Low Back Pain and Young Athletes
Introduction[edit | edit source]
8) Taking Part 2013/14 Annual Child Report
Low back pain (LBP) occurs in approximately 10% to 15% of young athletes[1] . Schmidt et al 2014 found that competitive adolescent athletes compared to aged matched individuals have increased prevalence of back pain
Injuries encountered to the lower back in young athletes occur from either an acute traumatic event or repetitive trauma (overuse injury) and are commonly seen in individuals participating in sports such as football, rugby, gymnastics, ice skating and dancing (Purcell and Micheli, 2009). Evidence has shown LBP occurs is as much as 27% of college football players and between 50% and 86% of gymnasts (Semon 1981; Kolt 1999). Overuse injury can be as a result of repeated flexion, extension and torsion which is performed frequently in gymnastics, ice skating and dancing (Purcell and Micheli, 2009).
There are significant differences between the nature of LBP in adults and young athletes.(Micheli and Wood, 1995). The most common causes of LBP in young athletes are spondylosis, spondylolisthesis, hyperlordosis syndrome and discogenic pain (Micheli and Wood, 1995).
The growing spine introduces certain variables that predisposes the back of the young to specific injuries such as pars interarticularis injury; reported to occur in up to 47% of young athletes (Micheli and Wood, 1995).
It is of great importance for an athlete with persisting symptoms to undergo a thorough assessment (Standaert, 2008)
The impact of the structural problems is considered alongside other aspects such as psychological, social and cultural issues (Purcell and Micheli, 2009). This approach facilitates compliance with the rehabilitation process and promotes recovery(Purcell and Micheli, 2009), as there is evidence showing athletes with a prior back injury are 3 times more likely to develop LBP (Greene, Cholewicki, Galloway et al., 2001).
Epidemiology
[edit | edit source]
Growth and Development of the Spine
[edit | edit source]
The vertebrae undergo gradual growth and development over the childhood and adolescence. This causes distinct structural differences of the spine from the adult spine, which affects the nature of injury in young athletes.
Development of the vertebrae[edit | edit source]
(Image)
Ossification of the vertebrae[edit | edit source]
Development of the vertebral column occurs in three stages: mesenchymal, chondrification, and ossification. There are two ossification stages:
- Primary - begins during ninth to tenth weeks in utero and finished by one year (Bogduk, 2005).
- Secondary - begins after puberty and ends at about age 25 (Pansky, 1982).
Primary Ossification:
(Image)
The vertebrae typically have three primary ossification centres (Schafer, 1986):
- The oval centrum
- One in each half of the cartilaginous neural arch
The three parts are united by hyaline cartilage. A cartilaginous ring develops around the anterior and lateral periphery of the centrum-disc interface, which firmly anchors the annulus to the centrum. The two halves of the arch ossify posteriorly by appositional growth (Schafer, 1986). The centrum joins the arch during 3-6 years old. In the lumbar region, ossification completes by age 8 (…).
Secondary ossification: (Image)
At puberty (age 13-16), five secondary ossification centres appear (Schafer, 1986; Williams and Warwich, 1980):
- One at the tip of the spinous process
- One at the tip of each transverse process (two in total)
- Cartilaginous mammillary processes (two in total)
Around the age of 25, union of secondary ossification centres with the rest of the vertebra is completed (Pansky, 1982).
Adolescent spines are more prone to pars defects/fractures due to the incomplete bony maturation present in the neural arch (Micheli and Wood, 1995). Biomechanical studies have indicated that the bone strength of the vertebrae especially the neural arch, can increase into the fourth or fifth decade of life (Cyron and Hutton, 1978
).
(Table of summary)
Growth of vertebral body[edit | edit source]
The physes associated with the vertebral end plates facilitate the growth of the vertebral body
Vertebral endplate are comprised of 2 parts: (Diagram)
- Hyaline cartilage (adjacent to the nucleus pulposus)
- Physeal cartilage (adjacent to the vertebral body)
(Luigi, 2009).
(Table)
The physes may be vulnerable during development. Fusion between ring apophysis and the adjacent vertebral body does not complete fully prior to the age of approximately 18–25 years. This increasing risk of apophyseal ring fractures in adolescents (Standaert, 2008).
(Diagram)
(Diagram)
Development of the intervertebral disc[edit | edit source]
Compared with the adult spine, nucleus pulposus in spine of children has a relatively greater hydrophilic nature, allowing more effective force absorption and central distribution of force transfer to the adjacent vertebrae. Due to the combination of central distribution of force, via the nucleus pulposus, and a weaker vertebral endplate, Schmorl nodes occur more frequently in children and adolescents compared to adults. Schmorl nodes are vertebral end-plate herniations of disc material. (Ferguson, 2006). The composition of the nucleus pulposus begins to change at 7-8 years old, resulting in a more peripheral force distribution of the disc (Standaert, 2008).
The relative strength of the intervertebral disc compared with that of the adjacent bone may also account for the relative reduction in rates of discogenic injuries seen in adolescents compared with adults.
Summary - Significance of developmental pattern of spine to injury[edit | edit source]
In summary, there are several aspects of the developmental pattern that are important in understanding injury to the young spine (...).
- The incomplete bony maturation present in the neural arch contributes to the occurrence of pars fractures in adolescents.
- The physes may be vulnerable during development, increasing risk of apophyseal ring fractures in adolescents.
- The more central distribution of force by way of the nucleus pulposus combined with a relatively weak vertebral end plate may account for the relatively high frequency of end plate herniations of disc material (Schmorl’s nodes) that occur in children and adolescents.
- The relative strength of the intervertebral disc compared with that of the adjacent bone may also account for the relative reduction in rates of discogenic injuries seen in adolescents compared with adults.
Risk Factors [edit | edit source]
Structural aspects of the growing spine[edit | edit source]
During adolescence injuries of the low back are prevalent due to the spinal column changing in structure and flexibility, the changes take place in the vertebral bodies and neural arch (Haus and Micheli, 2012) which are known as the growth ossification centres, one in the vertebral body and two in the vertebral arch (De Luigi, 2014).
Epiphyseal growth plates surround either end of the vertebral body and ring apophyses attach to the outer anulus fibrosis, there is risk of injury associated with these structures including herniation of the intervertebral disc through the ring apophyses caused by repetitive flexion, also injuries occurring to the ring apophyses can cause avulsion fractures (Purcell and Micheli, 2009).
The vertebral arch consists of the facet joints, spinous process and pars interarticularis (Purcell and Micheli, 2009). Failure in the fusion of these structures can lead development problems, such as spina bifida occulta, which if present at the lumosacral junction can increase the risk of spondylosis (Purcell and Micheli, 2009). The lack of fusion can also lead to Pars interarticularis fractures, which has been found to occur in 47% of young athletes (Micheli and Wood, 1995).
Variances in the adolescent spine development[edit | edit source]
Growth and maturation rates can differ in children of the same age, resulting in differences in size, strength and skeletal maturity (Purcell and Micheli, 2009).
The varied differences in size alongside other factors such as playing ability in young athletes can influence the impact of overload or excessive stress placed on spinal structures (Micheli, 1979).
Training[edit | edit source]
Young athletes participate in intense training programmes with repetitive practice which increases the likelihood of injury (Cassas and Cassettari- Wayhs, 2006) for example a gymnastic training programme can consist of up to 40 hours of training per week for elite gymnasts (Armstrong and Van Mechelen, 2008). This can cause overuse injuries and other musculoskeletal injuries (Emery, 2003).
As part of training a warm up is typically completed to reduce the risk of injury, lumbar flexibility is of importance for the lower back (Bono, 2004).
Intrinsic and extrinsic risk factors[edit | edit source]
Risk factors can be divided into two groups; intrinsic (i.e. age) or extrinsic (i.e. weather) (Emery, 2003). The intrinsic factors such as age and gender act as predisposing factors to injuries, extrinsic factors act from the outside which could influence injury risk, it is the combined effect of both of these categories that can make the individual vulnerable to injury (Meeuwisse, Tyreman, Hagel et al, 2007).
The effect of intrinsic and extrinsic factors in sporting injuries is illustrated in a model shown in figure 1 (Meeuwisse et al, 2007). It is the 'susceptible phase' of the model where the risks add together (Meeuwisse et al, 2007).
Figure 1- showing the model of risk factors in sporting injuries
Modifiable and non-modifiable risk factors[edit | edit source]
Risk factors can be further categorised into modifiable and non modifiable factors, modifiable factors are of importance as there is the possibility of being able to change them, for example training to improve flexibility and strength (Bahr and Holme, 2003). Non-modifiable factors are unchangeable but do influence the modifiable risk factors and therefore potential injury (Emery, 2003).
Table 2 summarises the most common factors for injury during sport: categorised according into intrinsic factors (modifiable and non-modifiable) and extrinsic factors (modifiable and non-modifiable). (Theisen, Malisoux, Seil, Urhausen, (2014) and Frisch, Croisier, Urhausen, Seil, Theisen, (2009).
Table - The potential risk factors for injury in sport
| Modifiable | Non-modifiable | |
| Intrinsic |
• Fitness level • Sport specific training/warm-up • Muscle strength • Flexibility • Joint stability • Biomechanical factors • Balance/proprioception • Psychological factors
|
• Gender • Age • Maturity level • Previous injury
|
| Extrinsic |
• Rules and regulations • Coaching education/training • Playing time • Playing surface • Equipment
|
• Type of sport • Sport context • Weather conditions • Level of play • Time of season • Playing position |
References:Theisen, Malisoux, Seil, Urhausen, (2014) and Frisch, Croisier, Urhausen, Seil, Theisen, (2009)
Additional risk factors[edit | edit source]
In a study by Nadler, Malanga, DePrince et al, 2000 the relationship between lower limb function and LBP was investigated in college athletes and showed athletes with reported LBP presented with a 5.8% greater difference between left and right extensor strength in the lower extremity compared with athletes without LBP. They conclude that it is clinically relevant in terms of screening athletes as part of preparation for participating in sport to minimise the occurrence of LBP and lower extremity injuries (Nadler et al, 2000).
Prevention[edit | edit source]
Recognising the risk factors is essential to reducing injury in sports, especially in young athletes.11 Here are some key aspects to consider when aiming to prevent injury.
Pre season
A preseason screening programme can indentify risk factors such as inflexibility, muscle weakness and previous injuries taht are not fully recovered. These risk factors should be identified and addressed before the start of the season.
Also athletes should start a general strength and fitness training several weeks
before the season begins, increasing in the frequency and intensity of training
gradually adapt to the high demands of the sport. 49 The training program, performance standards, and physical and psychological factors should be taken in to acccount Maffuli et al 2010.
For a prevention training program to prevent injuries their needs to be detailed understanding of the training content, frequency, duration, recovery and athlete compliance Frisch et al 2009 (SR).
Growth spurts
During periods of growth muscles struggle to lengthen as fast as bones grow, which can cause inflexibility and muscle imbalances predisposing them to injury.11,49 Due to this, young athletes should decrease the amount of training and of repetitive movements during growth spurts.
Technique and repetition
Specific movements in certain sports, such as walk overs in gymnastics and lay back spins in ice skating, put high amounts of pressure on the posterior spine that may lead to injury. Athletes may need to reduce the amount of repetitions of these movements, especially if their pain is associated with these movements.
Performing the correct techniques should be stressed to all athletes. Correcting posture to reduce excessive lordosis in the lumbar spine is important to help prevent injuries on the lumbar spine. Correct lifting techniques must be used to prevent damaging the back in sports that require lifting, such weight lifting and dancing.11
Exercises
Core stability exercises and stretching tight hip flexors and hamstrings can help reduce the risk of low back.
Competition
There can be a vast variability of sizes and strengths between players in team sports. Efforts should be made in contact sports to match athletes in strength and size in order to prevent injuries from contact with stronger and larger players.11,49
Early Intervention
It is important that athletes don’t associate back pain as being a part of their sport. Increasing complaints of pain should be addressed early and taken seriously to avoid significant injury, especially if the pain is interfering with activity. 11
Assessment[edit | edit source]
Subjective assessment[edit | edit source]
There is usually poorly localized lumbar pain without any associated neurologic symptoms.
Specific area of pain and neurologic symptoms are more likely to show an underlying pathology.
Knowing the onset of symptoms can help distinguish between acute or chronic overuse injury, and postural and developmental abnormalities.
The clinical history of a patient should include an in depth description of:
| Specific questions | |
| Pain |
Location |
| Trauma | Repetitive/overuse microtrauma Acute macrotrauma Specific movement of trauma Body positioning in trauma |
| Mechanical symptoms | Is the pain worse on movement? What specific movement? Does the pain cease during rest? |
| Inflammatory symptoms | Is there any morning stiffness? Does it get better with movement? |
| Neurological symptoms | Radiculopathy Pins and needles Bowel or bladder dysfunction Weakness |
| Systemic symptoms | Does the patient have a fever, night sweats or recent weight loss? |
| Gait | Does the patient suffer from foot drop |
| Previous Treatments | Has the patient had previous treatment for the same or similar condition? Was the treatment successful? |
| Lifestyle | Does the pain have any effect on their psychosocial well-being? Does it interfere with school or interests? |
| Past Medical History | Does the patient suffer from any medical conditions such neurological disorders, scoliosis, malignancy, osteoporosis, chronic inflammatory joint disease or has any treatment of immunosuppressive agents? Has the patient had any previous injury or surgery? |
| Family History |
Is there any of family history of orthopaedic, rheumatic or neurologic conditions? |
Objective assessment[edit | edit source]
Observation[edit | edit source]
Observation begins as soons as you see the patient. The examiner should observe the patients gait and posture as they walk in and note down any abnormalities. To observe the patients posture in more detail it is best appreciated if the examiner is able to see specific bony land marks and areas on the patients back.
Standing Posture
Anterior/Posterior view
- Both Shoulders should be level
- Both anterior superior iliac spines (ASIS) and posterior superior iliac spines should be level
- Symmetry of soft tissue and bony landmarks either side of the midline
Lateral view
- Foot arch cavus/planus?
- There should be a gentle cervical lordosis, thoracic kyphosis and lumbar lordosis (excess lumbar lordosis may be caused by weak abdominal muscles or a hip flexion contracture)
Palpation[edit | edit source]
(IMAGES)
It is best appreciated palpating the posterior spine with the patient in a standing position. Any point of severe tenderness should be related with the underlying soft tissue anatomy or bone. Useful places to palpate over are the facet joints, spinous processes, paraspinal muscles, sacroiliac joints, posterior iliac crest, PSIS, gluteals, greater trochanters and ischial tuberosities.
Range of movement[edit | edit source]
To test active movements of the thoracolumbar spine patients need to be in a standing position with their pelvis stabilised. Here are some examples how to measure the range movement in the thoracolumbar spine (IMAGES)
Flexion
Ask the patient to bend forward and try to touch their toes with their knees straight (measure the distance from their fingertips to the floor).
Extension
Ask the patient to bend as far backward as possible with knees straight, whilst supporting their lumbar spine (measure the degrees of movement).
Lateral flexion
Ask the patient to bend as far to the side as possible (the patient should be able to touch their fibular head).
Rotation
As well as stabilising the pelvis, place a hand on the opposite shoulder to prevent compensatory movements. Ask the patient to rotate their trunk as far as possible (measure the degrees of movement).
Hamstring length
Tight hamstrings or asymmetry between hamstring lengths is common in in having low back pain.
To examine a patients hamstring flexibility the examiner will measure their popliteal angle. This is done with the patient in supine with their hips and knees flexed to 90 degrees. The examiner will then extend the knee until there is a large resistance. The angle is measured between femur and tibia at the joint line of the knee between. An angle larger than 45 degrees may be a factor to having low back pain. The patients back and hip range of movement should be measured passively and activily. By the measuring the patients popliteal angle it determines their hamstring flexibility.
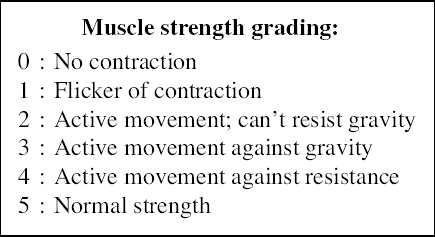
Strength[edit | edit source]
The patients core and lower limb strength should be examined. Lower limb strength can be measured using the MRC scale.
flylib.com/books/2/426/1/html/2/weakness_files/da1cweaknessff14.png
Neurological exam[edit | edit source]
A neurological exam should include trunk and lower limb sensation, strength, and deep tendon reflexes to investigate whether there is any neural involvement in the low back pain.
Dermatomes
(IMAGE)
Myotomes
(IMAGE)
Deep tendon reflex tests
Patellar (L2, 3, 4),
Achilles (S1)
.(IMAGE) or (VIDEO)
Special tests[edit | edit source]
- Scoliosis test (Adams Forward Bend Test)
- Modified Schober’s test
- Straight leg raise
- FABER or Patrick test
- Trendelenburg Test
Abdominal, pelvic and hip exam[edit | edit source]
Back pain can be referred from abdomen, pelvic or hip pathologies and injuries, so it is important to rule out all of these before carrying on with any treatment.
Further investigations[edit | edit source]
Laboratory tests[edit | edit source]
It is necessary to perform laboratory tests to investigate patients with back pain and high suspicion of systemic disease or infection. If an infection is suspected CBC, ESR or CRP, blood and joint cultures should be screened.
If arthritis is suspected rheumatoid factor, HLA-B27 and ANA can be investigated to help classification and decide treatment, but these results will help diagnosis.
If a hematological malignancy is suspected a peripheral blood smear (CBC) should be investigated.
Imaging[edit | edit source]
Radiographs
Radiographs can be used to detect fractured vertebrae and herniated discs
Technetium bone scan
A bone scan detects regions of increased osteoblastic activity and can help locate specific areas of bone injury that may not be visible on radiographs.
SPECT (singlephoton emission computed tomography) is useful in identifying stress fractures and spondylolysis [8].
Bhatia, N. N., Chow, G., Timon, S. J., & Watts, H. G. (2008). Diagnostic modalities for the evaluation of pediatric back pain: a prospective study. Journal of Pediatric Orthopaedics, 28(2), 230-233.
Computed (CT)
CTs provide a detailed image of bone and cartilage. A CT scan is useful for further investigation into lesions that are identified on a bone scan, including spondylolysis, fractures and tumors [11].
Rodriguez, D. P., & Poussaint, T. Y. (2010). Imaging of back pain in children. American Journal of Neuroradiology, 31(5), 787-802.
Magnetic resonance imaging (MRI)
MRI provides an detailed image of contrasts of soft tissue which allows evaluation of paraspinal structures and the spinal cord. MRI is useful for neurologic findings but it is necessary to compare and agree with clinical examination results to increase the specificity of imaging
Specific Conditions[edit | edit source]
Spondylolysis and Spondylolisthesis[edit | edit source]
Links to relevant Physiopedia pages:
http://www.physio-pedia.com/Spondylolysis
http://www.physio-pedia.com/Lumbosacral_spondylolysis
Posterior Element Overuse Syndrome[edit | edit source]
Vertebral Body Apophyseal Avulsion Fracture[edit | edit source]
Disc Herniation[edit | edit source]
Scheuermann's Kyphosis [edit | edit source]
Link to relevant physiopedia page:
http://www.physio-pedia.com/Scheuermann's_Kyphosis
Treatment[edit | edit source]
Return to sports[edit | edit source]
Back pain is associated with time lost playing sports among competitive athletes (Bono, 2004).The duration of the athletes treatment time off can be an indication of the severity of the injury and sporting time lost can impact upon the sports person in several ways such as mental well-being therefore it is important that the athlete returns to sport as soon as possible (Armstrong and Van Mechelen, 2008).
Return to sport following an injury is deemed appropriate after a period of rehabilitation for the specific condition which includes education regarding spinal awareness and dynamic postural control (De Luigi, 2014).
A criterion for return to play consists of normal strength and pain-free range of motion (Purcell and Micheli, 2009).
Table- overview of time scales for return to play for specific conditions common in the young athlete
References[edit | edit source]
- ↑ d’Hemecourt PA, Gerbino PG II, Micheli LJ. Back injuries in the young athlete.fckLRClin Sports Med; 2000:19:663–79.


{kind=link}