Burn Wound Injury Dressing Selection: Difference between revisions
No edit summary |
No edit summary |
||
| Line 44: | Line 44: | ||
* Provide topical antimicrobial protection | * Provide topical antimicrobial protection | ||
* Minimise contamination from the external environment | * Minimise contamination from the external environment | ||
* Decrease | * Decrease oedema | ||
* Protect the wound | * Protect the wound | ||
* Be careprovider friendly (ie. easy to apply and/or remove) | * Be careprovider friendly (ie. easy to apply and/or remove) | ||
Revision as of 04:35, 9 April 2024
Top Contributors - Stacy Schiurring and Jess Bell
Burn Wound Injury Standard of Care[edit | edit source]
Please see this document for a growing list of wound care terminology and definitions.
For a review of other steps in burn wound care, please see the following articles:
- Burn wound injury assessment
- Assessment of infection in burn wounds
- Burn wound injury cleansing techniques and solutions
- Burn wound injury non-surgical debridement
Current Standard of Care[edit | edit source]
The current standard of care for large and deep burn wounds is (1) early surgical excision and (2) wound closure[1]
- wound closure can be achieved by skin grafting or temporary biological coverage for deep partial and full thickness burns
Alternatives to Early Excision and Wound Closure[edit | edit source]
- Surgical debridement followed by wound cleansing and regular dressing changes
- preferred option for burns of indeterminate depth until burn depth determined
- can be the most appropriate option to allow healing of partial thickness burn size. This will allow for a smaller area of the burn wound will need a skin graft.
- Local wound cleansing and dressing changes
- Indicated when surgery is not feasible or after debridement without grafting or temporary closure
- Common for smaller burn areas, including full thickness burns
- Standard for most superficial partial thickness burns
Exceptions to Standards of Care[edit | edit source]
- Surgery not feasible due to patient status, or resource availability
- Grafting or skin substitutes not appropriate due to (1) contaminated wounds, (2) native skin is too damaged or of too small an area to provide a skin graft, or (3) skin substitutes are not available.
Burn wounds which (1) do not undergo surgical debridement, or that (2) underwent surgical debridement without application of a skin graft or temporary covered with a skin substitute will require ongoing dressing changes throughout the course of healing.[1]
Role of Wound Dressings[edit | edit source]
In all cases when burn wounds are not grafted immediately, routine burn wound care and dressing changes are needed. The determination of dressings and frequency of interventions is based on a variety of factors to be described below. [1]
Effective burn wound dressings provide the following:[1][2]
- Absorb and manage drainage
- Minimise risk of burn wound conversion
- Maintain a moist wound environment
- Minimise peri-wound maceration
- Prevent excessive evaporation from wound surface that can (1) cause the wound to become desiccated and (2) result in hypothermia
- Provide topical antimicrobial protection
- Minimise contamination from the external environment
- Decrease oedema
- Protect the wound
- Be careprovider friendly (ie. easy to apply and/or remove)
- Reduce pain during (1) removal and application of the dressings and (2) during functional activities
- Allow movement and function
Clinical Pearl: Benefits of Moist Wound Healing[edit | edit source]
Multiple studies have demonstrated that application of moist wound dressings immediately after injury minimises the risk of burn wound conversion. The positive effects of a moist wound environment on wound healing include:[1]
- increases keratin migration and re-epithelialization
- increases collagen synthesis
- increases autolytic debridement
- decreases necrosis
- decreases pain
- decreases inflammation
- decreases scarring
- facilitates cell-to-cell signaling
- provides means of delivering topical treatment
- improves wound aesthetics after healing
Determining Dressing Care Plan[edit | edit source]
Determining Dressing Change Frequency[edit | edit source]
Based on burn wound or patient status, and on type of dressing:[1]
- Status of burn wound (or patient) – daily or more than planned if:
- Dressing used is not antimicrobial, or agent has short-acting antimicrobial properties
- Verified or suspected infection
- Monitor for conversion
- Significant areas of undebrided eschar
- Drainage not contained by dressing
- Any other concerns
- Need to balance concern for wound and desire to leave wound undisturbed and not introduce risk for additional contamination
- Minimize risk of damage to healing tissue
- Type of dressing or topical agent
- Ability of dressing to maintain a moist environment
Determining Dressing and Topical Agent[edit | edit source]
- Depth and stage of healing of burn wound
- Indications of infection
- Amount of wound drainage
- Clinical assessment of progress, or lack of progress, in wound healing
- Ease of dressing application and removal
- Availability of dressings and topical agents
- Cost of topical agents and dressings
- Dressings change as wound progresses (or doesn’t progress)
Burn Wound Dressing Options[edit | edit source]
This section includes a summary of gauze and gauze-like dressings, and possible solutions, creams, and ointments that can be used in the treatment of burn wound injuries. Please see this article for more information on advanced dressings for burn care.
| Benefits | Risks | |
|---|---|---|
| Saline |
|
|
| Mafenide Acetate |
|
|
| Sodium Hypochlorite[3] | broad spectrum |
|
| Hypochlorous acid |
|
|
| Povidone-Iodine[3] | broad-spectrum | cytotoxic at full strength |
| Acetic acidvarious reports of strengths, 0.25% up to 5% |
|
| Benefits | Risks | Burn-specific Considerations | |
|---|---|---|---|
| Silver sulfadiazine[4][5] |
|
Contra-indications:
|
Full and deep-partial thickness burns:
|
| Mafenide acetate [5](sulfamyalon) |
|
|
|
| Antibiotic ointments |
|
Change the antibiotic used or discontinue with clinical assessment which finds:
|
Recommended primarily for superficial partial thickness burn wounds |
| Medical Grade honey[6] |
|
Minimal evidence for use with burn wounds, however research shows positive outcomes on superficial partial thickness burns | |
| Cadexomer Iodine[7] | Most effective against MSSA and MRSA |
| Benefits | Risks | Burn-specific Considerations | |
|---|---|---|---|
| Polyhexamethylene biguanide[3] (PHMB)-impregnated dressing |
|
Recommended for superficial partial thickness burn wounds | |
| Bismuth
(eg. Xeroform gauze) |
|
Contraindicated with allergy to Bismuth |
Burn Wound Injury Areas of Special Concern[edit | edit source]
Guidelines for Blister Management[edit | edit source]
"In all of the literature that I've looked at over the past couple of decades, [blister management] hasn't changed. The approach to managing blisters is kind of a 50-50 split between that side of the issue that thinks that all blisters should be unroofed and debrided immediately and completely, and the side that thinks you should leave blisters alone and allow things to happen naturally." -Diane Merwarth, Physical Therapist, Wound Care Specialist
Blisters should be deroofed (unroofed) in the following situations:[1]
- During surgical cleansing and debridement
- When the blister itself is disrupted
- Now a portal for entry of microbes
- Risk of microbes trapped under loose skin
- When appearance is questionable
- Thick, cloudy or opaque fluid
- Bloody or discolored
Blisters should be left intact in the following situations:[1]
- If blisters are small and not disrupted
- When not affecting function
Blisters shoulder drained but NOT deroofed in the following situations:[1]
- Large taut blisters with clear fluid
- Blisters continuing to increase in size
- Blisters are preventing function
Deroofing is the process whereby the 'roof' of the blister is removed under clean (aseptic) conditions to expose the viable tissue beneath. [8]
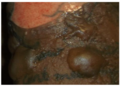
Intact blisters

Left image: intact blister. Middle image: deroofed blister. Right image: re- epithelialization in wound bed.
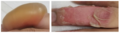
Left image: blister intact. Right image: deroofed blister

All photos provided by and used with kind permission from Diane Merwarth, PT
Resources[edit | edit source]
Clinical Resources:[edit | edit source]
- Wound Antiseptics and European Guidelines for Antiseptic Application in Wound Treatment
- American Burn Association Guidelines for Burn Care Under Austere Conditions
Optional Additional Reading:[edit | edit source]
- Allorto NL. Primary management of burn injuries: Balancing best practice with pragmatism. South African Family Practice. 2020 Jan 1;62(1):1-4.
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Merwarth, D. Management of Burn Wounds Programme. Introduction to Dressing Selection for Burn Wound Injuries. Physioplus. 2024.
- ↑ Legrand M, Barraud D, Constant I, Devauchelle P, Donat N, Fontaine M, Goffinet L, Hoffmann C, Jeanne M, Jonqueres J, Leclerc T. Management of severe thermal burns in the acute phase in adults and children. Anaesthesia Critical Care & Pain Medicine. 2020 Apr 1;39(2):253-67.
- ↑ 3.0 3.1 3.2 Babalska ZŁ, Korbecka-Paczkowska M, Karpiński TM. Wound antiseptics and European guidelines for antiseptic application in wound treatment. Pharmaceuticals. 2021 Dec 2;14(12):1253.
- ↑ Oaks RJ, Cindass R. Silver sulfadiazine. StatPearls, 2022; NCBI Bookshelf (a service of the National Library of Medicine, NIH. © 2022, StatPearls LLC. Bookshelf ID: NBK556054PMID: 32310514
- ↑ 5.0 5.1 PATEL R, DESAI R, PATEL A, SHAH S, PRAJAPATI B, PATEL V, ALEXANDER A. Burn assessment: A critical review on care, advances in burn healing and pre-clinical animal studies. Journal of Research in Pharmacy. 2023 Jul 1;27(4).
- ↑ Tashkandi H. Honey in wound healing: An updated review. Open life sciences. 2021 Oct 6;16(1):1091-100.
- ↑ Stuermer EK, Plattfaut I, Dietrich M, Brill F, Kampe A, Wiencke V, Ulatowski A, Geffken M, Rembe JD, Naumova EA, Debus SE. In vitro activity of antimicrobial wound dressings on P. aeruginosa wound biofilm. Frontiers in Microbiology. 2021 May 14;12:664030.
- ↑ North Bristol NHS Trust. The de-roofing of burns blisters. Available from: https://www.mysurgerywebsite.co.uk/website/SWUK001/files/The%20De-roofing%20of%20Burns%20Blisters_NBT002996.pdf (accessed 2 April 2024).

