Brachial Plexus Injury: Difference between revisions
m (removed a video as it was unavailable on you-tube) |
Kapil Narale (talk | contribs) No edit summary |
||
| (29 intermediate revisions by 4 users not shown) | |||
| Line 1: | Line 1: | ||
<div class="editorbox"> | <div class="editorbox">'''Original Editor '''[[User:Aarti Sareen|Aarti Sareen]] | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
</div> | </div> | ||
== Introduction == | == Introduction == | ||
Brachial | Brachial Plexus (BP) injuries range in severity and cause. The effects may be mild or severe. Unfortunately traumatic incidences of BP injuries are on the rise, often leading to severe social and financial hardships, and greatly affecting quality of life ([[Quality-Adjusted Life Year|QOL]]). This page outlines the main issues arising from BP injuries and the rationale behind their management.<ref name=":2" /> | ||
''Historical note : Homer (approx. 800 BC) depicted a battle in The Illiad which involved Hector striking Teucer over the clavicle with a rock and preventing him from wielding his bow.<ref>Luo TD, Li Z. Brachial Plexus Injuries. [Updated 2018 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482305/ (last accessed 13.3.2019)</ref>'' | ''Historical note : Homer (approx. 800 BC) depicted a battle in The Illiad which involved Hector striking Teucer over the clavicle with a rock and preventing him from wielding his bow.<ref>Luo TD, Li Z. Brachial Plexus Injuries. [Updated 2018 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482305/ (last accessed 13.3.2019)</ref>'' | ||
| Line 11: | Line 11: | ||
== Function == | == Function == | ||
[[Brachial | [[Brachial Plexus|Brachial plexus]] is the network of nerves which runs through the cervical spine, neck, axilla and then into arm or it is a network of nerves passing through the cervico axillary canal to reach the axilla, and innervates the brachium (upper arm), antebrachium (forearm) and the hand. It is a somatic nerve plexus formed by intercommunications among the ventral rami (roots) of the lower 4 cervical nerves (C5-C8) and the first thoracic nerve (T1).<br>The brachial plexus is responsible for cutaneous and muscular innervation of the entire upper limb, with two exceptions: the trapezius muscle innervated by the spinal accessory nerve (CN XI) and an area of skin near the axilla innervated by the intercostobrachial nerve. <br> | ||
== Clinical Anatomy == | == Clinical Anatomy == | ||
| Line 18: | Line 18: | ||
==== Roots ==== | ==== Roots ==== | ||
These | These consist of the anterior primary rami of spinal nerves C5 - C8 and T1 with contributions from the anterior primary rami of C4 and T2. The origin of the plexus may shift one segment either upward or downward resulting in a pre-fixed plexus or post-fixed plexus respectively. In a prefixed plexus, the contribution by C4 is large, and in that form T2 is often absent. In a post-fixed plexus, the contribution by T1 is large, T2 is always present, C4 is absent, and C5 is reduced in size.<ref name="BD">B.D Chaurasia.Human Anatomy.Vol.1.Fourth Edition.</ref> The roots join to form trunks as follows: | ||
[[Image:Brachial-plexus-2.png|500x500px]] | == [[Image:Brachial-plexus-2.png|500x500px]] Trunks == | ||
* Upper trunk is formed by C5 & C6 | * Upper trunk is formed by C5 & C6 | ||
* Middle trunk is formed by C7 | * Middle trunk is formed by C7 | ||
| Line 38: | Line 34: | ||
==== Branches ==== | ==== Branches ==== | ||
The specific branches of each cord can be seen | The specific branches of each cord can be seen on [http://www.physio-pedia.com/Brachial_plexus this page] | ||
== Mechanism of injury == | == Mechanism of injury == | ||
Injury to brachial plexus can occur in many ways. These include | Injury to brachial plexus can occur in many ways. These include, contact sports, motor vehicle accidents, or during birth. Grossly, it can be divided into: | ||
* Traumatic e.g motor vehicle accident, contact sports | * Traumatic, e.g motor vehicle accident, contact sports | ||
* Non traumatic e.g.obstetric palsy and [http://www.physio-pedia.com/Parsonage-Turner_Syndrome Parsonage-Turner Syndrome]<br> | * Non traumatic, e.g. obstetric palsy and [http://www.physio-pedia.com/Parsonage-Turner_Syndrome Parsonage-Turner Syndrome]<br> | ||
The network of nerves is fragile and can be damaged by stretching, pressure or cutting. | The network of nerves is fragile and can be damaged by stretching, pressure, or cutting. | ||
* Stretching can occur when the head and neck are forced away from the shoulder, | * Stretching can occur when the head and neck are forced away from the shoulder, which could happen in a fall from a motorcycle. If severe enough, the nerves can actually avulse, or tear out of their roots in the neck. | ||
* Pressure could occur from crushing of the brachial plexus between the collarbone and first rib, or swelling in this area from injured muscles or other structures<ref>American Society of Surgery of Hand. Available from www.assh.org/Public/HandConditions/Documents/Web_Version_PDF/BrachPlex.pdf</ref>. The former examples of events are caused by one of two mechanisms | * Pressure could occur from crushing of the brachial plexus between the collarbone and first rib, or swelling in this area from injured muscles or other structures <ref>American Society of Surgery of Hand. Available from www.assh.org/Public/HandConditions/Documents/Web_Version_PDF/BrachPlex.pdf</ref>. The former examples of events are caused by one of two mechanisms that remain constant during the injury. <ref>Midha, Rajiv, MD. "Neurosurgery." Epidemiology of Brachial Plexus Injuries in a Multitrauma Po... :. Congress of Neurological Surgeons, June 1997. Web. 29 Jan. 2013.</ref> The two mechanisms that can occur are 'traction' and 'heavy impact' <ref>Narakas, A.O. "The Treatment of Brachial Plexus Injuries." Link.springer.com. International Orthopaedics, June 1985. Web. 28 Jan. 2013.</ref>. These two methods disturb the nerves of the brachial plexus and cause the injury <ref>Hems, TE.; Mahmood, F. (Jun 2012). "Injuries of the terminal branches of the infraclavicular brachial plexus: patterns of injury, management and outcome.". J Bone Joint Surg Br 94 (6): 799–804.</ref>. | ||
** Traction: Traction, also known as stretch injury, is | ** Traction: Traction, also known as stretch injury, is a mechanism that causes brachial plexus injury. The nerves of the brachial plexus are damaged due to the forced pull by the widening of the shoulder and neck. Traction occurs from severe movement and causes a pull or tension among the nerves. There are two types of traction: downward traction, and upward traction. In downward traction there is tension of the arm which forces the angle of the neck and shoulder to become broader. This tension is forced and can cause lesions of the upper roots and trunk of the nerves of the brachial plexus. Upward traction also results in the broadening of the angle between the arm and chest as occurs when the arm and shoulder are forced upward, with the nerves of T1 and C8 are torn away.<ref>Coene L.N. Mechanisms of Brachial Plexus Lesions. Clinical Neurology and Neurosurgery. 1993:99:24-29.</ref><ref>Orthoinfo. [https://orthoinfo.aaos.org/en/diseases--conditions/brachial-plexus-injuries/ Brachial Plexus injuries]. Available from: https://orthoinfo.aaos.org/en/diseases--conditions/brachial-plexus-injuries/ (last accessed 12.3.2019)</ref> | ||
** Impact: Heavy impact to the shoulder is the second common mechanism | ** Impact: Heavy impact to the shoulder is the second common mechanism for brachial plexus injury. Depending on the severity of the impact, lesions can occur at all nerves in the brachial plexus. The location of impact also affects the severity of the injury, and depending on the location the nerves of the brachial plexus may be ruptured or avulsed. Some forms of impact that cause injury to the brachial plexus are shoulder dislocation, clavicle fractures, hyperextension of the arm, and sometimes delivery at birth. <ref>Jeyaseelan, L.; Singh, VK.; Ghosh, S.; Sinisi, M.; Fox, M. (Jan 2013). "Iatropathic brachial plexus injury: A complication of delayed fixation of clavicle fractures.". Bone Joint J 95–B (1): 106–10.</ref> During the delivery of a baby, the shoulder of the baby may graze against the pelvic bone of the mother. During this process, the brachial plexus can experience damage which results in injury. This is very low compared to the other identified brachial plexus injuries.<ref>Joyner, Benny, Mary Ann Soto, and Henry M. Adam. "Brachial Plexus Injury." Brachial Plexus Injury. Pediatrics in Review, 1 June 2006. Web. 29 Jan. 2013.</ref><br> | ||
{{#ev:youtube|JfsjQwCL0xU}} | {{#ev:youtube|JfsjQwCL0xU}} | ||
== Classification of injuries == | == Classification of injuries == | ||
The various classifications of brachial plexus injury are as follows: | There are [[Brachial Plexus#Classification of Injury|three types of classification systems]] for brachial plexus injuries, with many classification systems. | ||
The various classifications of brachial plexus injury are as follows: | |||
==== Leffert | ==== Leffert Classification System ==== | ||
Leffert Classification System (based on etiology and level of injury): | |||
#* '''I''' Open (usually from stabbing) | #* '''I''' Open (usually from stabbing) | ||
#*'''II''' Closed (usually from motorcycle accident) | #*'''II''' Closed (usually from motorcycle accident) | ||
| Line 64: | Line 63: | ||
#***no proximal stump, no neuroma formation (neg Tinel's) | #***no proximal stump, no neuroma formation (neg Tinel's) | ||
#***pseudomeningocele, denervation of neck muscles are common | #***pseudomeningocele, denervation of neck muscles are common | ||
#*** | #***Horner's sign (ptosis, miosis, anhydrosis) | ||
#**Postgangionic: | #**Postgangionic: | ||
#***roots remain intact; | #***roots remain intact; | ||
| Line 78: | Line 77: | ||
#*'''IVb''' Klumpke (lower root) | #*'''IVb''' Klumpke (lower root) | ||
==== Millesi | ==== Millesi Classification System ==== | ||
#* '''I''': supraganglionic/preganglionic | Millesi Classification System: <ref>Andrew Hodges.A-Z of Plastic Surgery.Oxford University Press.</ref> | ||
#* '''I''': supraganglionic/preganglionic | |||
#* '''II''': infraganglionic/postganglionic | #* '''II''': infraganglionic/postganglionic | ||
#* '''III''': trunk | #* '''III''': trunk | ||
#* '''IV''': cord.Classification on anatomical location of injury | #* '''IV''': cord. Classification on anatomical location of injury | ||
==== | ==== Classification on Anatomical Location of Injury ==== | ||
* Upper plexus palsy (Erb’s palsy in the OBPI cases) involves C5-C6+/-C7 roots<ref>Dodds SD et al.Perinatal Brachial Plexus Palsy. Curr Op Pediat 12: 40-47, 2000.</ref><ref>Kay SPJ. Obstetrical Brachial Palsy. Br J Plastic Surg 51: 43-50, 1998.</ref> | |||
* Lower plexus palsy (Klumpke’s palsy) involves C8-T1 roots (and sometimes also C7) | * Lower plexus palsy (Klumpke’s palsy) involves C8-T1 roots (and sometimes also C7) | ||
* Total plexus lesions involve all nerve roots C5-T1 | * Total plexus lesions involve all nerve roots C5-T1 | ||
* Some authors have included a fourth type,an intermediate type that primarily involves the C7 root.<ref>Al-qattan MM. Self-mutilation in Children with Obstetric Brachial Pexus Palsy. J Hand Surg Br 24B; 5: 547-549, 1999</ref><ref>Shenaq SM et al. Brachial Plexus Birth Injuries and Current Management. Clin Plast Surg 25; 4: 527-536, 1998</ref> | * Some authors have included a fourth type, an intermediate type that primarily involves the C7 root.<ref>Al-qattan MM. Self-mutilation in Children with Obstetric Brachial Pexus Palsy. J Hand Surg Br 24B; 5: 547-549, 1999</ref><ref>Shenaq SM et al. Brachial Plexus Birth Injuries and Current Management. Clin Plast Surg 25; 4: 527-536, 1998</ref> | ||
== Injuries == | == Injuries == | ||
{{#ev:youtube|https://www.youtube.com/watch?v=BnAJNnhC5EY|width}}<ref>Hospital for special surgery. What is a brachial plexus injury. Available from: https://www.youtube.com/watch?v=BnAJNnhC5EY (last accessed 10.3.2019)</ref> | {{#ev:youtube|https://www.youtube.com/watch?v=BnAJNnhC5EY|width}}<ref>Hospital for special surgery. What is a brachial plexus injury. Available from: https://www.youtube.com/watch?v=BnAJNnhC5EY (last accessed 10.3.2019)</ref> | ||
Injuries to roots, trunks and cords of the brachial plexus produce characteristic defects which are as | Injuries to roots, trunks, and cords of the brachial plexus produce characteristic defects which are as follows: <ref name="BD" /> | ||
==== | ====Erb's Paralysis==== | ||
* | ===== Site of Injury ===== | ||
** Abduction and lateral rotation of the arm | The region of the upper trunk of the brachial plexus is called Erb's point. Six nerves meet here. Injury to the upper trunk causes [[Erb's Palsy|Erb's Paralysis]]. | ||
===== Causes of Injury ===== | |||
Undue separation of the head from the shoulder, which is commonly encountered in | |||
* Birth injury | |||
* Fall on shoulder | |||
* During anaesthesia | |||
===== Nerve Roots Involved ===== | |||
* Mainly C5 | |||
* Partly C6 | |||
===== Muscles Paralysed ===== | |||
* Mainly: biceps, deltoid, brachialis, and brachioradialis. | |||
* Partly: supraspinatus, infraspinatus, and supinator | |||
===== Deformity ===== | |||
* Arm: Hangs by the side, adducted and medially rotated | |||
* Forearm: Extended and pronated | |||
* The deformity is known as "Policeman's tip hand" or "Porter's tip hand" | |||
===== Disability ===== | |||
* Abduction and lateral rotation of the arm. | |||
* Flexion and supination of forearm. | |||
* Biceps and supinator jerks are lost. | |||
* Sensations are lost over a small area over the lower part of the deltoid.<br> | |||
{{#ev:youtube|F6XiVA_rYWw}} | {{#ev:youtube|F6XiVA_rYWw}} | ||
==== | ====Klumpke's Paralysis==== | ||
===== Site of Injury ===== | |||
Injury to the Lower trunk of the brachial plexus is called [[Klumpke Paralysis]]. | |||
===== Cause of Injury ===== | |||
* | Undue abduction of the arm, as in clutching a tree branch with the hand during a fall from a height, or sometimes in a birth injury. | ||
*Ulnar flexors of the wrist and fingers (C8). | |||
===== Nerve Roots Involved ===== | |||
* Mainly T1 | |||
* Partly C8 | |||
===== Muscles Paralysed ===== | |||
* Intrinsic muscles of the hand (T1) | |||
* Ulnar flexors of the wrist and fingers (C8). | |||
===== Deformity ===== | |||
Claw hand (position of the hand) due to the unopposed action of the long flexors and extensors of the fingers. In a claw hand there is hyperextension at the metacarpophalangeal joints and flexion at the interphalangeal joints. | |||
===== Disability ===== | |||
* Claw hand | |||
* Cutaneous anaesthesia and analgesia in a narrow zone along the ulnar border of the forearm and hand. | |||
* [http://www.physio-pedia.com/Horner%27s_Syndrome Horner's syndrome]: ptosis, miosis, anhydrosis, enophthalmos, and loss of ciliospinal reflex - may be associated. This is because of injury to sympathetic fibres to the head and neck that leave the spinal cord through nerve T1. | |||
* Vasomotor changes: The [[skin]] areas with sensory loss is warmer due to arteriolar dilation. It is also drier due to the absence of [[Physiology of Sweat|sweating]] as there is loss of sympathetic activity. | |||
* Tropic changes: Long standing case of paralysis leads to dry and scaly skin. The nails crack easily with atrophy of the pulp of fingers.<br> | |||
{{#ev:youtube|fl2qb761_a8}} | {{#ev:youtube|fl2qb761_a8}} | ||
====Injury to | ====Injury to Lateral Cord==== | ||
===== Cause ===== | |||
Dislocation of humerus associated with others. | |||
===== Nerve Involved ===== | |||
Musculocutaneous, lateral root of median nerve. | |||
==== | ===== Muscles Paralysed ===== | ||
* | * [[Biceps Brachii|Biceps]] | ||
* [[Coracobrachialis Muscle|Coracobrachialis]] | |||
* All muscles supplied by the median nerve, except those of hand. | |||
* | |||
* | |||
==Physiotherapy | ===== Deformity and Disability ===== | ||
Physiotherapy treatment for | * Midprone forearm | ||
* Loss of flexion of forearm | |||
* Loss of flexion of the wrist | |||
* Sensory loss on the radial side of the forearm | |||
* Vasomotor and trophic changes. | |||
====Injury to Medial Cord==== | |||
===== Cause ===== | |||
Subcoracoid dislocation of humerus. | |||
===== Nerves Involved ===== | |||
* Ulnar, Medial root of median nerve. | |||
===== Muscles Paralysed ===== | |||
* Muscles supplied by ulnar nerve | |||
* Five muscles of the hand supplied by the median nerve. | |||
===== Deformity and Disability ===== | |||
* Claw hand | |||
* Sensory loss on the ulnar side of the forearm and hand | |||
* Vasomotor and tropic changes as a bone | |||
==Physiotherapy Treatment == | |||
Physiotherapy treatment for Brachial Plexus Injury varies significantly according to the type and severity of the injury. In mild cases physiotherapy and rehabilitation will assist recovery, while in more severe cases surgery and bracing may be needed.<ref>Richmond Rehab. [https://www.richmondrehab.com.au/blog/category/the-brachial-plexus The Brachial plexus]. Available from: https://www.richmondrehab.com.au/blog/category/the-brachial-plexus (last accessed 10.3.2019)</ref> The goal always stays constant, to return to previous level of function and preventing potential disability. | |||
[[File:Rehab equipment.png|frameless|200x200px]] | [[File:Rehab equipment.png|frameless|200x200px]] | ||
==== Physiotherapy | ==== Physiotherapy Treatment Aims ==== | ||
# Development of strength, flexibility, stamina and co-ordination | # Development of strength, flexibility, stamina, and co-ordination | ||
# Maintaining ROM via passive movements, exercise therapy, splinting and positioning and protection of denervated dermatomes.<ref name=":0">Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, et al. Treatment options for brachial plexus injuries. ISRN Orthop. 2014:314137. doi: 10.1155/2014/314137. Available from: Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, et al. Treatment options for brachial plexus injuries. ISRN Orthop. 2014:314137. doi: 10.1155/2014/314137.(last accessed 11.3.2019)</ref> | # Maintaining ROM via passive movements, exercise therapy, splinting and positioning, and protection of denervated dermatomes.<ref name=":0">Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, et al. Treatment options for brachial plexus injuries. ISRN Orthop. 2014:314137. doi: 10.1155/2014/314137. Available from: Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, et al. Treatment options for brachial plexus injuries. ISRN Orthop. 2014:314137. doi: 10.1155/2014/314137.(last accessed 11.3.2019)</ref> | ||
# Functional training and adoption adaptive devices if needed.<ref name=":1">Ausmed. [https://www.ausmed.com/cpd/articles/brachial-plexus-injuries Brachial Plexus Injuries.] Available at: https://www.ausmed.com/cpd/articles/brachial-plexus-injuries (last accessed 10.3.2019)</ref> | # Functional training and adoption adaptive devices if needed.<ref name=":1">Ausmed. [https://www.ausmed.com/cpd/articles/brachial-plexus-injuries Brachial Plexus Injuries.] Available at: https://www.ausmed.com/cpd/articles/brachial-plexus-injuries (last accessed 10.3.2019)</ref> | ||
# Pain control via acupuncture and TENS | # Pain control via acupuncture and TENS | ||
# Managing chronic oedema via education, compression garments and massage therapy.<ref name=":0" /> | # Managing chronic oedema via education, compression garments, and massage therapy.<ref name=":0" /> | ||
A systematic review indicated that physiotherapy interventions like constraint-induced movement therapy, kinesiotaping, electrotherapy, virtual reality simulation, and use of splints or orthotics have positive outcomes for the affected upper limb functionality in obstetric brachial palsy from 0 to 10 years.<ref>Palomo R, Sánchez R. [https://pubmed.ncbi.nlm.nih.gov/32583409/ Physiotherapy applied to the upper extremity in 0 to 10-year-old children with obstetric brachial palsy: a systematic review.] Revista de Neurologia. 2020 Jul 1;71(1):1-0.</ref> | |||
The video clips below highlight the scope of treatment that may be undertaken for the various respective injuries: | |||
*The following video shows treatment for an infant with brachial plexus injury. | |||
{{#ev:youtube|U4aOr1CXAGQ}}<ref>Cincinnatti Children’s. Brachial Plexus Injury: Range of Motion Exercises. Available from: https://www.youtube.com/watch?v=U4aOr1CXAGQ&ab_channel=CincinnatiChildren%27s (accessed 17 February 2024)</ref><div class="row"><div class="col-md-6"> {{#ev:youtube|qQDu-cQ0sRw|250}}<ref>Standford Medicine Children’s Health. Wrist Extension – Brachial Plexus Injury. Available from: https://www.youtube.com/watch?v=qQDu-cQ0sRw&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).</ref> | |||
</div> | |||
<div class="col-md-6"> {{#ev:youtube|ugw2RYxBs5E|250}}<ref>Stanford Medicine Children’s Health. Shoulder External Rotation with Adduction II. Available from: https://www.youtube.com/watch?v=ugw2RYxBs5E&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).</ref> | |||
</div> | |||
</div> | |||
<div class="row"> | |||
<div class="col-md-6"> {{#ev:youtube|IhO17pVsRK0|250}}<ref>Stanford Medicine Children’s Health. Elbow Flexion Bending – Brachial Plexus Injury. Available from: <nowiki>https://www.youtube.com/watch?v=IhO17pVsRK0&ab_channel=StanfordMedicineChildren%27sHealth</nowiki> (accessed 17 February 2024). | |||
</ref> | |||
</div> | |||
<div class="col-md-6"> {{#ev:youtube|T-6NK_X4u1s|250}}<ref>Stanford Medicine Children’s Health. Shoulder External Rotation with Abduction I. Available from: https://www.youtube.com/watch?v=T-6NK_X4u1s&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).</ref> | |||
</div> | |||
</div> | |||
*The following video shows treatment methods that may be employed after a Vespa scooter accident. | |||
{{#ev:youtube|https://www.youtube.com/watch?v=oVWfYUk4vOA|width}}<ref>Ask Dr Jo. Bracial plexus injury stretches and exercise. Available from: https://www.youtube.com/watch?v=oVWfYUk4vOA (last accessed 10.3.2019)</ref> | {{#ev:youtube|https://www.youtube.com/watch?v=KwgHgg3Vfx4|width}}<ref>Mayo clinic. Treatment of Brachial plexus injuries. Available from: https://www.youtube.com/watch?v=KwgHgg3Vfx4 (last accessed 10.3.2019)</ref> | ||
* This video shows treatment that may occur following a simple over stretching of the brachial plexus. | |||
{{#ev:youtube|https://www.youtube.com/watch?v=oVWfYUk4vOA|width}}<ref>Ask Dr Jo. Bracial plexus injury stretches and exercise. Available from: https://www.youtube.com/watch?v=oVWfYUk4vOA (last accessed 10.3.2019)</ref> | |||
* This video demonstrates that BP neuromobility stretching could be used in the rehabilitation of sporting BP injuries. Neuromobilty places an important role in eliminating pain and restoring function. | |||
{{#ev:youtube|https://www.youtube.com/watch?v=F3tKQG8IUrI|width}}<ref>COR. Brachial plexus neuromobility. Available from: https://www.youtube.com/watch?v=F3tKQG8IUrI (last accessed 10.3.2019)</ref> | {{#ev:youtube|https://www.youtube.com/watch?v=F3tKQG8IUrI|width}}<ref>COR. Brachial plexus neuromobility. Available from: https://www.youtube.com/watch?v=F3tKQG8IUrI (last accessed 10.3.2019)</ref> | ||
====Physiotherapy | ====Physiotherapy Following Surgery for Brachial Plexus Injury==== | ||
Surgery is an option for severe brachial plexus injuries, and to be viable should occur within certain timeframes. Surgery aims to regain function by surgical repair. This can take the | Surgery is an option for severe brachial plexus injuries, and to be viable should occur within certain timeframes. Surgery aims to regain function by surgical repair. This can take the form of nerve grafts, nerve transfers, or both, and possible musculoskeletal reconstruction.<ref name=":1" /> | ||
Physiotherapists are crucial in the | Physiotherapists are crucial in the rehabilitative phase post-surgery in the restoring of function via strength, co-ordination, flexibility, ROM, power, and use of splinting if needed. The client needs to be aware that the rehabilitation duration will be for some year(s), and not weeks.<ref name=":1" /> | ||
The video clips below are examples of use of allografts and autografts. These complex procedures will need intensive physiotherapy after to | The video clips below are examples of use of allografts and autografts. These complex procedures will need intensive physiotherapy after to restore the arm to the most optical outcome. | ||
{{#ev:youtube|https://www.youtube.com/watch?v=6YzHsisOFtw|width}}<ref>Hand surgery internation 2015. BP surgery in 3 minutes. Available from: https://www.youtube.com/watch?v=6YzHsisOFtw (last accessed 11.4.2019)</ref> | {{#ev:youtube|https://www.youtube.com/watch?v=6YzHsisOFtw|width}}<ref>Hand surgery internation 2015. BP surgery in 3 minutes. Available from: https://www.youtube.com/watch?v=6YzHsisOFtw (last accessed 11.4.2019)</ref> | ||
{{#ev:youtube|https://www.youtube.com/watch?v=A8h3LgbVTMU|width}}<ref>Phoenics Children's Hospital. Dylan's story. Available from: https://www.youtube.com/watch?v=A8h3LgbVTMU (last accessed 11.4.2019)</ref> | {{#ev:youtube|https://www.youtube.com/watch?v=A8h3LgbVTMU|width}}<ref>Phoenics Children's Hospital. Dylan's story. Available from: https://www.youtube.com/watch?v=A8h3LgbVTMU (last accessed 11.4.2019)</ref> | ||
==== Medical Management - Implications for Physiotherapy ==== | ==== Medical Management - Implications for Physiotherapy ==== | ||
Pain management is often a major issue. Significant pain occurs with root avulsions, causing neuropathic pain. Severe pain will also exhaust the client and if not treated appropriately will hinder | Pain management is often a major issue. Significant pain occurs with root avulsions, causing neuropathic pain. Severe pain will also exhaust the client, and if not treated appropriately will hinder physiotherapy rehabilitation. This is when drugs, such as NSAIDs and opioid drugs, should be used during the first stages (but not with neuropathic chronic pain). Neuropathic pain requires careful use of anti-epileptic drugs (gabapentin and carbamazepine) or antidepressants such as amitriptyline. However, less than a third of clients report significant pain relief with this approach.<ref name=":2">Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, Tagkalegkas I, Sofianos IP. Treatment options for brachial plexus injuries. ISRN orthopedics. 2014 Apr 14;2014. (last accessed 12.3.2019)</ref> | ||
[[File:Pain med.jpg|right|frameless|150x150px]] | [[File:Pain med.jpg|right|frameless|150x150px]] | ||
Physiotherapy may offer an additional source of pain relief with use of TENS, biofeedback, acupuncture and pain neuroscience education [[Pain Neuroscience Education (PNE)|PNE]]. <ref name=":2" /> | Physiotherapy may offer an additional source of pain relief with use of [[Transcutaneous Electrical Nerve Stimulation (TENS)|TENS]], [[biofeedback]], [[acupuncture]], and pain neuroscience education ([[Pain Neuroscience Education (PNE)|PNE]]). <ref name=":2" /> | ||
Dorsal Root Entry Zone (DREZ) operation is an option for persistent pain. The operation aims to destroy the nerve signal transmission from the secondary central sensory centrally. | Dorsal Root Entry Zone (DREZ) operation is an option for persistent pain. The operation aims to destroy the nerve signal transmission from the secondary central sensory centrally. | ||
Spinal Cord Stimulator (SCS) used to mask pain signals before they reach the brain, similar to TENS, but involves a small device and wires being inserted under the skin.<ref>Mayfeild Brain and Spine. [https://mayfieldclinic.com/pe-stim.htm Spinal Cord Stimulation.] Available from: https://mayfieldclinic.com/pe-stim.htm (last accessed 13.3.2019)</ref> | Spinal Cord Stimulator (SCS) used to mask pain signals before they reach the brain, similar to TENS, but involves a small device and wires being inserted under the skin.<ref>Mayfeild Brain and Spine. [https://mayfieldclinic.com/pe-stim.htm Spinal Cord Stimulation.] Available from: https://mayfieldclinic.com/pe-stim.htm (last accessed 13.3.2019)</ref> Cervical SCS can be an effective form of treatment for patients with neuropathic pain from a brachial plexus avulsion<ref>Samer Abdel-Aziz, Ahmed H. Ghaleb; [https://academic.oup.com/painmedicine/article/15/4/712/1931598 Cervical Spinal Cord Stimulation for the Management of Pain from Brachial Plexus Avulsion,] ''Pain Medicine'', Volume 15, Issue 4, 1 April 2014, Pages 712–714, https://doi.org/10.1111/pme.12313 (last accessed 13.3.2019)</ref>. | ||
==== Psychological Management ==== | ==== Psychological Management ==== | ||
Psychological problems and a lack of cooperation by the patient may limit rehabilitation effects and increase disability.[[Brachial | Psychological problems and a lack of cooperation by the patient may limit rehabilitation effects and increase disability.[[Brachial Plexus|[8]]] | ||
[[File:Fun fact.jpg|frameless|100x100px]] Funny Fact........What are armies for? To hang your handy's from! | [[File:Fun fact.jpg|frameless|100x100px]] Funny Fact........What are armies for? To hang your handy's from! | ||
see also [[Nerve Injury Rehabilitation Physiotherapy]] | see also [[Nerve Injury Rehabilitation Physiotherapy]] | ||
== References == | == References == | ||
| Line 222: | Line 259: | ||
[[Category:Paediatrics]] | [[Category:Paediatrics]] | ||
[[Category:Paediatrics - Conditions]] | [[Category:Paediatrics - Conditions]] | ||
[[Category:Peripheral_Nerve_Injuries]] | |||
Latest revision as of 00:23, 10 March 2024
Top Contributors - Aarti Sareen, Lucinda hampton, Kapil Narale, Garima Gedamkar, Kim Jackson, Vidya Acharya, Naomi O'Reilly, Mande Jooste, Laura Ritchie, WikiSysop, Admin, Wendy Walker, Evan Thomas and Meaghan Rieke
Introduction[edit | edit source]
Brachial Plexus (BP) injuries range in severity and cause. The effects may be mild or severe. Unfortunately traumatic incidences of BP injuries are on the rise, often leading to severe social and financial hardships, and greatly affecting quality of life (QOL). This page outlines the main issues arising from BP injuries and the rationale behind their management.[1]
Historical note : Homer (approx. 800 BC) depicted a battle in The Illiad which involved Hector striking Teucer over the clavicle with a rock and preventing him from wielding his bow.[2]

Function[edit | edit source]
Brachial plexus is the network of nerves which runs through the cervical spine, neck, axilla and then into arm or it is a network of nerves passing through the cervico axillary canal to reach the axilla, and innervates the brachium (upper arm), antebrachium (forearm) and the hand. It is a somatic nerve plexus formed by intercommunications among the ventral rami (roots) of the lower 4 cervical nerves (C5-C8) and the first thoracic nerve (T1).
The brachial plexus is responsible for cutaneous and muscular innervation of the entire upper limb, with two exceptions: the trapezius muscle innervated by the spinal accessory nerve (CN XI) and an area of skin near the axilla innervated by the intercostobrachial nerve.
Clinical Anatomy[edit | edit source]
The plexus consists of roots, trunks, divisions, cords and branches.
Roots[edit | edit source]
These consist of the anterior primary rami of spinal nerves C5 - C8 and T1 with contributions from the anterior primary rami of C4 and T2. The origin of the plexus may shift one segment either upward or downward resulting in a pre-fixed plexus or post-fixed plexus respectively. In a prefixed plexus, the contribution by C4 is large, and in that form T2 is often absent. In a post-fixed plexus, the contribution by T1 is large, T2 is always present, C4 is absent, and C5 is reduced in size.[3] The roots join to form trunks as follows:
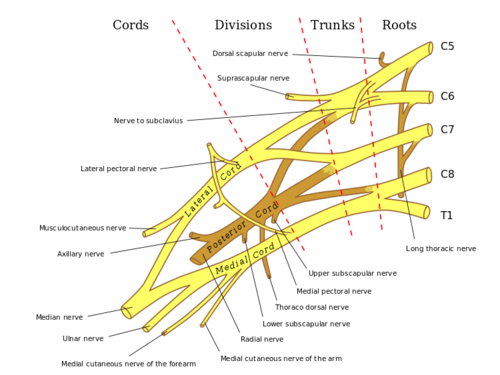 Trunks[edit | edit source]
Trunks[edit | edit source]

- Upper trunk is formed by C5 & C6
- Middle trunk is formed by C7
- Lower trunk is formed by C8 & T1
Divisions (of the trunk)[edit | edit source]
Each trunk divides into ventral and dorsal divisions (which ultimately supply the anterior and posterior aspects of the limb). These divisions join to form cords.
Cords (it forms 3 cords)[edit | edit source]
- The Posterior Cord is formed from the three posterior divisions of the trunks (C5-C8,T1)
- The Lateral Cord is the anterior divisions from the upper and middle trunks (C5-C7)
- The Medial Cord is simply a continuation of the anterior division of the lower trunk (C8,T1)
Branches[edit | edit source]
The specific branches of each cord can be seen on this page
Mechanism of injury[edit | edit source]
Injury to brachial plexus can occur in many ways. These include, contact sports, motor vehicle accidents, or during birth. Grossly, it can be divided into:
- Traumatic, e.g motor vehicle accident, contact sports
- Non traumatic, e.g. obstetric palsy and Parsonage-Turner Syndrome
The network of nerves is fragile and can be damaged by stretching, pressure, or cutting.
- Stretching can occur when the head and neck are forced away from the shoulder, which could happen in a fall from a motorcycle. If severe enough, the nerves can actually avulse, or tear out of their roots in the neck.
- Pressure could occur from crushing of the brachial plexus between the collarbone and first rib, or swelling in this area from injured muscles or other structures [4]. The former examples of events are caused by one of two mechanisms that remain constant during the injury. [5] The two mechanisms that can occur are 'traction' and 'heavy impact' [6]. These two methods disturb the nerves of the brachial plexus and cause the injury [7].
- Traction: Traction, also known as stretch injury, is a mechanism that causes brachial plexus injury. The nerves of the brachial plexus are damaged due to the forced pull by the widening of the shoulder and neck. Traction occurs from severe movement and causes a pull or tension among the nerves. There are two types of traction: downward traction, and upward traction. In downward traction there is tension of the arm which forces the angle of the neck and shoulder to become broader. This tension is forced and can cause lesions of the upper roots and trunk of the nerves of the brachial plexus. Upward traction also results in the broadening of the angle between the arm and chest as occurs when the arm and shoulder are forced upward, with the nerves of T1 and C8 are torn away.[8][9]
- Impact: Heavy impact to the shoulder is the second common mechanism for brachial plexus injury. Depending on the severity of the impact, lesions can occur at all nerves in the brachial plexus. The location of impact also affects the severity of the injury, and depending on the location the nerves of the brachial plexus may be ruptured or avulsed. Some forms of impact that cause injury to the brachial plexus are shoulder dislocation, clavicle fractures, hyperextension of the arm, and sometimes delivery at birth. [10] During the delivery of a baby, the shoulder of the baby may graze against the pelvic bone of the mother. During this process, the brachial plexus can experience damage which results in injury. This is very low compared to the other identified brachial plexus injuries.[11]
Classification of injuries[edit | edit source]
There are three types of classification systems for brachial plexus injuries, with many classification systems.
The various classifications of brachial plexus injury are as follows:
Leffert Classification System[edit | edit source]
Leffert Classification System (based on etiology and level of injury):
- I Open (usually from stabbing)
- II Closed (usually from motorcycle accident)
- IIa Supraclavicular
- Preganglionic:
- avulsion of nerve roots, usually from high speed injuries with other injuries and LOC
- no proximal stump, no neuroma formation (neg Tinel's)
- pseudomeningocele, denervation of neck muscles are common
- Horner's sign (ptosis, miosis, anhydrosis)
- Postgangionic:
- roots remain intact;
- usually from traction injuries;
- there are proximal stump and neuroma formation (pos Tinel's)
- deep dorsal neck muscles are intact, and pseudomeningoceles will not develop;
- Infraclavicular lesion:
- usually involves branches from the trunks (supraclavicular);
- function is affected based on trunk involved
- Preganglionic:
- III Radiation induced
- IV Obstetric
- IVa Erb's (upper root) - waiter's tip hand;
- IVb Klumpke (lower root)
Millesi Classification System[edit | edit source]
Millesi Classification System: [12]
- I: supraganglionic/preganglionic
- II: infraganglionic/postganglionic
- III: trunk
- IV: cord. Classification on anatomical location of injury
Classification on Anatomical Location of Injury[edit | edit source]
- Upper plexus palsy (Erb’s palsy in the OBPI cases) involves C5-C6+/-C7 roots[13][14]
- Lower plexus palsy (Klumpke’s palsy) involves C8-T1 roots (and sometimes also C7)
- Total plexus lesions involve all nerve roots C5-T1
- Some authors have included a fourth type, an intermediate type that primarily involves the C7 root.[15][16]
Injuries[edit | edit source]
Injuries to roots, trunks, and cords of the brachial plexus produce characteristic defects which are as follows: [3]
Erb's Paralysis[edit | edit source]
Site of Injury[edit | edit source]
The region of the upper trunk of the brachial plexus is called Erb's point. Six nerves meet here. Injury to the upper trunk causes Erb's Paralysis.
Causes of Injury[edit | edit source]
Undue separation of the head from the shoulder, which is commonly encountered in
- Birth injury
- Fall on shoulder
- During anaesthesia
Nerve Roots Involved[edit | edit source]
- Mainly C5
- Partly C6
Muscles Paralysed[edit | edit source]
- Mainly: biceps, deltoid, brachialis, and brachioradialis.
- Partly: supraspinatus, infraspinatus, and supinator
Deformity[edit | edit source]
- Arm: Hangs by the side, adducted and medially rotated
- Forearm: Extended and pronated
- The deformity is known as "Policeman's tip hand" or "Porter's tip hand"
Disability[edit | edit source]
- Abduction and lateral rotation of the arm.
- Flexion and supination of forearm.
- Biceps and supinator jerks are lost.
- Sensations are lost over a small area over the lower part of the deltoid.
Klumpke's Paralysis[edit | edit source]
Site of Injury[edit | edit source]
Injury to the Lower trunk of the brachial plexus is called Klumpke Paralysis.
Cause of Injury[edit | edit source]
Undue abduction of the arm, as in clutching a tree branch with the hand during a fall from a height, or sometimes in a birth injury.
Nerve Roots Involved[edit | edit source]
- Mainly T1
- Partly C8
Muscles Paralysed[edit | edit source]
- Intrinsic muscles of the hand (T1)
- Ulnar flexors of the wrist and fingers (C8).
Deformity[edit | edit source]
Claw hand (position of the hand) due to the unopposed action of the long flexors and extensors of the fingers. In a claw hand there is hyperextension at the metacarpophalangeal joints and flexion at the interphalangeal joints.
Disability[edit | edit source]
- Claw hand
- Cutaneous anaesthesia and analgesia in a narrow zone along the ulnar border of the forearm and hand.
- Horner's syndrome: ptosis, miosis, anhydrosis, enophthalmos, and loss of ciliospinal reflex - may be associated. This is because of injury to sympathetic fibres to the head and neck that leave the spinal cord through nerve T1.
- Vasomotor changes: The skin areas with sensory loss is warmer due to arteriolar dilation. It is also drier due to the absence of sweating as there is loss of sympathetic activity.
- Tropic changes: Long standing case of paralysis leads to dry and scaly skin. The nails crack easily with atrophy of the pulp of fingers.
Injury to Lateral Cord[edit | edit source]
Cause[edit | edit source]
Dislocation of humerus associated with others.
Nerve Involved[edit | edit source]
Musculocutaneous, lateral root of median nerve.
Muscles Paralysed[edit | edit source]
- Biceps
- Coracobrachialis
- All muscles supplied by the median nerve, except those of hand.
Deformity and Disability[edit | edit source]
- Midprone forearm
- Loss of flexion of forearm
- Loss of flexion of the wrist
- Sensory loss on the radial side of the forearm
- Vasomotor and trophic changes.
Injury to Medial Cord[edit | edit source]
Cause[edit | edit source]
Subcoracoid dislocation of humerus.
Nerves Involved[edit | edit source]
- Ulnar, Medial root of median nerve.
Muscles Paralysed[edit | edit source]
- Muscles supplied by ulnar nerve
- Five muscles of the hand supplied by the median nerve.
Deformity and Disability[edit | edit source]
- Claw hand
- Sensory loss on the ulnar side of the forearm and hand
- Vasomotor and tropic changes as a bone
Physiotherapy Treatment[edit | edit source]
Physiotherapy treatment for Brachial Plexus Injury varies significantly according to the type and severity of the injury. In mild cases physiotherapy and rehabilitation will assist recovery, while in more severe cases surgery and bracing may be needed.[18] The goal always stays constant, to return to previous level of function and preventing potential disability.

Physiotherapy Treatment Aims[edit | edit source]
- Development of strength, flexibility, stamina, and co-ordination
- Maintaining ROM via passive movements, exercise therapy, splinting and positioning, and protection of denervated dermatomes.[19]
- Functional training and adoption adaptive devices if needed.[20]
- Pain control via acupuncture and TENS
- Managing chronic oedema via education, compression garments, and massage therapy.[19]
A systematic review indicated that physiotherapy interventions like constraint-induced movement therapy, kinesiotaping, electrotherapy, virtual reality simulation, and use of splints or orthotics have positive outcomes for the affected upper limb functionality in obstetric brachial palsy from 0 to 10 years.[21]
The video clips below highlight the scope of treatment that may be undertaken for the various respective injuries:
- The following video shows treatment for an infant with brachial plexus injury.
- The following video shows treatment methods that may be employed after a Vespa scooter accident.
- This video shows treatment that may occur following a simple over stretching of the brachial plexus.
- This video demonstrates that BP neuromobility stretching could be used in the rehabilitation of sporting BP injuries. Neuromobilty places an important role in eliminating pain and restoring function.
Physiotherapy Following Surgery for Brachial Plexus Injury[edit | edit source]
Surgery is an option for severe brachial plexus injuries, and to be viable should occur within certain timeframes. Surgery aims to regain function by surgical repair. This can take the form of nerve grafts, nerve transfers, or both, and possible musculoskeletal reconstruction.[20]
Physiotherapists are crucial in the rehabilitative phase post-surgery in the restoring of function via strength, co-ordination, flexibility, ROM, power, and use of splinting if needed. The client needs to be aware that the rehabilitation duration will be for some year(s), and not weeks.[20]
The video clips below are examples of use of allografts and autografts. These complex procedures will need intensive physiotherapy after to restore the arm to the most optical outcome.
Medical Management - Implications for Physiotherapy[edit | edit source]
Pain management is often a major issue. Significant pain occurs with root avulsions, causing neuropathic pain. Severe pain will also exhaust the client, and if not treated appropriately will hinder physiotherapy rehabilitation. This is when drugs, such as NSAIDs and opioid drugs, should be used during the first stages (but not with neuropathic chronic pain). Neuropathic pain requires careful use of anti-epileptic drugs (gabapentin and carbamazepine) or antidepressants such as amitriptyline. However, less than a third of clients report significant pain relief with this approach.[1]

Physiotherapy may offer an additional source of pain relief with use of TENS, biofeedback, acupuncture, and pain neuroscience education (PNE). [1]
Dorsal Root Entry Zone (DREZ) operation is an option for persistent pain. The operation aims to destroy the nerve signal transmission from the secondary central sensory centrally.
Spinal Cord Stimulator (SCS) used to mask pain signals before they reach the brain, similar to TENS, but involves a small device and wires being inserted under the skin.[32] Cervical SCS can be an effective form of treatment for patients with neuropathic pain from a brachial plexus avulsion[33].
Psychological Management[edit | edit source]
Psychological problems and a lack of cooperation by the patient may limit rehabilitation effects and increase disability.[8]
 Funny Fact........What are armies for? To hang your handy's from!
Funny Fact........What are armies for? To hang your handy's from!
see also Nerve Injury Rehabilitation Physiotherapy
References[edit | edit source]
- ↑ 1.0 1.1 1.2 Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, Tagkalegkas I, Sofianos IP. Treatment options for brachial plexus injuries. ISRN orthopedics. 2014 Apr 14;2014. (last accessed 12.3.2019)
- ↑ Luo TD, Li Z. Brachial Plexus Injuries. [Updated 2018 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482305/ (last accessed 13.3.2019)
- ↑ 3.0 3.1 B.D Chaurasia.Human Anatomy.Vol.1.Fourth Edition.
- ↑ American Society of Surgery of Hand. Available from www.assh.org/Public/HandConditions/Documents/Web_Version_PDF/BrachPlex.pdf
- ↑ Midha, Rajiv, MD. "Neurosurgery." Epidemiology of Brachial Plexus Injuries in a Multitrauma Po... :. Congress of Neurological Surgeons, June 1997. Web. 29 Jan. 2013.
- ↑ Narakas, A.O. "The Treatment of Brachial Plexus Injuries." Link.springer.com. International Orthopaedics, June 1985. Web. 28 Jan. 2013.
- ↑ Hems, TE.; Mahmood, F. (Jun 2012). "Injuries of the terminal branches of the infraclavicular brachial plexus: patterns of injury, management and outcome.". J Bone Joint Surg Br 94 (6): 799–804.
- ↑ Coene L.N. Mechanisms of Brachial Plexus Lesions. Clinical Neurology and Neurosurgery. 1993:99:24-29.
- ↑ Orthoinfo. Brachial Plexus injuries. Available from: https://orthoinfo.aaos.org/en/diseases--conditions/brachial-plexus-injuries/ (last accessed 12.3.2019)
- ↑ Jeyaseelan, L.; Singh, VK.; Ghosh, S.; Sinisi, M.; Fox, M. (Jan 2013). "Iatropathic brachial plexus injury: A complication of delayed fixation of clavicle fractures.". Bone Joint J 95–B (1): 106–10.
- ↑ Joyner, Benny, Mary Ann Soto, and Henry M. Adam. "Brachial Plexus Injury." Brachial Plexus Injury. Pediatrics in Review, 1 June 2006. Web. 29 Jan. 2013.
- ↑ Andrew Hodges.A-Z of Plastic Surgery.Oxford University Press.
- ↑ Dodds SD et al.Perinatal Brachial Plexus Palsy. Curr Op Pediat 12: 40-47, 2000.
- ↑ Kay SPJ. Obstetrical Brachial Palsy. Br J Plastic Surg 51: 43-50, 1998.
- ↑ Al-qattan MM. Self-mutilation in Children with Obstetric Brachial Pexus Palsy. J Hand Surg Br 24B; 5: 547-549, 1999
- ↑ Shenaq SM et al. Brachial Plexus Birth Injuries and Current Management. Clin Plast Surg 25; 4: 527-536, 1998
- ↑ Hospital for special surgery. What is a brachial plexus injury. Available from: https://www.youtube.com/watch?v=BnAJNnhC5EY (last accessed 10.3.2019)
- ↑ Richmond Rehab. The Brachial plexus. Available from: https://www.richmondrehab.com.au/blog/category/the-brachial-plexus (last accessed 10.3.2019)
- ↑ 19.0 19.1 Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, et al. Treatment options for brachial plexus injuries. ISRN Orthop. 2014:314137. doi: 10.1155/2014/314137. Available from: Sakellariou VI, Badilas NK, Stavropoulos NA, Mazis G, Kotoulas HK, Kyriakopoulos S, et al. Treatment options for brachial plexus injuries. ISRN Orthop. 2014:314137. doi: 10.1155/2014/314137.(last accessed 11.3.2019)
- ↑ 20.0 20.1 20.2 Ausmed. Brachial Plexus Injuries. Available at: https://www.ausmed.com/cpd/articles/brachial-plexus-injuries (last accessed 10.3.2019)
- ↑ Palomo R, Sánchez R. Physiotherapy applied to the upper extremity in 0 to 10-year-old children with obstetric brachial palsy: a systematic review. Revista de Neurologia. 2020 Jul 1;71(1):1-0.
- ↑ Cincinnatti Children’s. Brachial Plexus Injury: Range of Motion Exercises. Available from: https://www.youtube.com/watch?v=U4aOr1CXAGQ&ab_channel=CincinnatiChildren%27s (accessed 17 February 2024)
- ↑ Standford Medicine Children’s Health. Wrist Extension – Brachial Plexus Injury. Available from: https://www.youtube.com/watch?v=qQDu-cQ0sRw&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).
- ↑ Stanford Medicine Children’s Health. Shoulder External Rotation with Adduction II. Available from: https://www.youtube.com/watch?v=ugw2RYxBs5E&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).
- ↑ Stanford Medicine Children’s Health. Elbow Flexion Bending – Brachial Plexus Injury. Available from: https://www.youtube.com/watch?v=IhO17pVsRK0&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).
- ↑ Stanford Medicine Children’s Health. Shoulder External Rotation with Abduction I. Available from: https://www.youtube.com/watch?v=T-6NK_X4u1s&ab_channel=StanfordMedicineChildren%27sHealth (accessed 17 February 2024).
- ↑ Mayo clinic. Treatment of Brachial plexus injuries. Available from: https://www.youtube.com/watch?v=KwgHgg3Vfx4 (last accessed 10.3.2019)
- ↑ Ask Dr Jo. Bracial plexus injury stretches and exercise. Available from: https://www.youtube.com/watch?v=oVWfYUk4vOA (last accessed 10.3.2019)
- ↑ COR. Brachial plexus neuromobility. Available from: https://www.youtube.com/watch?v=F3tKQG8IUrI (last accessed 10.3.2019)
- ↑ Hand surgery internation 2015. BP surgery in 3 minutes. Available from: https://www.youtube.com/watch?v=6YzHsisOFtw (last accessed 11.4.2019)
- ↑ Phoenics Children's Hospital. Dylan's story. Available from: https://www.youtube.com/watch?v=A8h3LgbVTMU (last accessed 11.4.2019)
- ↑ Mayfeild Brain and Spine. Spinal Cord Stimulation. Available from: https://mayfieldclinic.com/pe-stim.htm (last accessed 13.3.2019)
- ↑ Samer Abdel-Aziz, Ahmed H. Ghaleb; Cervical Spinal Cord Stimulation for the Management of Pain from Brachial Plexus Avulsion, Pain Medicine, Volume 15, Issue 4, 1 April 2014, Pages 712–714, https://doi.org/10.1111/pme.12313 (last accessed 13.3.2019)

