislocation of the shoulder or fracture of surgical neck of the humerus axillary nerve may be injured. The damage to axillary nerve leads to paralysis of deltoid muscle.[6]
Trigger Point Referral Patterns[edit | edit source]


Techniques[edit | edit source]
Palpation[edit | edit source]
Flex elbow to 90 degrees and have patient abduct the shoulder against resistance.
Anterior Fibers
- Deltoid palpated with elbow extended, shoulder 90 degrees abduction and then resist horizontal adduction.
Posterior Fibers
- Position same as above and then resist horizontal abduction.
Length Tension Testing[edit | edit source]
Length Tension Testing for Anterior Deltoid-[edit | edit source]
- The position of patient will be high sitting
- Mark the origin and insertion of anterior deltoid on patient's shoulder by palpating from 1/3rd of clavicle to deltoid tuberosity for better understanding
- The therapist will be standing behind the patient holding the testing shoulder
- The primary function of anterior deltoid is flexion, internal rotation and horizontal adduction
- In order to stress this muscle and to check for length test, we are going reverse the action by extension, external rotation and horizontal abduction without letting the torso rotate
- While performing extension and external rotation, place your one hand on the patient forearm and with the other hand push the shoulder anterior from posterior thereby lengthening the muscle
Length Tension Testing for Posterior Deltoid[edit | edit source]
- The position of patient will be high sitting
- Mark the origin and insertion of posterior deltoid on patient's shoulder by palpating the spine of scapula to deltoid tuberosity for better understanding
- The therapist will be standing in front of the patient initially and moving back to the patient later for better length assessment
- The primary function of posterior deltoid is extension, external rotation and horizontal abduction
- In order to stress this muscle and to check for length test, we are going to reverse the action by flexion, internal rotation and horizontal adduction
- While performing flexion, internal rotation and horizontal adduction, place your one hand on the patient's shoulder and the other hand on patient's forearm
- Moreover, if we want to, perform flexion, internal rotation and horizontal adduction by bringing the patient's shoulder against the chest and therapist moving to the back of the patient by holding the patient's shoulder and forearm thereby lengthening the muscle.
Treatment[edit | edit source]
Exercises:[7]
Supine active assisted:
Lie down flat on your back, with a pillow supporting your head.
Bend your elbow as far as possible. Then raise your arm to 90 degrees vertical, using the stronger arm to assist if necessary. Once you have got to 90 degrees, you can straighten your elbow. Hold your arm in this upright position with its own strength.
Circles: Slowly with your fingers, wrist and elbow straight move the arm in small circular movements clockwise and counterclockwise. Gradually increase the circle as comfortable (this may take a few weeks to increase to bigger and bigger circles).
Progress to light weight:
As you get more confidence in controlling your shoulder movement, a lightweight e.g. a tin of beans or small paperweight, should be held in the affected hand.
Progress to sitting and standing:
Having more confidence in controlling your shoulder movement gradually go from lying down to sitting and eventually standing.
At this stage you may recline the head of your bed or put some pillows underneath your back to recline your position.
Repeat the same exercise again, this time against some gravity.
Start again from holding your arm in the upright position with its own strength.
Start first without any weights and progress to use the same lightweight you used before in the lying down position.
Resisted exercise:
For re-education of concentric contracture of the deltoid muscle.
Make a fist with the hand of the affected side. The flat hand of the opposite side is providing resistance. Push your affected side hand against resistance from the other hand. Whilst doing this, you will notice that you can fully elevate your arm (above your head).
Repeat these exercises in order to ‘learn’ and re-educate your Deltoid muscle to perform this ‘concentric contracture’ even without pushing against your other arm.
References[edit | edit source]
- ↑ 1.0 1.1 Moser T, Lecours J, Michaud J, Bureau NJ, Guillin R, Cardinal É. The deltoid, a forgotten muscle of the shoulder. Skeletal radiology. 2013 Oct;42(10):1361-75.Available:https://pubmed.ncbi.nlm.nih.gov/23784480/ (accessed 5.1.2022)
- ↑ Sports MD Deltoid strain Available: https://www.sportsmd.com/sports-injuries/shoulder-injuries/deltoid-strain/(accessed 5.1.2021)
- ↑ Rispoli, Damian M.; Athwal, George S.; Sperling, John W.; Cofield, Robert H. (2009). "The anatomy of the deltoid insertion". J Shoulder Elbow Surg 18: 386–390
- ↑ Dyrna F, Kumar NS, Obopilwe E, Scheiderer B, Comer B, Nowak M, Romeo AA, Mazzocca AD, Beitzel K. Relationship between deltoid and rotator cuff muscles during dynamic shoulder abduction: a biomechanical study of rotator cuff tear progression. The American journal of sports medicine. 2018 Jul;46(8):1919-26.Available: https://pubmed.ncbi.nlm.nih.gov/29741391/(accessed 5.1.2022)
- ↑ Availble from: Kenhub - Learn Human Anatomy. Deltoid Muscle: Origin, Insertion & Action {last accessed 29 April 2020}
- ↑ Chaurasia BD. Human Anatomy Regional and Applied Dissection and Clinical. Vol 1. CBS Publishers and Distributors Pvt Ltd, 2010
- ↑ Shoulderdoc.co.uk. Available from:https://www.shoulderdoc.co.uk/article/1028 (accessed 10 Nov 2020).

