Psoriatic Arthritis
Original Editors - Stacy Downs as part of the Bellarmine University's Pathophysiology of Complex Patient Problems project.
Top Contributors - Stacy Downs, Keri Gibson, Sarah Yurt, Admin, Kim Jackson, Oyemi Sillo, Elaine Lonnemann, Wendy Walker, WikiSysop, Nikhil Benhur Abburi and 127.0.0.1
 Definition/Description[edit | edit source]
Definition/Description[edit | edit source]

Psoriatic arthritis is a chronic progressive inflammatory joint disease that can be associated with psoriasis. The condition may affect both peripheral joints and the axial skeleton causing pain, stiffness, swelling, and possible joint destruction. This joint pathology progresses slowly and can be more of a nuisance than disabling. Psoriatic arthritis is considered a seronegative spondyloarthropathy. The fact that it is "seronegative" means that the blood tests negative for a certain factor that is present in rheumatoid arthritis. Spondyloarthropathy is a word that describes a group of conditions that all share two common characteristics. First, there is the presence of arthritis that affects the spine or extremities with evidence of family inheritance. Secondly, inflammation occurs in the ligaments, tendons, and occasionally in organs such as the eye.[1]
Prevalence[edit | edit source]
- Occurs in 6%-42% of persons that have psoriasis
- Approximately 2% of general population has psoriasis
- Psoriatic arthritis is estimated to have a prevalence of 0.1%-0.25% in the US
- Equal prevalence in both males and females [2]
- Can occur at any age but typically occurs between ages of 30-50 years old
*80-90% chance of having psoriatic arthritis if one of your first degree relatives has the disorder
 Arthritis Mutilans
Arthritis Mutilans Arthritis Mutilans Presentation #2Characteristics/Clinical Presentation
Arthritis Mutilans Presentation #2Characteristics/Clinical Presentation
[edit | edit source]


Psoriatic arthritis causes inflammation, pain, stiffness, and swelling in joints as well as ligaments and tendons at their insertion sites. Bone, tendons, enthesis, cartilage, synovial membrane, skin, and nails may all be affected by the condition. During the initial stages it is the tendons, synovia, and articular capsule that are primarily affected. As the condition progresses, tendon and bone becomes altered. Marked joint destruction may occur in some individuals.
Psoriatic arthritis is a condition that may often be misdiagnosed due to the wide variety of clinical presentations. Even though it is associated with psoriasis, in 15% of cases the arthritis appears first. In cases where psoriasis appears first, it usually occurs 8-10 years before. Mild cases of psoriasis may be incorrectly diagnosed as exzema, seborrheic dermatitis, or atopic dermatitis. This may further complicate diagnostic accuracy. [1]Expression of the disease varies greatly from one person to the next. Its course is unpredictable, ranging from mild to severe and destructive. In around 70% of cases, psoriasis precedes arthritis. For the majority, joint symptoms do not appear until approximately ten years after the first signs of psoriasis. Both occur simultaneously in 15% of cases. Extra articular manifestations of psoriatic arthritis include inflammatory eye disease, such as vitis and iritis, renal disease, mitral valve prolapse, and aortic regurgitation. Around The urethra may also become inflamed. Fatigue may also be a significant problem for people with psoriatic arthritis.[1]
Five Clinical Presentations of Psoriatic Arthritis
- Distal Interphalangeal Dominant - Only DIPs of fingers or toes are affected with nail changes often present.
- Symmetric Arthritis - This type resembles rheumatoid arthritis. Five or more joints will be affected in a symmetrical pattern throughout the body.
- Asymmetric Arthritis - This is the most common type making up 70% of cases. Four or less joints are affected in an asymmetrical pattern.
- Spondylitis - This type causes inflammation in the spine. The neck, low back, and SI joints are often affected. It may coincide with symptoms throughout the extremities.
- Arthritis Mutilans - This type is the most severe and destructive. Mutilation of the small joints of fingers and toes often occurs. The fingers may appear sausage like due to swelling. This is the most rare form, occuring in less than 1% of all cases.[1]
Diagnosis of psoriatic arthrits may often be delayed since there are no identified biomarkers at this time. If left untreated psoriatic arthritis may lead to severe physical limitations and disability. Early diagnosis is critical to slow the progression of the disease with medications.
Associated Comorbidities[edit | edit source]
- Psoriasis
- Ankylosing Spondylitis
- Systemic Lupus Erythematosus
- Giant Cell Arteritis
- Sjogren's Syndrome
- Chron's Disease
- Metabolic Syndrome
- Atherosclerosis
- Coronary Heart Disease
- Depression
Medications[edit | edit source]
Goals of treatment: Reduce pain, stiffness and swelling, inhibit disease progression, optimize function, decrease effects of the disease, and improve the patients quality of life.[3]
Mild disease
- Non-steroidal Anti-Inflammatory Drugs (NSAIDS)
- Local Corticosteroid Injections (must be careful because can cause flare up of psoriasis in some patients.)[3]
'NOTE: Neither NSAIDS or intra articular corticosteroids will stop structural joint damage'
Moderate to Severe Disease
- Disease-Modifying antirheumatic drugs (DMARD) also called Slow-Acting Antirheumatic Drugs-these drugs will suppress the disease activity (SAARD) www.webmd.com/rheumatoid-arthritis/modifying-medications
- Anti-tumor necrosis factor: should be used if patient do not respond well to NSAIDS or DMARDS. These can include adalimumab, etanercept, golimumab and infliximab[3] www.drugs.com/mtm/infliximab.html,www.drugs.com/cdi/etanercept.html,www.drugs.com/cdi/alefacept.html These drugs which are given intravenously reduce T-cells so that less tumor necrosis factor is released. Both are highly effective but do come with risks since they weaken the immune system.[1]www.psoriasisguide.ca/medical_treatment/immunobiologics/biologic_drugs.html
Diagnostic Tests/Lab Tests/Lab Values[edit | edit source]
- There is no definitive test. Diagnosis is made by ruling out other conditions.
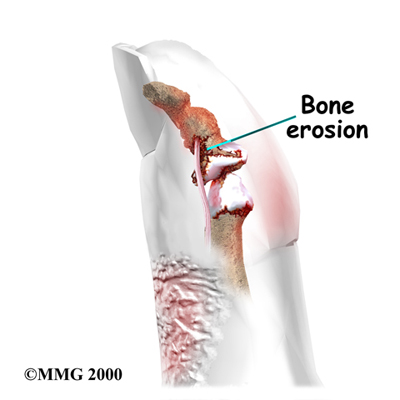
- X-rays are the current gold standard. However, signs of psoriatic arthritis often do not appear on radiographs until later stages of the disease when bone erosion has occured.[4]
- Contrast enhanced ultra sound is starting to play a leading role since it can detect changes in bone and soft tissue much sooner than X-rays.[4]
- Early studies have demonstrated that ultrasound and MRI are both highly sensitive to early inflammatory joint changes that occur in psoriatic arthritis. [4]
- DIP erosive changes on X-rays may support the diagnosis.
- Blood work will be done to detect for the HLA-B27 since it is a common histocompatibility complex marker in people with psoriatic arthritis.
- A blood test for rheumatoid factor should be done to rule out rheumatoid arthritis.
- A blood test for antinuclear antibody (ANA) should be done to rule out Lupus.
- CBC should be done to check for a reduction in red blood cells that sometimes occurs in psoriatic arthritis.[1]
- A joint aspiration may be done in which a syringe removes fluid from a joint. The fluid is then examined for the presence of infection, crystals, and white blood cells.[1]
Causes[edit | edit source]
Genetic Psoriatic arthritis seems to have a genetic cause, although the exact marker genes have not been identified. Having a first-degree realtive with psoriatic arthritis increases the likihood of contracting the disease by 80-90%.[2] There are currently genome studies being done to determine the biomarkers associated with psoriatic arthritis. [5]
Environmental
Trauma and infection may trigger the developement of psoriatic arthritis.[1]
Immunologic
The immune system is believed to play a key role in the development of psoriatic arthritis. Cytokines have been found to be in high abundance in the joints of people with psoriatic arthritis. Cytokines are inflammatory messengers that are released when T cells are activated. Tumor necrosis factor is a specific cytokine that is abundant in the skin, blood, and joints of patients with psoriatic arthritis and psoriasis. The job of tumor necrosis factor is to regulate inflammation in the body, and it should be present in low levels. Continued high levels of tumor necrosis factor leads to inflammation in the body. Blocking this particular cytokine often leads to significant improvement in psoriatic arthritis.[1]
Medical Management[edit | edit source]
- It is ideal for patients to have coordinated care between a dermatologist and rheumatologist since the majority have both skin and joint manifestations of the disease. Since disease manifestations first begin within the skin and nails, it is likely the patients first point of contact is a dermatologist, putting them in an optimal position to be the first to screen for PsA. There are several screening questionnaire available for PsA including the TOPAS, PEST, PASE, and the EARP, all of which are filled out by the patient. Some of which have been tested to show good sensitivity and specificity. Once the dermatologist has detected PsA in a patient they are then able to refer to a rheumatologist, who plays a key role in the medical management of psoriatic arthritis. Medications are important to slow the progression of the disease and improve quality of life. Many of the drugs used to treat this disease may be harmful to the kidneys and/or gastro intestinal system. The rheumatologist will monitor closely the renal and GI system of patients that are on medications.
- When determining treatment for PsA, an assessment is done to help focus in on the clinical domains present in the patient. They include arthritis, enthesitis, dactylitis, spondylitis, psoriasis, and nail disease. Usually, measures are used that focus on the skin or joints that result from RA and psoriasis. However, more recently, the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA)have been working on a composite measure that attempts to take the whole patient into account. The measure will allow them to assess the several domains of the disease, and monitor it's activity as well as the patients response to therapy. Furthermore, GRAPPA has developed a grid to help determine treatments based on the severity of the disease. Currently, there are two sets of PsA treatments. The first one is the EULAR, which is a set of recommendations to guide the clinician on treatment steps and medication. And the second is the GRAPPA group recommendations, based on a literature review of treatment of the domains and skin. Treatment choices are based off a grid method that help the clinician determine disease severity and the impact of the domain on the patients quality of life.
*Narrowband UVB light therapy can be very effective in clearing skin lesions. Bulbs with a narrow emission between 311 and 313 nm have been shown in studies to be superior to broadband UVB light. Treatment can be done in an outpatient setting or at home. Both small handheld devices are available as well as larger full body light units. UV light lamps designed specifically for psoriasis are more effective than commercial tanning beds or sunlight since they give of narrowband UVB light. Commercial tanning beds often give off much higher levels of UVA radiation that has been proven to be less effective in treating psoriasis unless combined with psoralen. Exact ratios of UVA and UVB are very difficult to determine with both sunlight and tanning beds. Generally light treatments should be done 2-3 times per week for a total of around twenty-five treatments. Skin will be exposed to UVB light from 20 seconds up to around 2 minutes during each treatment based on the Fitzpatrick skin type or minimal erythema dose. [6] www.dermaray.com/
Physical Therapy Management (current best evidence)[edit | edit source]
This patient should be referred to a rheumatologist immediately if undiagnosed psoriatic arthritis is suspected. All patients with manifestation of arthritic type conditions should be asked if they have any type of skin condition or patches of dry skin. They should also be encouraged to see a rheumatologist that can verify the type of arthritis that they have.
Physical therapy can play an important role in improving the life of a person with psoriatic arthritis. Physical therapy management should focus on education, improvement of range of motion, strengthening, and general cardiovasuclar conditioning. Physical therapists may also provide UV therapy and modalities to decrease pain. Cryotherapy may help to reduce swelling and tenderness in affected joints. Heat may be used to relieve joint pain. Paraffin baths tend to be soothing for the hands and feet. Aquatic therapy is a excellent choice for patients in advanced stages of psoriatic arthritis since it is easier on painful joints. Splinting may be of benefit to prevent deformity.
Recently studies have shown that hydrotherapy is an effective treatment for patients with psoriatic arthritis. Hydrotherapy has been shown to improve physical function, energy, sleep and relaxation, cognitive function, work and participation in patients with psoriatic arthritis.
Alternative/Holistic Management (current best evidence)[edit | edit source]
- Currently there is not much evidence to support alterantive therapies other than sunlight.
- Vacationing at the Dead Sea (balneotherapy or climatotherapy) is a popular holistic therapy for psoriatic arthritis and has been effective for some. The Dead Sea in Israel is 400 m below sea level. This allows for a higher concentraion of UVA rays, while UVB is blocked. Therefore, people can spend a longer time in the sun without burning. Salt concentration in the Dead Sea is ten times that of oceans. Minerals including magnesium, calcium, potassium, and bromine are also present in the water providing added benefit.[1]
 Dead Sea
Dead Sea - Healing Psoriasis: The Natural Alternative is a book written by John Pagano, a chiropractic physician, that describes a special diet to clear psoriasis. He developed this treatment with inspiration from the mystic Edgar Cayce. Central to the book is his theory that degenerative diseases are caused by leaky gut syndrome. Spinal adjustments, relaxation, and internal cleansing are also an important part of his program. The diet is extremely strict and difficult to follow. [7] www.psoriasis-healing.com/

Differential Diagnosis[edit | edit source]
- Osteoarthritis
- Rheumatoid Arthritis
- Reactive Arthritis
- Gaut
- Lupus
- Mallet finger due to traumatic injury
- Ankylosing spondylitis[8]
- fibromyalgia[8]

Resources[edit | edit source]
- National Psoriasis Foundation www.psoriasis.org/NetCommunity/Page.aspx
Case Reports[edit | edit source]
Recent Related Research (from Pubmed)[edit | edit source]
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 1.8 1.9 Langley R. Psoriasis: Everything You Need to Know. New York: Firefly Books; 2005.
- ↑ 2.0 2.1 Fuller KS. Pathology: Implications for the Physical Therapist. Third Edition. St.Louis: Saunders Elsevier; 2009.
- ↑ 3.0 3.1 3.2 Waldron N. Care and support of patients with psoriatic arthritis. Nursing Standard [serial online]. August 29, 2012;26(52):35-39. Available from: CINAHL with Full Text, Ipswich, MA. Accessed March 23, 2014.
- ↑ 4.0 4.1 4.2 Solivetti FM, et al. Role of contrast-enhanced ultrasound in early diagnosis of psoriatic arthritis. Dermatology 2010;220:25-31.
- ↑ Castelino M, Barton Anne. Genetic susceptibility factors for psoriatic arthritis. Curr Opin Rheumatol 2010;22:152-156.
- ↑ Menter A, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. Section 5. Guidelines of care for the treament of psoriasis with phototherapy and photochemotherapy. Journal of the American Academy of Dermatology. 2010;62(1):114-135.
- ↑ Pagano JOA. Healing Psoriasis. New Jersey: John Wiley & Sons; 2009.
- ↑ 8.0 8.1 8.2 Managing Patients with Psoriatic Disease: The Diagnosis and Pharmacologic Treatment of Psoriatic Arthritis in Patients with Psoriasis. Drugs [serial online]. March 15, 2014;74(4):423-441. Available from: CINAHL with Full Text, Ipswich, MA. Accessed March 23, 2014.

