Hand Pulleys
Top Contributors - Curtil Louis, Kim Jackson, Vidya Acharya, Lucinda hampton, Admin, Aya Alhindi, Candace Goh, WikiSysop and Aminat Abolade
Definition/Description[edit | edit source]
There are five flexor tendon pulleys in the fingers that are named A1-A5, and consists of annular ligament pulleys, and cruciate pulleys ie The flexor tendon pulley system. The thumb only has two pulleys that are described as A1 and A2.
Flexor pulley system consists of following
- Palmar Aponeurosis Pulley
- 5 Annular Pulleys
- 3 Cruciform Culleys.
Together, these form a fibro-osseous tunnel on the palmar aspect of the hand through which passes the deep and superficial flexor tendons.
Flexor tendon pulley system maintains flexor tendons close to joint’s axis of motion and prevents bowstringing.
NB Finger flexors attachments
- FDP: flexor digitorum profundus (the deeper of the two)
- FDS: flexor digitorum superficialis (the more superficial muscle)
Although the FDP is deep to the FDS over most of its course, it attaches to the skeleton more distally, because it passes through a split in the FDS tendon[1].
Clinically Relevant Anatomy[edit | edit source]
The flexor pulley system (digital sheath) is formed by a

- Retinacular component which condensates and are arranged in cruciform, annular pulleys and transverse patterns.
2. Membranous, or synovial, lining (deep to the above)
The digital sheath serves following functions
- Facilitates smooth gliding of the tendons
- Pulleys from retinacular component provide a mechanical advantage to flexion
- Synovial fluid bathes and provides nutrition.
The flexor tendon system of the hand consists of the flexor muscles of the forearm, their tendinous extensions, and the specialized digital flexor sheaths.
These components work in concert to produce smooth and efficient flexion of the individual digits of the hand.
- Injury to the flexor tendon system can lead to significant morbidity for patients.[2][3]
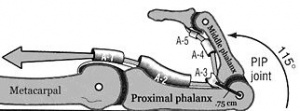
- The most important ones are the A2 and the A4 pulleys[4], situated at the palmar side of the digits. The A2 pulley is continuous with the periosteum of the proximal phalanx and the A4 pulley is in the middle of the middle phalanx.[5]
- Image at R shows the annular and cruciform pulleys on index finger.
Pathology[edit | edit source]

The annular pulleys are functionally important and commonly injured. They comprise a transversely orientated sheath of fibrous tissue that wraps over the flexor superficials and profunda tendons.
There are five flexor tendon pulleys in the fingers (A1-A5.) and two in the thumb (A1 and A2).
- A1, A3 and A5 pulleys [Image at R shows a A3 rupture and associated bowstringing, image below is intact A3].
- overlie the palmar aspect of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints respectively
- attach to the volar plate
- rarely torn
- A2 and A4
- attach to periosteum
- A2 is most load bearing and most frequently torn 2
- A4 is the most flexible
- A4 rupture often seen with A3 rupture[6]

Diagnostic Procedures[edit | edit source]
A fresh pulley injury results in local swelling, tenderness, and pain over the affected area. The main indicator to identify if a total rupture of a pulley has occurred is the appearance of the clinical bowstringing (In this case; when the finger is in flexion, the flexor tendon is taking the shortest line between the top and the base of the finger. Instead of following the phalange).
- Plain radiograph - Have no role in the diagnosis but may be requested in the acute setting of a finger injury. May shows soft tissue swelling.
- Ultrasound - Allows for dynamic testing with flexion stress on the affected digit. It is reported to be up to 100% accurate in identifying pulley injuries
A recent study about the diagnostic procedure of the pulley, was a comparison between the effectiveness of ultrasonography and MRI (Magnetic Resonance Imaging) scanning.
This study showed us that the ultrasonography is a better diagnostic tool than the MRI. Not only because it’s an inexpensive method but also because you can have more precision and a better view with the ultrasonography.[5]
Examination[edit | edit source]
Pulley injuries can be classified according to 3 grades:
- Grade III: Complete rupture of the pulley causing bowstring of the tendon. Symptoms are: locally pain at the pulley, heard a PO or CRACK, swelling, pain when squeezing or climbing, pain during finger extension
- Grade II: Partial rupture of the pulley. Symptoms: locally pain at the pulley, pain while extending the finger and while climbing
- Grade I: Sprain in the finger ligament. Symptoms: Locally pain, pain when squeezing or climbing
Medical Management[edit | edit source]
All A2 and a large proportion of A4 pulley ruptures require surgical repair. A1, A3 and A5 pulleys may be managed conservatively initially.
- Free extrasynovial tendon grafts are the most common method currently in use for pulley reconstruction. The A2 and A4 are recommended to be reconstructed using multiple loops of free extrasynovial tendon grafts in the same place where the original digital pulley was[7]. The strength of the repaired pulley is correlated with the number of loops in the tendon[8].
- Recent studies suggest that intersynovial donor tendons may be more efficient as free extrasynovial tendon graft[9]. The intersynovial grafts had less frictions, what gives a better mobility in the digits.
- Another method is the use of the dorsal wrist retinaculum for the reconstruction of the annular digital pulleys[10]. The advantage of this technique is that the long pulley structure retains the flexor tendon in close proximity to the bone. It is a very efficient technique but has also been shown to be one of the weakest pulley reconstruction methods[11].
Physical Therapy Management[edit | edit source]

Finger Pulley Tear treatment is vital to ensure the full recovery. These injuries can be devastating for eg rock climbers. Around 40% of all reported rock climbing injuries occur at the A2 and A4 pulleys of the flexor tendons. The mechanism of injury is predictable and involves:
- Closed crimp hand position
- Repetitive motion
- Excessive force
- Acute loading[12]
The below is an outline of treatment example
Grade 1: Pulley sprain
A partial tear of a single pulley
No need for immobilization. Begin gentle range-of-motion exercises—bend the finger until it feels tight, hold for 2–3 seconds, relax, and repeat 10 times for several sessions each day. Now perform the same exercise, only straighten the finger. Avoid pushing through pain.
Grade 2: Complete A4 or partial A2, A3 tear/rupture
Either the A4 pulley is completely torn, or A2 and A3 are both partially torn
One to two weeks of immobilization with a finger-immobilization splint or a pulley-protection splint, available online. Gentle range-of-motion exercises. Taping for three months while eg climbing.
Grade 3: Complete A2 or A3 tear/rupture
A2 or A3 pulleys are fully torn
One to two weeks of immobilization with a finger-immobilization splint or a pulley-protection splint, available online. Gentle range-of-motion exercises. Taping for six months.
Grade 4: Annular Pulley Ruptures
Single or multiple ruptures with possible lumbricalis muscle (the muscle between the metacarpal bones) or collateral ligament trauma
Surgical repair is recommended due to the increased risk of fixed flexion contractures, an inability to fully straighten the finger. (Some studies have also recommended surgical repair for grades 2 and 3, especially for elite-level climbers.) Consult with surgeon about rehab options, as they can vary depending on the damage.
- Rohrbough indicates that there remains some disagreement between researchers as to the treatment of pulley tears.[13]. Stretching is recognized as an important promoter of the formation of strong compacted scar tissue[14]. Stretching involves pulling the finger in the varus direction, effectively hyperextending the metacarpophalangeal joint and PIP joint[15]. An alternative therapy such a squeezing a ball may be useful. Such therapy is useful in promoting healing in the injury, it does not prevent atrophy of other healthy tissues.
- Minor A2 pulley injuries or partial tears with no evidence of bowstringing can be treated with either firm circumferential taping for 2 to 3 months to permit healing[16]. The effectiveness of pulley taping was tested and the effect was maximized (10% of bowstringing force) when the tape is positioned near the distal end of the proximal phalanx. The tape absorbed progressively less bowstringing force as the force produced at the fingertip increased[17]; non-stretch, zinc oxide tape of 1.3 cm width was used[16]. This result has two implications. Firstly, taping is likely to be most effective during the earlier stages of rehabilitation when the forces produced by the fingers are lower. Secondly, taping is unlikely to prevent pulley injuries, as these are likely to occur when forces on the pulley are maximal[18].
Key Research[edit | edit source]
- Digital Flexor Sheath: Repair and Reconstruction of the Annular Pulleys and Membranous Sheath
- Analysis of the gliding pattern of the canine flexor digitorum profundus tendon through the A2 pulley, Shigeharu Uchiyama1, Peter C. Amadio, Lawrence J. Berglund, Kai-Nan An Biomechanics Laboratory, Division of Orthopedic Research, Mayo Clinic, 200 First Street S.W., Rochester, MN 55905, USA Accepted 15 January 2008
- Zone II Combined Flexor Digitorum Superficialis and Flexor Digitorum Profundus Repair Distal to the A2 Pulley Jeffrey M. Pike, MD, Richard H. Gelberman, MD
Resources[edit | edit source]
Bron 1: http://www.orthobullets.com/hand/6004/flexor-pulley-system
Bron 2: http://edgar.brand.edgar-online.com/EFX_dll/EDGARpro.dll?FetchFilingHTML1?ID=5479903&SessionID=cg7xWq-zAf69x47
References[edit | edit source]
- ↑ Biomechanics of the hand Gwenda Sharp OTR and Dave Thompson PT Available from:https://ouhsc.edu/bserdac/dthompso/web/namics/hand.htm (last accessed 18.3.2020)
- ↑ Kaplan EB. Functional and Surgical Anatomy of the Hand. Philadelphia, JB Lippincott Co, 2nd Ed, 1965
- ↑ Bone spine Pulley system of hand Available from:https://boneandspine.com/flexor-tendon-pulley-system-of-hand/ (last accessed 17.3.2020)
- ↑ Lin GT, Amadic PC, An KN, et al. Functional anatomy of the human digital flexor pulley system. J Hand Surg Am 14:949-956, 1989
- ↑ 5.0 5.1 Martinoli, C., Bianchi, S., Nebolio, M., Derchi, L. E., Garcia, J. F. (2000) Sonographic evaluation of digital annular pulley tears. Skeletal Radiol. 29. 387-391
- ↑ Radiopedia Finger pulley Injury Available from:https://radiopaedia.org/articles/finger-pulley-injury (last accessed 17.3.2020)
- ↑ Bunnell S. Repair of tendons in the fingers and descriptions of two new instruments. Surg Gynecol Obstet 26:103-110, 1918
- ↑ Widstrom CJ, Doyle JR, Johnson G. A mechanical study of the effectiveness of 6 digital pulley reconstruction techniques. Part 2. Strength of individual reconstructions. J Hand Surg Am 4:826-829,1989
- ↑ Nishida J, Amadio PC, Bettinger PC, et al. Excursion properties of tendon graft sources. interaction between tendon and A2 pulley. J Hand Surg Am 23:274-278, 1998
- ↑ Lister GD. Reconstruction of pulleys employing extensor retinaculum. J Hand Surg Am 4:461-464, 1979
- ↑ Kleinert HE, Bennett JB. Digital pulley reconstruction employing the always present rim of the other previous pulley. J Hand Surg Am 3:297-298, 1978
- ↑ Anytime physio Finger pulley injury Available from:https://anytimephysio.com.au/finger-pulley-tear-treatment/ (last accessed 17.3.2020)
- ↑ Rohrbough, J. T., Mudge, M. K., Schilling, R. C. (2000) Overuse injuries in the elite rock climber. Med. Sci Sports Exerc. 32(8): 1369-1372
- ↑ R. S., Raya, M. A. (2001) Manual Modalities. in: Gonzalez, E. G., Myers, S. J., Edelstein, J. E., Lieberman, J. S., Downey, J. A. Physiological basis of rehabilitation medicine. 3rd ed. Butterworth Heinemann
- ↑ Gresham, N. (1996) High performance: warming up. High. 166: 14-15
- ↑ 16.0 16.1 Hand Injuries in Rock Climbing. Reaching the Right Treatment Peter J. L. Jebson, MD; Curtis M. Steyers, MD The Physician and Sportsmedicine – Vol 25: No5, May 1997
- ↑ Schweizer, A. (2000) Biomechanical effectiveness of taping the A2 pulley in rock climbers. J. Hand Surg. 25B. 102-107
- ↑ Warme, W. J., Brooks, D. (2000) The Effect of circumferential taping on flexor tendon pulley failure in rock climbers. Am. J. Sports Med. 28(5): 674-678


{kind=link}