Cerebral Palsy Introduction
Introduction
[edit | edit source]
The information on this page has developed for you from the expert work of Roelie Wolting alongside the Enablement Cerebral Palsy Project and Handicap International Group.
 |
This page will provide you with information on Cerebral Palsy (CP) such as:
- Definitions,
- Causes
- Epidemiology and aetiology.
This page will provide you with knowledge and better understanding of CP and how it affect children and their families.
Definition[edit | edit source]
Cerebral Palsy (CP) is a disorder of movement and posture that appears during infancy or early childhood resulting from damage to the brain. The damage to the brain is permanent and cannot be cured but the earlier we start with intervention the more improvement can be made.Any non-progressive central nervous system (CNS) injury occurring during the first 2 (some say 5) years of life is considered to be CP. There are several definitions of Cerebral Palsy within the literature, although these may all vary slightly in the way they are worded they are all similar and can be summarised to:
Cerebral Palsy is a group of permanent, but not unchanging, disorders of movement and/or posture and of motor function, which are due to a non-progressive interference, lesion, or abnormality of the developing/immature brain.
This definition specifically excludes progressive disorders of motor function, defined as loss of previously acquired skills in the first 5 years of life.
Time Frame of Brain Injury[edit | edit source]
We only talk about cerebral palsy if the brain damage arises during one of the following periods:
Prenatal period:
- Conception to the onset of labour
Perinatal period:
- 28 weeks intrauterine to 7 days
Postnatal period :
- First two (and some say five) years of life
After the age of 5 we speak of stroke or traumatic brain injury.
Epidemiology[edit | edit source]
The incidence of CP has not declined despite the improved perinatal and obstetric care. Even at centres where optimal conditions exist for perinatal care and birth asphyxia is relatively uncommon, the incidence of CP in term babies has remained the same.

The overall prevalence, all over the world, increased during the last decades, because of increased survival.Here are some facts on the epidemiology of CP:
- The incidence is 2-2,5/1000 live births in Western Countries.
- Some affected children do not survive.
- The prevalence varies between 1-5/1000 babies in different countries.
- There are no reliable statistics from Asian countries.
Aetiology[edit | edit source]
Improved medical care have decreased the incidence of CP among some children, medical advances have also resulted in the survival of children who previously would have died at a young age.
The type of cerebral palsy has also changed:
- In the 60’s around 20% of children with CP had athetoid / dyskinetic cerebral palsy.
- Today only 5 or 10% have this type and 80-90% have spastic CP.
- This decrease is mainly due to advances in the treatment of hyperbilirubinamia.
- The increase of spastic cerebral palsy is because of higher survival rates for (very small premature) babies.
- The most common cause is idiopathic, which means that the cause of damage to the brain during pregnancy is not known.

Risk Factors[edit | edit source]
There are different risk factors for each stage at which a child might develop CP. These can be broken down into; Prenatal, Perinatal and Postnatal.

Prenatal:
- Prematurity (gestational age less than 36 weeks)
- Low birth weight (less than 2500 g), which could be due to poor nutritional status of the mother
- Maternal epilepsy
- Hyperthyroidism
- Herpes simplex virus
- Infections (TORCH = toxoplasmosis, rubella, cytomegalovirus
- Severe toxemia, eclampsia
- Drug abuse
- Trauma
- Multiple pregnancies
- Placental insufficiency
Perinatal:
- Premature rupture of membranes
- Prolonged and difficult labour
- Vaginal bleeding at the time of admission for labour
- Bradycardia
Postnatal (0-2 years):
- Central Nervous System infection (encephalitis,meningitis)
- Hypoxia
- Seizures
- Coagulopathies
- Neonatal hyperbilirubinemia
- Head trauma
There is no way to predict which children’s brain will be damaged by one of these factors, or to what the extent of the damage will be. None of these factors always results in brain damage; and even when brain damage occurs, the damage does not always result in CP.
For example: Some children may have an isolated hearing loss from their meningitis, others will have severe intellectual disability, and some will have CP.
Sub Types of CP[edit | edit source]
There are 3 sub-types of CP and these are:

- Spastic
- Dyskinetic
- Ataxic
Even though they are not clinically precise and may lack reliability, amongst observers these terms can be conceptually useful.
Spastic CP[edit | edit source]
Spastic Cerebral Palsy is characterised by at least two of the following symptoms, which may be unilateral (hemiplegia) or bilateral:
- Abnormal pattern of posture and/or movement
- Increased tone (not necessarily constantly)
- Pathological reflexes (hyper-reflexia or pyramidal signs e.g. Babinski response)

Dyskinetic CP[edit | edit source]
Dyskinetic Cerebral Palsy is Characterised by the following Symptoms:
- Abnormal pattern of posture and/or movement, and
- Involuntary, uncontrolled, recurring, occasionally stereotyped movements of affected body parts
Dyskinetic Cerebral Palsy may be either:
- Dystonic Cerebral Palsy, dominated by both hypokinesia and hypertonia.
or
- Choreo-athetotic Cerebral Palsy, dominated by both hyperkinesia and hypotonia
Ataxic CP[edit | edit source]
Ataxic Cerebral Palsy is characterised by the following symptoms:
- Abnormal pattern of posture and/or movement
- Lost of orderly muscular co-ordination, so that movements are performed with abnormal force, rhythm and accuracy
 |
 |
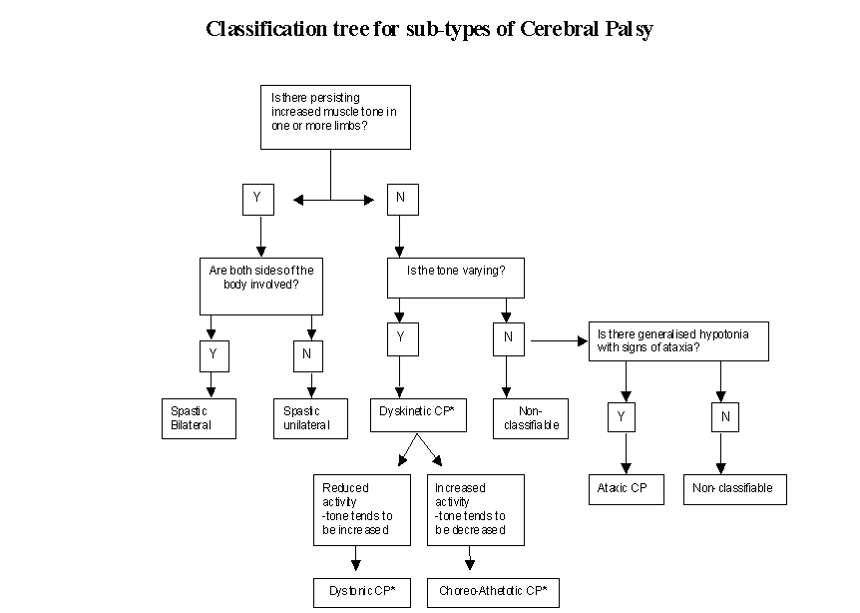
Classification Tree for Sub-types of CP[edit | edit source]
Many children with cerebral palsy have a mixed form of cerebral palsy.
In this page the definition and classification used as agreed on in Europe. More information on definitions, outcome of some studies, exchange of information on clinical practice on CP in Europe you can find, after registering here.
The Surveillance of Cerebral Palsy in Europe was established in 1998.
 Anatomical Classifications[edit | edit source]
Anatomical Classifications[edit | edit source]

Anatomical classification are as follows:
- Unilateral: one side of the body is affected
- Bilateral: both sides of the body are affected
- Spastic CP: are used to distinguish between quadriplegia, diplegia and hemiplegia. Diplegia mainly affects the upper limbs in comparison the lower limbs.
Spastic CP is either bilateral or unilateral.
- Unilateral CP: we refer to as hemiplegia.
- Dyskinetic CP and Ataxic CP: always involve the whole body (bilateral).
Spacticity [edit | edit source]
Spasticity is defined as an increase in the physiological resistance of muscle to passive motion. It is part of the upper motor neuron syndrome characterised by hyperreflexia, clonus, extensor plantar responses and primitive reflexes. Spastic CP is the most common form of CP. Approximately 80% to 90% of children with CP have spastic CP.
Traditionally we recognised 3 types of spastic CP:
| Hemiplegia | Diplegia | Quadriplegia |
 |

|

|
Hemiplegia (unilateral) CP[edit | edit source]
With hemiplegia, one side of the body is involved with the upper extremity generally more affected than the lower. Seizure disorders, visual field deficits, astereognosis, and proprioceptive loss are likely. Twenty percent of children with spastic CP have hemiplegia. A focal traumatic, vascular, or infectious lesion is the cause in many cases. A unilateral brain infarct with posthemorrhagic porencephaly can be seen on magnetic resonance imaging (MRI).
Diplegia (bilateral) CP[edit | edit source]
With diplegia, the lower extremities are severely involved and the arms are mildly involved. Intelligence usually is normal, and epilepsy is less common. Fifty per cent of children with spastic CP have diplegia. A history of prematurity is usual. Diplegia is becoming more common as more low- birth-weight babies survive. MRI reveals mild periventricular leukomalacia (PVL).
Quadriplegia (bilateral) CP[edit | edit source]
With quadriplegia, all four limbs, the trunk and muscles that control the mouth, tongue, and pharynx are involved. Thirty percent of children with spastic CP have quadriplegia. More serious involvement of lower extremities is common in premature babies. Some have perinatal hypoxic ischemic encephalopathy. MRI reveals periventricular leukomalacia (PVL).
Dyskinetic CP[edit | edit source]

Abnormal movements that occur when the child initiates movement are named dyskinesias. Dysarthria, dysphagia, and drooling accompany the movement problem. Intellectual development is generally normal, however severe dysarthria makes communication difficult and leads the outsider to think that the child has intellectual impairment. Sensorineural hearing dysfunction also impairs communication. Dyskinetic CP accounts for approximately 10% to 15 % of all cases of CP. Hyperbilirubinemia or severe anoxia causes basal ganglia dysfunction and results in dyskinetic CP.
Ataxic CP[edit | edit source]
Ataxia is loss of balance, coordination, and fine motor control. Ataxic children cannot coordinate their movements. They are hypotonic during the first 2 years of life. Muscle tone becomes normal and ataxia becomes apparent toward the age of 2 to 3 years. Children who can walk have a wide-based gait and a mild intention tremor (dysmetria). Dexterity and fine motor control is poor. Ataxia is associated with cerebellar lesions. Ataxia is often combined with spastic diplegia. Most ataxic children can walk, but some need walkers.
Mixed CP[edit | edit source]
Children with a mixed type of CP commonly have mild spasticity, dystonia, and/or athetoid movements. Ataxia may be a component of the motor dysfunction in children in this group. Ataxia and spasticity often occur together. Spastic ataxic diplegia is a common mixed type that often is associated with hydrocephalus.
The Brain[edit | edit source]
Here are some of the clinical terminology used when talking about CP:

- Tonus
- Lesion Site
- Spastic
- Cortex
- Dyskinetic
- Basal Ganglia - Extrapyramidal System
- Hypotonic / Ataxic
- Cerebellum
- Mixed
- Diffuse
Knowing were the damage could be located will not influence your interventions. Look at the following pictures of the brain to understand the relationship between the location of the damage and the symptoms.
 |
 |
Problems Regularly Seen with Children with CP[edit | edit source]
This table highlights the problems that children with CP experience within different areas.
| Neurological | Musculoskeletal | Associated Problems |
|
|
|
This image gives a nice pictorial overview of the problems experience by children with CP

Associated Problems[edit | edit source]
There are many associate problems for children with CP, therefore more detail on each are has been provided below:
Learning Difficulties[edit | edit source]
Children with cerebral palsy may experience specific learning difficulties. These may include a short attention span, motor planning difficulties (organisation and sequencing), perceptual difficulties and language difficulties.
Intellectual Difficulties[edit | edit source]
Children with cerebral palsy vary widely in their intellectual capabilities. Some will show the same abilities as other people, despite their physical difficulties. Others will have some degree of intellectual disability, ranging from mild to significant. Speech that is difficult to understand, saliva loss or the movements of children with cerebral palsy, may give the mistaken impression of an intellectual impairment.
Perceptual difficulties[edit | edit source]

Perception is the making sense of information gained from the senses. This enables children to do things such as move around obstacles, judge size and shape of objects and understand how lines are connected to form letters. For those who experience these difficulties, their problems may not become apparent until school or preschool.
Communication / language difficulties[edit | edit source]
Children with cerebral palsy may have difficulties with understanding and expressing ideas. They may require support to follow instructions, construct sentences, give specific information or tell stories that make sense. If a child is having any of these difficulties, it may have an effect on learning.

Speech difficulties[edit | edit source]
Because the muscles of the mouth may be affected, some children may find talking difficult. For those with restricted speech, an alternative communication system may assist them (for example communication board, book or electronic device). Speech that is difficult to understand is not necessarily an indication of intellectual impairment.
Eating and drinking difficulties[edit | edit source]
Cerebral palsy may affect the muscles that open and close the mouth and move the lips and the tongue. Some children may show difficulties in chewing and swallowing food and drink.
Saliva loss[edit | edit source]
Due to poor muscle control some children with cerebral palsy may have varying degrees of saliva loss (dribbling). The dribbling may be more noticeable when they are concentrating on a fine motor task.

Vision[edit | edit source]
Some children may have visual impairments. One of these may be: Strabismus (also known as ‘turned eye’ or ‘squint’) - One or both eyes are turned in or out and are prevented from working together. This may lead to double vision or focusing with one eye at a time.
Hearing[edit | edit source]
Some children with Cerebral Palsy may have hearing loss.

Epilepsy[edit | edit source]
If this problem is present, the doctor may aim to control the seizures by choosing medicine that suits the child. It may be necessary to change the medication several times before the seizures are controlled. Sometimes they cannot be controlled.
Other Associated Problems[edit | edit source]
A systemic review was performed in order to compile information on the rates of co-occurring impairments, diseases, and functional limitations in children with cerebral palsy. Here is an overview of the results:
- 3 in 4 were in pain
- 1 in 2 had an intellectual disability
- 1 in 3 could not walk
- 1 in 3 had a hip displacement
- 1 in 4 could not talk
- 1 in 4 had epilepsy
- 1 in 4 had a behaviour disorder
- 1 in 4 had bladder control problems
- 1 in 5 had a sleep disorder
- 1 in 5 dribbled
- 1 in 10 were blind
- 1 in 15 were tube-fed
- 1 in 25 were deaf
You can read more about this review here.
Diagnosis[edit | edit source]
Cerebral palsy is one of the main causes of childhood disabilities, with many different signs, symptoms and challenges. There is no one test to confirm if a child has cerebral palsy or something else. There is no blue print of interventions for a child with cerebral palsy, and
each child is different and unique. Classification of gross motor, fine motor and communication will help medical professionals and the family to better understand the abilities of the child and what to focus on for interventions.
The diagnosis of cerebral palsy is based on a clinical description. The diagnosis is not based on the result of a (biological) test or on imaging findings. Consequently, the diagnosis can be subject to some degree of variability. This means that two paediatricians may disagree on a diagnosis of CP for the same child. It is sometimes difficult for even professionals to differentiate between bilateral spastic CP and dyskinetic CP.
Ideally a paediatrician will give the diagnose, or the child's Neurologist. But some children with CP in developing countries have never seen a doctor. There are also many children in developing countries with CP who have seen many doctors previously, but with no good explanation of the meaning and consequences of the diagnoses.
Life Expectancy[edit | edit source]
Mortality in CP is extremely variable. Life expectancy is normal in most diplegic and hemiplegic children who receive adequate medical care and have strong family support. Some severely affected quadriplegics die of malnutrition, infections or respiratory problems before reaching adolescence.
In some very poor and poor resource areas children with cerebral palsy may not reach the age of 5 years
Interventions with CP [edit | edit source]
The aim and types of interventions are unique for each child with CP, as their needs are all different depending on the level of disability. This table gives a great overview of the aims of treatment / interventions for each level of disability.
| Mild | Moderate | Severe |
| Intervention will focus of appearance and integration | Intervention will focus on independence and self-care skill | Intervention will focus on comfort and enhanced care |
Communication[edit | edit source]
Communication is necessary to express thoughts, feelings and needs. Every individual with CP needs a way to communicate to be part of the family and the community. If the child can produce comprehensible sounds and syllables by 2 years of age, they will probably have normal verbal communication, but considerations need to be made for those whose communication skills are severely affected. Alternative methods such as communication methods such as simple communication boards in children who have difficulty speaking.
Activities of Daily Living (ADL)[edit | edit source]
Activities of daily living are self-care activities such as feeding, toileting, bathing, dressing, and grooming in addition to meal preparation and household maintenance. Dyskinetic and total body involved children have problems of dexterity and fine motor control that prevent independence in activities of daily living. Hemiplegic and diplegic children can become functional in these areas. They sometimes need help of (occupational) therapy. Family attitude is a critical factor determining the level of independence of a child. Overprotection results in a shy and passive individual who has not gained self-care abilities.
Moblity[edit | edit source]

Children have to explore their surroundings to improve their cognitive abilities. Mobilisation is crucial for the young child with disability to prevent secondary mental deprivation. The use of wheelchairs or other mechanical assertive devices can help to promote independent mobility in the community, if the child cannot mobilise through walking. Mobility is important to function in the fast paced societies and people who have difficulty moving are always at a disadvantage. In the adult, becoming an independent member of the society and earning a living depends upon independent mobility. Families view ambulation as the most important issue during childhood. Every effort must be made to increase the child’s ability to walk; however, walking depends more on the extent of the child’s neurological impairment rather than the amount of physical therapy, surgery or bracing that they receive. The child can achieves their own maximum potential with practice.
Focus on ambulation should not result in neglecting communication and cognitive development. Priorities change in adolescence as they need education, independence, and an active social life. Although ambulation is still important, it is needed less to function. Learning how to use computers may benefit the adolescent in the long term rather than being able to take a few assisted steps.
Mobility is important for the child, whereas social identity and independence are more valuable for the adolescent.
Additional Resources [edit | edit source]
Here are some additional resources related to CP:

