General Principles of Exercise Rehabilitation: Difference between revisions
No edit summary |
No edit summary |
||
| Line 164: | Line 164: | ||
* Transfer/ Autonomous stage: the ability to carry out a task without paying attention to tactics. Ideally, we want to deliver our patients to this stage where they can perform a similar, but different task than originally learned in the acquisition stage. | * Transfer/ Autonomous stage: the ability to carry out a task without paying attention to tactics. Ideally, we want to deliver our patients to this stage where they can perform a similar, but different task than originally learned in the acquisition stage. | ||
{{#ev:youtube|OHGE68ZS8g4}}<ref>Three stages of learning movement. Available from: https://www.youtube.com/watch?v=OHGE68ZS8g4</ref> | {{#ev:youtube|OHGE68ZS8g4}}<ref>Three stages of learning movement. Available from: https://www.youtube.com/watch?v=OHGE68ZS8g4</ref> | ||
| Line 170: | Line 171: | ||
Feedback during motor learning<ref name=":1" /> | Feedback during motor learning<ref name=":1" /> | ||
* Feedback can be either intrinsic or extrinsic. Intrinsic feedback - seen as the knowledge of performance but in can be limiting to learning when in extreme. Extrinsic (augmented) feedback can be from visual demonstrations, using a mirror, verbal instructions or guidance through touching. | * Feedback can be either intrinsic or extrinsic. | ||
* | ** Intrinsic feedback - seen as the knowledge of performance but in can be limiting to learning when in extreme. | ||
* | ** Extrinsic (augmented) feedback can be from visual demonstrations, using a mirror, verbal instructions or guidance through touching. | ||
* Feedback can also | ** Provide specific and constructive feedback | ||
* Timing feedback is | ** Feedback is informational, but can also have motivational properties<ref name=":3">Cools AM, Maenhout AG, Vanderstukken F, Declève P, Johansson FR, Borms D. The challenge of the sporting shoulder: From injury prevention through sport-specific rehabilitation toward return to play. Annals of Physical and Rehabilitation Medicine. 2021 Jul 1;64(4):101384.</ref> | ||
* Constant feedback | ** Timing of feedback is important | ||
* | *** Constant feedback won't allow for the athlete to reflect and learn | ||
*** "Less is more" - occasional feedback on positive performance is better than constant feedback on every task attempt<ref name=":3" /> | |||
The rehabilitation then should develop complexity to mimic the reality of | The rehabilitation then should develop complexity to mimic the reality of the athlete's performance requirements. | ||
Random | Random skill training can be acquired in this stage, by training the athlete to deliver function on various surfaces, with different external loads and to react to external stimuli.<ref name=":1" /> | ||
* | * | ||
Revision as of 12:00, 5 August 2022
Original Editor - Wanda van Niekerk based on the course by Lee Herrington
Top Contributors - Wanda van Niekerk, Kim Jackson and Jess Bell
Introduction[edit | edit source]

For clinicians to design an effective rehabilitation programme, they need to understand what the specific performance needs of the athlete are. What are the athlete's goals, but also what is their current status? Identifying an athlete's current status will also identify the athlete's current constraints, and most often these constraints are around tissue injury. Implementation of the rehabilitation programme can only start if these factors are in place. The rehabilitation plan consists of a loading plan with a clear set of intervention intents. This results in adaptations that lead the athlete from their current status to their performance goals. An important consideration is monitoring and reviewing the interventions and also monitoring against the intended outcome.[1]
Performance Backward Thinking[edit | edit source]
- Performing a performance needs analysis with the athlete[2]
- What is the athlete's performance goal or end goal?
- What is required to reach this goal?
- What physical qualities underpin these?
- What are the current capabilities?
- What are the barriers and facilitators?
Components of a Performance Needs Analysis[edit | edit source]
Consider the following in an activity-specific needs analysis[2]:
| Components of Activity Specific Performance Needs Analysis[2] |
|---|
|
A Paradigm for Needs Analysis and Rehabilitation[edit | edit source]
- Performance requirements can include level of strength, level of mobility, level of endurance, coordination tasks
- With an injury, the current status of the injured tissue as well as the athlete’s holistic status needs to be assessed.
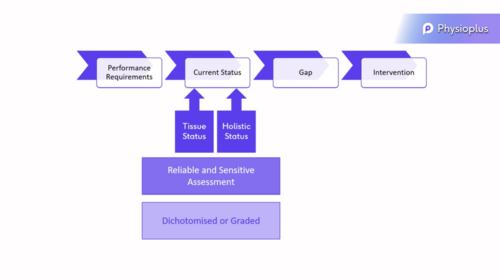 Needs Analysis Paradigm[1]
Needs Analysis Paradigm[1]- Reliable and sensitive assessments are necessary to assess the current tissue status
- What can the injured tissue tolerate at this moment in time?
- What can the individual do in relation to the injured tissue at this current time with injury?
- Consider dichotomised versus graded assessment approaches
- Dichotomised assessment:
- "Specific structure is painful, therefor it is injured"
- Simple test with a yes or no answer or yes the structure is injured or no, the structure is not injured.
- Graded assessment
- Graded exposure of the tissue to load to see how much load the injured tissue can tolerate.
- Dichotomised assessment:
- The assumption is often that an acute muscle/ligament/tendon injury will have zero load tolerance when the structure is injured, but often these injured structures can still tolerate a level of load even if it is very little.
- The level of load an injured tissue can tolerate needs to be clearly identified[1]
- Note that significant muscle atrophy can occur within 5 -14 days of inactivity.[3] It is, therefore, crucial to determine the minimum activity an injured athlete can perform to reduce the occurrence of atrophy due to underactivity.
- The level of load an injured tissue can tolerate needs to be clearly identified[1]
- Reliable and sensitive assessments are necessary to assess the current tissue status

Principles of Rehabilitation[edit | edit source]
Where to Start?[edit | edit source]
- Identify the start point
- Establish a stable baseline
- Once the gaps have been identified and a starting point for loading has been identified, that can be seen as the establishment of a stable baseline. The starting point is not always at zero (i.e. no strength or no flexibility) and therefor a graded approach in assessing the tissue tolerance level is key.
- Consider the load deformation curve
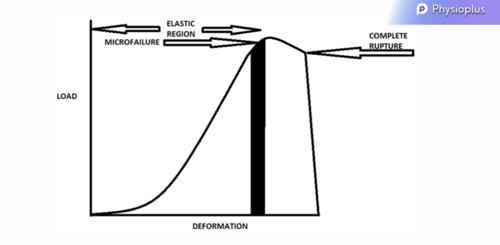 Load Deformation Curve[2]
Load Deformation Curve[2]- refresh your memory here: Is load a bad thing?
- A certain amount of micro failure is allowed when loading the tissue as this brings on physiological changes, which leads to tissue adaptation, and this strengthens the tissue.
- If we consider the load-deformation curve and sub-optimally load tissue (loading on the left side to the micro failure zone), this will lead to tissue atrophy and the tissue will weaken to the level of the loads applied.
- Similarly, if the tissue is overloaded (loading to the right side of the micro failure zone), this can lead to irreparable damage
- Therefore, it is imperative to apply the maximum load the specific tissue can tolerate.

Underpinning Theories[edit | edit source]
- Mechanotransduction = shifting of mechanical energy into physiological energy.
- Read more here: Mechanotransduction Hypothesis
- Physical Stress Theory[4]
- biological tissues adapt to changes in the levels of applied stress
- maintaining tissue tolerance is essential to prevent atrophy, whereas overloading results in hypertrophy
- excessively high levels of stress lead to tissue injury and potential permanent damage
- the magnitude, time, and direction of stress application determine the overall level of exposure to physical stress
- injury may occur due to a high-magnitude stress applied for a brief period, a low-magnitude stress applied for a long duration, and/or a moderate-magnitude stress applied to the tissue many times
- Principle of Specificity = the body adapts to the loads which are applied to it
- Read more here: The Basic Principles in Exercise Physiology
- Tissue requires loads in specific ways
- Bone[5]
- Tendon[6]
- stretch-shortening or plyometric tasks to transfer energy
- isometric forces - transfer force across a joint to generate joint movement
- Read more: Tendon Load and Capacity
- Muscle[7]
- responds to the nature of the load
- responds to the range that load is applied in
- specific velocities of muscle contraction (Olympic sprinter vs Older person walking to the shops)

Key Issues when Reloading Injured Tissues[edit | edit source]
- Key issues to remember when reloading injured tissues[1]
- Understand what the stable baseline load is and at what level loading should start at
- What forces stress the injured structure?
- Which forces and loads do not stress the injured structure?
- Ligaments - direction and magnitude of injurious force need to be defined
- Muscle and tendon - nature of contraction load, force velocity and length-tension relationship implications should be defined
- Articular surface - define the direction and magnitude of injurious forces and the impact of malalignment
Monitoring Impact of Load[edit | edit source]
It is important to know when to proceed with gradual stress and when to take a step back. There are multiple indicators of excess or less load: [2]
- Increased swelling of the training muscles indicates inflammation-overload.
- Circumferential measures: to be taken after the activity, in the morning and in the evening.
- Ideally swelling should not increase between days. If it was increased after training it should decrease by the evening, if it is still swollen by the next morning then the training load should be decreased.
- Pain
- Visual Analogue Scale (VAS) 0-10, rate the score to a specific movement or exercise.
- Any change in score the day after training >1 that does not reduce by the evening may indicate overload.
- Stiffness: especially in the morning, is a good mark of inflammation.
- Link the stiffness to a specific task or movement for e.g. simply ask the patient if they find difficulties doing a simple full squat in the morning.
- Muscle contractility or inhibition is influenced by pain and swelling.
- Monitor muscle contraction force.[1]
- Global loads[8]
- Technological applications and trackers could be helpful in giving a start point to build up a gradual progressive rehabilitation program without overloading or deloading.
Progressing Load[edit | edit source]
- Progressively expose to load at tissue and system level[9]
- Maximum tolerated loads necessary to generate supraphysiological stress and low level of micro failure to create adaptation[1]
- Allow for sufficient recovery time to allow for adaptation
- Application of the appropriate load to drive the required adaptation
- Specific Adaptation to Imposed Demand (SAID) principle
- Adaptations produced by the training are highly specific to the nature of the stimulus or overload applied[7]
- SAID applies to all the systems of the body
- The adaptations are specific to strength, power, endurance, functional activity, joint angle, sequence of muscle activations, energy systems and virtually all other variables present
- Specific Adaptation to Imposed Demand (SAID) principle
Key Rehabilitation Areas[edit | edit source]
Regaining Maximum Force and Force Generation[edit | edit source]
- Maximum force
- Overcome muscle inhibition
- muscle stimulation at the same time as contracting the muscle to superimpose the contraction[10]
- use crosstalk or effort from the other limb to generate neural activity in injured limb
- whole body or local vibration
- relieve pain
- work in mid-range initially to generate strongest contraction
- Repetition maximums
- The repetition continuum or strength-endurance continuum is usually used to prescribe specific loading recommendations.[7]
- Muscle strength - low repetitions with heavy loads: 1 - 5 repetitions per set with 80% - 100% of 1 -repetition max (1RM)
- Muscle hypertrophy – moderate repetitions with moderate loads: 8 - 12 repetitions per set with 60% - 80% of 1RM
- Muscle endurance – high repetitions with light loads: 15 + repetitions per set with loads below 60% of 1RM
- Read more: Loading Recommendations for Muscle Strength, Hypertrophy, and Local Endurance: A Re-Examination of the Repetition Continuum[7]
- Overcome muscle inhibition
- Force generation
- Force velocity - slow contraction vs rapid generation of force
Regaining Movement Skill[edit | edit source]
Teaching the movement involves various levels of learning[2][11]:
- Acquisition/Cognitive stage: deconstructing the function onto simple movements with repetitions.
- Retention/Associative stage: recalling and delivering the task after a period of not practicing the task.
- Transfer/ Autonomous stage: the ability to carry out a task without paying attention to tactics. Ideally, we want to deliver our patients to this stage where they can perform a similar, but different task than originally learned in the acquisition stage.
Instructing patients depends on the stage of learning. In the first stage, closed skill is used to eliminate all external influences and drives the focus internally (Intrinsic focused cues) by asking patient to reflect on the purpose and the mechanism of a simple movement e.g. single leg squat. Repetitions in this stage aids cognition and acquisition. In Retention and Transfer stages, training should be external or goal focused. For example, asking patient to move towards a certain target, or doing a task while keeping trunk ahead of knees. The ultimate aim of motor skill learning is to transfer the skill to performance in sport or activities of daily living. The patient needs to move from closed skill tasks (same movement tasks in stable predictable environments) to open skill where tasks/movements are unplanned.
Feedback during motor learning[2]
- Feedback can be either intrinsic or extrinsic.
- Intrinsic feedback - seen as the knowledge of performance but in can be limiting to learning when in extreme.
- Extrinsic (augmented) feedback can be from visual demonstrations, using a mirror, verbal instructions or guidance through touching.
- Provide specific and constructive feedback
- Feedback is informational, but can also have motivational properties[13]
- Timing of feedback is important
- Constant feedback won't allow for the athlete to reflect and learn
- "Less is more" - occasional feedback on positive performance is better than constant feedback on every task attempt[13]
The rehabilitation then should develop complexity to mimic the reality of the athlete's performance requirements.
Random skill training can be acquired in this stage, by training the athlete to deliver function on various surfaces, with different external loads and to react to external stimuli.[2]
Key Take Home Messages[edit | edit source]
- Understand the performance requirements
- Identify what load the tissue (and individual) can currently tolerate
- Fill the gap in the performance deficits
- Clearly define the purpose of an exercise
- Measure the exercise's impact against that purpose
- Always apply the maximum loads the tissue (and individual) can tolerate
- Assess the impact of loading at all stages
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 Herrington, L. General Principles of Exercise Rehabilitation Course. Physioplus. 2022.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 Herrington, L, Spencer, S. Principles of Exercise Rehabilitation. In Petty NJ, Barnard K, editors. Principles of musculoskeletal treatment and management e-book: a handbook for therapists. Elsevier Health Sciences; 2017 Jun 28.
- ↑ Wall BT, Dirks ML, Van Loon LJ. Skeletal muscle atrophy during short-term disuse: implications for age-related sarcopenia. Ageing research reviews. 2013 Sep 1;12(4):898-906.
- ↑ Mueller MJ, Maluf KS. Tissue adaptation to physical stress: a proposed “Physical Stress Theory” to guide physical therapist practice, education, and research. Physical therapy. 2002 Apr 1;82(4):383-403.
- ↑ Mellon SJ, Tanner KE. Bone and its adaptation to mechanical loading: a review. International Materials Reviews. 2012 Sep 1;57(5):235-55.
- ↑ Docking SI, Cook J. How do tendons adapt? Going beyond tissue responses to understand positive adaptation and pathology development: A narrative review. Journal of musculoskeletal & neuronal interactions. 2019;19(3):300.
- ↑ 7.0 7.1 7.2 7.3 Schoenfeld BJ, Grgic J, Van Every DW, Plotkin DL. Loading recommendations for muscle strength, hypertrophy, and local endurance: a re-examination of the repetition continuum. Sports. 2021 Feb 22;9(2):32.
- ↑ Draovitch P, Patel S, Marrone W, Grundstein MJ, Grant R, Virgile A, Myslinski T, Bedi A, Bradley JP, Williams III RJ, Kelly B. The Return-to-Sport Clearance Continuum Is a Novel Approach Toward Return to Sport and Performance for the Professional Athlete. Arthroscopy, sports medicine, and rehabilitation. 2022 Jan 1;4(1):e93-101.
- ↑ Taberner M, Allen T, Cohen DD. Progressing rehabilitation after injury: consider the ‘control-chaos continuum’. British journal of sports medicine. 2019 Sep 1;53(18):1132-6.
- ↑ Blazevich AJ, Collins DF, Millet GY, Vaz MA, Maffiuletti NA. Enhancing adaptations to neuromuscular electrical stimulation training interventions. Exercise and sport sciences reviews. 2021 Oct;49(4):244.
- ↑ Charlton JM, Eng JJ, Li LC, Hunt MA. Learning Gait Modifications for Musculoskeletal Rehabilitation: Applying Motor Learning Principles to Improve Research and Clinical Implementation. Physical Therapy. 2021 Feb;101(2):pzaa207.
- ↑ Three stages of learning movement. Available from: https://www.youtube.com/watch?v=OHGE68ZS8g4
- ↑ 13.0 13.1 Cools AM, Maenhout AG, Vanderstukken F, Declève P, Johansson FR, Borms D. The challenge of the sporting shoulder: From injury prevention through sport-specific rehabilitation toward return to play. Annals of Physical and Rehabilitation Medicine. 2021 Jul 1;64(4):101384.

