Resisted Exercise Initiative (RExI)
This article is currently under review and may not be up to date. Please come back soon to see the finished work!
Introduction[edit | edit source]
RExI is an abbreviation for the PT Knowledge Broker facilitated project started in April 2019: Resisted Exercise Initiative (RExI) – Use of resisted exercise by physiotherapists for elderly patients in British Colombia (BC) Hospitals.
The current volume and level of acuity of elderly patients in acute care settings challenges physical therapists to address all needs. One related aspect of practice that is receiving increasing attention is the optimal prescription of resistance exercise in these settings.
Goal: To support best practice in use of resisted exercise by physical therapists for elderly patients in BC Hospitals.
Objectives:
- To determine existing practice.
- To identify opportunities to support enhanced practice.
- To undertake knowledge translation (KT) strategies to target barriers to enhance using of resisted exercise.
- To evaluate effect of introduction of the KT strategies.

This project will:
- Describe current practice to confirm whether there is ‘a gap’ between current actual and desired evidence-based practice for PTs in BC.
- Determine the barriers to desired evidence-based practice from the perspective of the front-line public-practice PT.
- Map the barriers identified to categories identified by KT/implementation/behaviour change science.
- Using KT/implementation/behaviour change science and resources to identify targeted KT strategies to address the barriers.
- Develop/undertake, disseminate & support implementation of the targeted strategies.
- Re-evaluate practice post-implementation of the strategies.
Resistance Exercise Tool Kit[edit | edit source]
Definition&Benefits[edit | edit source]
Defined as movement using body weight or external resistance that improves muscular strength ,power , endurance and it may positively impact mobility ,function and independence.[1]

Benefits of resistance exercise ;[2][3]
- Improving muscle strength and tone.
- Maintaining flexibility and balance .
- Weight management and increased muscle to fat ratio.
- May help in prevent or reduce cognitive decline in older people.
- Greater stamina ( people will not tire easily due to improved body strength ).
- Prevention or control of chronic conditions ...eg (back pain, heart disease , arthritis , obesity &depression ).
- Pain management .
- Improved posture and decrease risk of injury.
- Decrease risk of osteoporosis by helping in increasing bone density.
- Improve sense of wellbeing , boost confidence and self-esteem.
A statement from National Strength and Conditioning Association highlighted the benefits of resistance exercise to older people ( Fragala et al .2019).[4]
Aproberly designed resistance training programme can help in :[5]

- Counteracting the age related changes in human skeletal muscle.
- Enhance the muscular strength ,power and neuromuscular functioning of senior citizens.
- Improve older adults resistance to injuries and catastrophic events like : falls.
- Improve mobility , physical functioning , performance of daily activities (ADL) and preserve independence.
- Help in promoting psychosocial well-being of older adults.
Also Fragala et al .2019 recommended the resisted exercise training programme should be matched appropriately to the individuals'abilities and goals.
Considerations & Flags[edit | edit source]
Before prescribing resistance exercise , liaise with patient's physician your treatment plan and discuss the signs and symptoms to monitor :[6][7][8]
| Flags &Contraindications |
|---|
|
- Pain
- Strength
- Function
- Ability to learn
- Comorbidities and medications
- Oxygen Saturation and requirements
- Needs Supervision
- Fatigue Management
- Mobility Assessment
- Hemoglobine (hgb) (monitor patients with levels less than 70g/L)
- Blood Pressure
- HR
- Oxygen Saturation SPO2.
- Platelets
- Physical Activity vital signs (PAVS)*
- Rapid Assessment of Physical Activity *
- Physical Activity Screening for Elderly *
- Risks of coronary Artery Disease
- Uncontrolled hypertension
- People with implanted pacemakers and defibrillators
- Musculoskeletal Limitation
- Joint Pain and Instability (from arthritis or any other causes)
- Diabetes at any age
- Lines
- Aids ( eye wear , hearing aids & gait aids )
Exercise Physiology Foundation[edit | edit source]
1-Muscle strength & life course[edit | edit source]

Muscle strength decrease through adult years and life course . There is a strong link between decreased muscle strength and falls,immobility and mortality [4] .
Loss in strength can be moderated by maximizing muscle in early adulthood , maintaining strength in middle age and minimizing loss in older age. This can be achieved through resistance exercise training .[4] [9] *(diagram)
Hospitalized older adults may experience some problems from immobility like: Muscle atrophy , Sarcopenia [9], cachexia.....eg
1- Muscle Atrophy[edit | edit source]

Types of muscle atrophy[10][11]
- Disuse or physiologic Atrophy.
- Neurogenic Atrophy.[12]
- Myogenic Atrophy.
2- Sarcopenia[edit | edit source]

Is defined as a progressive and generalized skeletal muscle disorder associated with an increased likelihood of adverse outcomes like falls, fractures, physical disability and mortality.[9] Sarcopenia is considered a muscle disease ( muscle failure ) with the following 3 criteria :
- Low muscle strength.
- Low muscle quantity and quality.
- Low physical performance.
- Probable sarcopenia is identified by criteria 1.
- Diagnosis is confirmed by additional documentation of criteria 2.
- sarcopenia is considered severe if 1,2 &3 criteria are met.
3- Cachexia[edit | edit source]
Cachexia is a complex metabolic syndrome associated with underlying illness and characterized by loss of muscle with or without loss of fat mass. The prominent clinical feature of cachexia is weight loss in adults (corrected for fluid retention) or growth failure in children (excluding endocrine disorders). Anorexia, inflammation, insulin resistance, and increased muscle protein breakdown are frequently associated with cachexia. Cachexia is distinct from starvation, age-related loss of muscle mass, primary depression, malabsorption, and hyperthyroidism and is associated with increased morbidity.Sarcopenia is one of the factors that may cause cachexia.[13][14]
2-Regeneration Of Injured Skeletal Muscle[edit | edit source]
If the patient has sustained an injury to skeletal muscle, the following information regarding types of muscle injuries and phases of muscle healing may be helpful in planning the progression of resisted exercise.[15]
3- Principles Of Strength and Conditioning[edit | edit source]

For further information you can access strength and conditioning page
The Effects of Resistance Exercise on Muscle[edit | edit source]
Key terms[16]
- Hypertrophy[17]

Increase in skeletal muscle mass by increasing muscle fibre size[18]
- Strength
The ability to produce force
- Power
The ability to produce force at a high speed of movement (force x distance/time)
- Motor Unit[16]
Consists of an alpha motor neuron and the muscle fibres innervated by

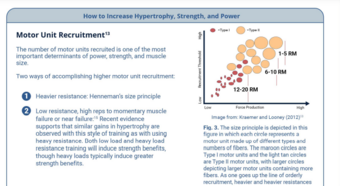
Type I muscle fibres are considered slower but more fatigue-resistant fibres (e.g. beneficial for long distance runners).
Type II fibres are considered the faster, more powerful fibres, but are also more susceptible to fatigue (e.g. more beneficial for sprinters and lifters)
- Henneman's Size Principle[20]
As levels of activation increase (either through increased load or speed), larger motor units are recruited (i.e. Type I, Type Ila, and Type llb in succession).
4- Prescription Principles (Older Adults)[edit | edit source]
- Assessment
1- Screen for contraindications .
2- Resistance exercise has been shown to be safe in the frail, elderly population, but if you have any questions or are unsure of medical stability for resistance exercises, check with the primary care provider, or use https://eparmedx.com/.

Goal is to work towards 2-3 sets of 1-2 multi-joint exercises per major muscle group (6-12 reps), 70-85% 1RM, 2-3 times/week (non-consecutive days) You can start at one set for beginners or older adults with frailty.
Appropriate Intensity [1][21][22]
-Free weights, machines, or bands or body weight can be used. Beginners, frail older adults, or those with functional limitations, benefit from machine-based resistance training, training with resistance bands and isometric training to help simplify and/or stabilize movements.High functioning older adults gain added benefit from free-weight resistance training as these exercises may engage additional muscles for support and stability and are more similar to movements used in activities of daily living Y.
- Lift and lower the weight in a controlled manner with a focus on good form.
- Rest 1.5-3 min between sets. The greater the intensity, the longer rest period is needed. The rest allows the muscles energy stores to be restored and therefore you can maximize the intensity of each set.
-Exercises done with the muscles in a fatigued state can lead to poor form and injury Y.
-Primary attention should be given to lower body exercises as age-related reductions are more pronounced in the lower body.
-In general, larger muscle groups should be worked before smaller muscle groups and multi-joint exercises (encouraged) should be done before uni-joint.
Muscle Groups
► The specific muscle groups targeted can be based on manual muscle testing, dynamometer testing, or functional muscle testing.Exercise selection should include major muscle groups targeted through multi-joint movements. Some examples of exercises that may be included in a whole-body resistance exercise session for general weakness or prevention of decline/deconditioning (if there is not a targeted area of weakness) include:
(see standardized exercise programs for more specifics)
Basic
• Squat (leg press if unable to do squat)
• Knee extension
• knee flexion (leg curl or Romanian deadlift; deadlift with caution in elderly patients with spine issues)
• Chest press
• Seated low row
Complementary
• Hip adduction/abduction
• Hip flexion/extension
• Calf raise (standing or seated)
• Elbow flexion/extension
• Core/abdominals
One multi-joint exercise should be prescribed for major muscle groups although lower limbs may respond better to exercise.
Monitoring and progression
Progression should follow general exercise principles of individualization, periodization, and progression.
For progression of intensity, continue to use the method utilized for your initial strength testing prescription.
Progression
The following summarizes different methods of progression:
► It is important to explain to patients that, with resistance training, they should expect some delayed onset muscle soreness.
For patients with medical issues, continue to monitor as per clinical judgement (e.g. SpO2 with patients with COPD; Borg for patients who are short of breath; heart rate for patients with a cardiac condition; or blood sugar for patients with diabetes
Additional Notes
Where possible, resistance exercise should be prescribed in combination with aerobic training because both types of exercise elicit distinct benefits .To optimize functional capacity, resistance training programs should include familiarization to training in which the patients' body mass is used for resistance and in which daily activities are simulated (like sit-to-stand). High speed motion (at low to moderate intensity 30-60% 1 RM) can also be incorporated to promote greater improvements in the functional task performance of older adults Y .For more information about resistance training in the frail older adult, see the "Special Population " section on frailty.
Grip strength is a robust proxy indicator of overall strength. Grip strength of <26kg in men and <16 kg in women have been established as a biomarker of age related disability and early mortality and have been strongly related to incident mobility limitations and mortality.
Simple Progression Recommendations
Volume: Manipulate sets, reps, weight
Equipment: Body weight, bands, machine, free weight
Stability: Lying, seated, kneeling, standing both feet on flat surface, standing single leg on flat surface, standing both legs on unstable surface, standing single leg on unstable surface.
Behaviour Change[edit | edit source]

Supporting Your Patient to Participate in Strength Training
References[edit | edit source]
- ↑ 1.0 1.1 1.2 Loveless MS, Ihm JM. Resistance exercise: how much is enough?. Current sports medicine reports. 2015 May 1;14(3):221-6.
- ↑ Exercise prescription principles - Exercise.trekeducation.org https://exercise.trekeducation.org/2021
- ↑ American Physical Therapy Association | Choosing Wisely Choosing Wisely | Promoting conversations between providers and patients https://www.choosingwisely.org/societies/american-physical-therapy-association/
- ↑ 4.0 4.1 4.2 4.3 Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD, Ryan ED. Resistance training for older adults: position statement from the national strength and conditioning association. The Journal of Strength & Conditioning Research. 2019 Aug 1;33(8).
- ↑ Ratamess N. ACSM's foundations of strength training and conditioning. Lippincott Williams & Wilkins; 2021 Mar 15.
- ↑ Kim J, Fanola C, Ouzounian M, Hughes GC, Pyeritz RE, Gleason TG, Evangelista-Masip A, Braverman AC, Montgomery DG, Ehrlich M, Schermerhorn M. ACUTE AORTIC DISSECTION IN PATIENTS WITH MITRAL VALVE DISEASE. Journal of the American College of Cardiology. 2020 Mar 24;75(11_Supplement_1):2255-.
- ↑ Jeevanantham D, Rajendran V, McGillis Z, Tremblay L, Larivière C, Knight A. Mobilization and exercise intervention for patients with multiple myeloma: clinical practice guidelines endorsed by the Canadian Physiotherapy Association. Physical therapy. 2021 Jan;101(1):pzaa180.
- ↑ Stiller K, Phillips A. Safety aspects of mobilising acutely ill inpatients. Physiotherapy theory and practice. 2003 Jan 1;19(4):239-57.
- ↑ 9.0 9.1 9.2 Cruz-Jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y, Schneider SM, Topinková E. Sarcopenia: European consensus on definition and diagnosis Report of the European Working Group on Sarcopenia in Older PeopleA. J. Cruz-Gentoft et al. Age and ageing. 2010 Jul 1;39(4):412-23.
- ↑ He N, Ye H. Exercise and muscle atrophy. Physical Exercise for Human Health. 2020:255-67.
- ↑ Ding S, Dai Q, Huang H, Xu Y, Zhong C. An overview of muscle atrophy. Muscle Atrophy. 2018:3-19.
- ↑ 12.0 12.1 Dumitru A, Radu BM, Radu M, Cretoiu SM. Muscle changes during atrophy. Muscle Atrophy. 2018:73-92.
- ↑ Evans WJ, Morley JE, Argilés J, Bales C, Baracos V, Guttridge D, Jatoi A, Kalantar-Zadeh K, Lochs H, Mantovani G, Marks D. Cachexia: a new definition. Clinical nutrition. 2008 Dec 1;27(6):793-9.
- ↑ Ding S, Dai Q, Huang H, Xu Y, Zhong C. An overview of muscle atrophy. Muscle Atrophy. 2018:3-19.
- ↑ Järvinen TA, Järvinen M, Kalimo H. Regeneration of injured skeletal muscle after the injury. Muscles, ligaments and tendons journal. 2013 Oct;3(4):337.
- ↑ 16.0 16.1 Kraemer WJ, Looney DP. Underlying mechanisms and physiology of muscular power. Strength & Conditioning Journal. 2012 Dec 1;34(6):13-9.
- ↑ Phillips SM. A brief review of critical processes in exercise-induced muscular hypertrophy. Sports Medicine. 2014 May;44(1):71-7.
- ↑ Khan KM, Scott A. Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. British journal of sports medicine. 2009 Apr 1;43(4):247-52.
- ↑ Deschenes MR. Effects of aging on muscle fibre type and size. Sports medicine. 2004 Oct;34(12):809-24.
- ↑ Schoenfeld BJ, Grgic J, Ogborn D, Krieger JW. Strength and hypertrophy adaptations between low-vs. high-load resistance training: a systematic review and meta-analysis. The Journal of Strength & Conditioning Research. 2017 Dec 1;31(12):3508-23.
- ↑ Camp PG, Reid WD, Chung F, Kirkham A, Brooks D, Goodridge D, Marciniuk DD, Hoens AM. Clinical decision-making tool for safe and effective prescription of exercise in acute exacerbations of chronic obstructive pulmonary disease: results from an interdisciplinary Delphi survey and focus groups. Physical therapy. 2015 Oct 1;95(10):1387-96.
- ↑ Uthman OA, Van Der Windt DA, Jordan JL, Dziedzic KS, Healey EL, Peat GM, Foster NE. Exercise for lower limb osteoarthritis: systematic review incorporating trial sequential analysis and network meta-analysis. Bmj. 2013 Sep 20;347.


{kind=link}
{kind=link}
{kind=link}