Sternum: Difference between revisions
Grace Barla (talk | contribs) No edit summary |
Kim Jackson (talk | contribs) (Removed image in the introduction) |
||
| (10 intermediate revisions by 3 users not shown) | |||
| Line 1: | Line 1: | ||
<div class="editorbox"> | <div class="editorbox"> | ||
'''Original Editor''' - [[User:Grace Barla|Grace Barla]] | '''Original Editor''' - [[User:Grace Barla|Grace Barla]] | ||
| Line 5: | Line 4: | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
</div> | </div> | ||
== | == Introduction == | ||
The sternum completes the anterior chest wall as the ventral breastplate. The sternum is a flat cancellous [[bone]] with a compact cortex, it is slightly convex anteriorly, with multiple indentations along its lateral borders (costal notches). <ref name=":2">Radiopedia Sternum Available:https://radiopaedia.org/articles/sternum?lang=gb (accessed 28.9.2022)</ref><ref name=":0">Chaurasia BD. [https://worldofmedicalsaviours.com/bd-chaurasia-human-anatomy-pdf/ Human anatomy]. CBS Publisher; 2004. 8th Edition. Vol.1. Pg 224.</ref><ref>Drake R, Vogl AW, Mitchell AW, Tibbitts R, Richardson P. [https://books.google.co.in/books?hl=en&lr=&id=Di_TDwAAQBAJ&oi=fnd&pg=PP1&dq=Drake+R,+Vogl+AW,+Mitchell+AW,+Tibbitts+R,+Richardson+P.+Gray%27s+Atlas+of+Anatomy+E-Book.+Elsevier+Health+Sciences%3B+2020+Feb+27.&ots=1nOpd5gfYs&sig=0cLBj-amKtlYqTF950sLqnxDexE&redir_esc=y#v=onepage&q&f=false Gray's Atlas of Anatomy E-Book]. Elsevier Health Sciences; 2020 Feb 27.</ref> | |||
The sternum is a flat cancellous bone with a compact cortex, it is slightly convex anteriorly, with multiple indentations along its lateral borders (costal notches). | |||
=== Structure === | === Structure === | ||
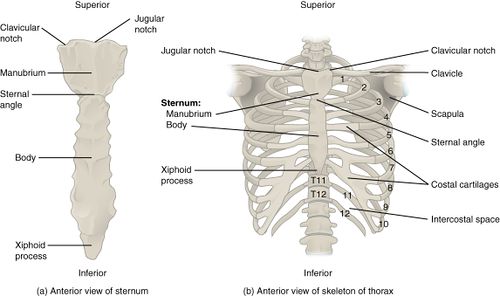
[[File:Parts of sternum.jpg| | [[File:Parts of sternum.jpg|alt=|thumb|Parts of sternum]] | ||
The sternum develops as three distinct parts: | The sternum develops as three distinct parts: | ||
# The manubrium | # The manubrium is flat and four-sided, wider superiorly | ||
# The body is a flat rectangular bone that has facets on its lateral border for articulation with the [[ribs]]. It is: approximately 20 cm long; 3-4 cm wide; 1 cm thick | |||
# The xiphoid process is a thin bony projection inferiorly | |||
# | |||
They articulate via secondary cartilaginous joints via hyaline cartilage with a fibrocartilaginous intervening disc. <ref name=":2" />{{#ev:youtube|kxKoFcfDVYM|600}} | |||
== Function == | == Function == | ||
Changes in the position of the skeletal components of the chest wall cause the changes in the dimensions of the chest. Two very different types of motion of the ribs and sternum create these changes in diameter. | |||
Changes in the position of the skeletal components of the chest wall cause the changes in the dimensions of the chest. Two very different types of motion of the ribs and sternum create these changes in diameter. | |||
# Anteriorly, the ribs are connected to the sternum, which can be viewed as a handle on a mechanical water pump that is activated manually. The manubrium (the ‘‘handle’’) has little motion, so its upward and anterior excursion is relatively limited. The joint between the manubrium and the body of the sternum allows the body and the xiphoid process to have a greater anterior and cephalad excursion, which causes the lower ribs to move more cephalad and anterior than the upper ribs, resulting in a greater increase in diameter in the lower chest. | |||
# The accessory [[Muscles of Respiration|muscles of inspiration]] cause these increases in thoracic diameter, which result in forced inspiration. Conversely, the accessory muscles of expiration cause the sternum to move downward and inward, decreasing these diameters and causing forced expiration<ref name=":1">Graeber GM, Nazim M. [https://www.sciencedirect.com/science/article/abs/pii/S154741270600106X The anatomy of the ribs and the sternum and their relationship to chest wall structure and function]. Thoracic surgery clinics. 2007 Nov 1;17(4):473-89.</ref> | |||
{{#ev:youtube|dxEDGK4nAZM|600}}<ref>Medical Lecture. Learn Movement in respiration,Pump handle & Bucket handle movement. Available from: https://www.youtube.com/watch?v=dxEDGK4nAZM [last accessed 11/28/2021]</ref> | |||
== Articulations == | == Articulations == | ||
The body | # [[File:Rib Cage.jpg|right|frameless|500x300px]] Superiorly the manubrium attaches to the neck where the two deep layers of cervical investing fascia insert | ||
# The manubrium: articulates with the first rib (primary cartilaginous), clavicle (atypical synovial), and body of the sternum (secondary or primary cartilaginous joint). | |||
# The body: articulates with the second rib at the sternomanubrial angle and the 3rd to 7th rib and costal cartilages | |||
# Inferiorly articulates with xiphisternal joint, a secondary cartilaginous joint (symphysis) | |||
# Muscle attachments | |||
[[File:Sternum muscle attachment.png|alt=|thumb|Sternum muscle attachment]] | |||
== Musculotendinous Attachments == | |||
Muscle attachments: [[sternocleidomastoid]], intercostal, [[pectoralis major]], sternohyoid, and sternothyroid muscles | |||
Transversus thoracis muscle arises from the posterior surface of the body | |||
= | The xiphisternum attaches to [[Linea Alba|linea alba]]<ref name=":2" /> | ||
=== Blood and Nerve Supply === | |||
# Arterial supply: nutrient branches from internal thoracic (mammary) artery; deep to the sternum is the internal thoracic artery laterally | |||
# Venous drainage: tributaries of the internal thoracic veins, posterolateral to the sternum | |||
# Nerve supply is via intercostal nerves which arise from the anterior rami of thoracic spinal nerves | |||
== Clinical relevance == | == Clinical relevance == | ||
* The slight movements that take place at the manubriosternal joint are essential for movements of the ribs. | * The slight movements that take place at the manubriosternal joint are essential for movements of the ribs. | ||
* In the anomaly called ‘funnel chest’, the sternum is depressed in another anomaly called | * In the anomaly called ‘funnel chest’, the sternum is depressed in another anomaly called ‘[[Pectus Carinatum (pigeon chest )|pigeon chest]]’, there is forward projection of the sternum like the keel of a boat, and flattening of the chest wall on either side. | ||
* For cardiac surgery, the manubrium and/or body of sternum need to be splitted in midline and the incision is closed with stainless steel wires. | * For cardiac surgery, the manubrium and/or body of sternum need to be splitted in midline and the incision is closed with stainless steel wires. See [[Sternal Precautions]] | ||
* [[Sternal fracture]] are associated with severe blunt trauma to the chest, such as in a vehicular accident. | * [[Sternal fracture]] are associated with severe blunt trauma to the chest, such as in a vehicular accident. | ||
* [[Costochondritis]] is the most common cause of [[Sternal Pain - Different Causes|sternal pain]] and occurs when the cartilage between the sternum and ribs become inflammed and/ or irritated. | * [[Costochondritis]] is the most common cause of [[Sternal Pain - Different Causes|sternal pain]] and occurs when the cartilage between the sternum and ribs become inflammed and/ or irritated. | ||
* [[ | * Sternum pain is pain or discomfort in the area of the chest that contains the sternum and the cartilage connecting it to the ribs. See [[Sternal Pain - Different Causes]] | ||
= References | == References == | ||
<references /> | <references /> | ||
[[Category:Anatomy]] [[Category:Bones]] | [[Category:Anatomy]] [[Category:Bones]] | ||
Latest revision as of 12:23, 29 September 2022
Original Editor - Grace Barla
Top Contributors - Grace Barla, Kim Jackson, Vaibhav Panchal, Lucinda hampton and Vidya Acharya
Introduction[edit | edit source]
The sternum completes the anterior chest wall as the ventral breastplate. The sternum is a flat cancellous bone with a compact cortex, it is slightly convex anteriorly, with multiple indentations along its lateral borders (costal notches). [1][2][3]
Structure[edit | edit source]

The sternum develops as three distinct parts:
- The manubrium is flat and four-sided, wider superiorly
- The body is a flat rectangular bone that has facets on its lateral border for articulation with the ribs. It is: approximately 20 cm long; 3-4 cm wide; 1 cm thick
- The xiphoid process is a thin bony projection inferiorly
They articulate via secondary cartilaginous joints via hyaline cartilage with a fibrocartilaginous intervening disc. [1]
Function[edit | edit source]
Changes in the position of the skeletal components of the chest wall cause the changes in the dimensions of the chest. Two very different types of motion of the ribs and sternum create these changes in diameter.
- Anteriorly, the ribs are connected to the sternum, which can be viewed as a handle on a mechanical water pump that is activated manually. The manubrium (the ‘‘handle’’) has little motion, so its upward and anterior excursion is relatively limited. The joint between the manubrium and the body of the sternum allows the body and the xiphoid process to have a greater anterior and cephalad excursion, which causes the lower ribs to move more cephalad and anterior than the upper ribs, resulting in a greater increase in diameter in the lower chest.
- The accessory muscles of inspiration cause these increases in thoracic diameter, which result in forced inspiration. Conversely, the accessory muscles of expiration cause the sternum to move downward and inward, decreasing these diameters and causing forced expiration[4]
Articulations[edit | edit source]
- Superiorly the manubrium attaches to the neck where the two deep layers of cervical investing fascia insert
- The manubrium: articulates with the first rib (primary cartilaginous), clavicle (atypical synovial), and body of the sternum (secondary or primary cartilaginous joint).
- The body: articulates with the second rib at the sternomanubrial angle and the 3rd to 7th rib and costal cartilages
- Inferiorly articulates with xiphisternal joint, a secondary cartilaginous joint (symphysis)
- Muscle attachments


Musculotendinous Attachments[edit | edit source]
Muscle attachments: sternocleidomastoid, intercostal, pectoralis major, sternohyoid, and sternothyroid muscles
Transversus thoracis muscle arises from the posterior surface of the body
The xiphisternum attaches to linea alba[1]
Blood and Nerve Supply[edit | edit source]
- Arterial supply: nutrient branches from internal thoracic (mammary) artery; deep to the sternum is the internal thoracic artery laterally
- Venous drainage: tributaries of the internal thoracic veins, posterolateral to the sternum
- Nerve supply is via intercostal nerves which arise from the anterior rami of thoracic spinal nerves
Clinical relevance[edit | edit source]
- The slight movements that take place at the manubriosternal joint are essential for movements of the ribs.
- In the anomaly called ‘funnel chest’, the sternum is depressed in another anomaly called ‘pigeon chest’, there is forward projection of the sternum like the keel of a boat, and flattening of the chest wall on either side.
- For cardiac surgery, the manubrium and/or body of sternum need to be splitted in midline and the incision is closed with stainless steel wires. See Sternal Precautions
- Sternal fracture are associated with severe blunt trauma to the chest, such as in a vehicular accident.
- Costochondritis is the most common cause of sternal pain and occurs when the cartilage between the sternum and ribs become inflammed and/ or irritated.
- Sternum pain is pain or discomfort in the area of the chest that contains the sternum and the cartilage connecting it to the ribs. See Sternal Pain - Different Causes
References[edit | edit source]
- ↑ 1.0 1.1 1.2 Radiopedia Sternum Available:https://radiopaedia.org/articles/sternum?lang=gb (accessed 28.9.2022)
- ↑ Chaurasia BD. Human anatomy. CBS Publisher; 2004. 8th Edition. Vol.1. Pg 224.
- ↑ Drake R, Vogl AW, Mitchell AW, Tibbitts R, Richardson P. Gray's Atlas of Anatomy E-Book. Elsevier Health Sciences; 2020 Feb 27.
- ↑ Graeber GM, Nazim M. The anatomy of the ribs and the sternum and their relationship to chest wall structure and function. Thoracic surgery clinics. 2007 Nov 1;17(4):473-89.
- ↑ Medical Lecture. Learn Movement in respiration,Pump handle & Bucket handle movement. Available from: https://www.youtube.com/watch?v=dxEDGK4nAZM [last accessed 11/28/2021]

