Back Education Program
Original Editors - Hannah Anderson, Dan McCoy, Rebecca Porter and Millie Ware
Top Contributors - Rebecca Porter, Hannah Anderson, Elaine Lonnemann, Laura Ritchie, Millie Deason, Kim Jackson, Daniel McCoy, Admin, Evan Thomas, Shreya Pavaskar, Kalyani Yajnanarayan, WikiSysop, Vidya Acharya and Lucinda hampton
|
An Evidence-Informed Back Education Program |
|---|
About Low Back Pain [edit | edit source]
Are you experiencing low back pain? You are not alone! Look at these statistics...[1]
- As many as 80% of Americans have symptoms of low back pain during their lifetime[2]
- Low back pain is the leading cause of injury and disability for those younger than 45 years old[2]
- Each year, approximately $26 billion dollars are spent in the United States for the treatment of low back pain[3]

Is pain always bad? No. Pain is a warning sign to our body that something is not physiologically correct. We feel pain when there is structural damage, sign of an infection, a previous structure has been reinjured, etc. Pain is a helpful indicator for us to get treatment to heal our bodies.
Before you are able to truly understand back pain, it is important to know your body's anatomy.[4]
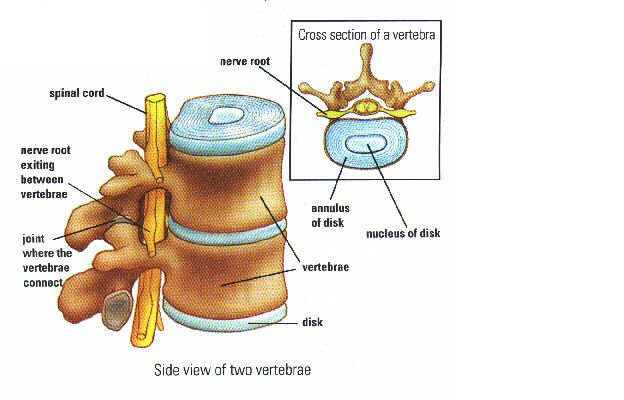
Your spine is made up of 33 small bones called vertebrae. Together, they form what is know as the vertebral column. There are 7 vertebrae in the cervical region which is your neck; 12 vertebrae in the thoracic region which is your upper back; 5 vertebrae in your lumbar spine which is your lower back; and 5 sacral vertebrae and 4 coccyx which are located below that.
Between each of the vertebrae is a disc that acts as a cushion and a shock absorber. These intervertebral discs are made up of two parts-- the nucleus pulposis and the annulus fibrosis. The nucleus pulposis is in the middle of the disc and is jelly-like due to its large water content; it is composed of up to 80% water! The annulus fibrosis surrounds this nucleus and so forms the outer part of the disc. These discs play an important role in keeping the back healthy! For more information on these discs, go to section Why Does My Back Hurt.
Other important parts of the spine:
- Facet: the joint where the vertebrae connect
- Spinal cord
- Nerves: diverge off of the spinal cord and run to different parts of the body

Your spine has three natural curves that begin to develop from the moment a baby lifts his/her head and gravity begins to work on the body. The curves keep the spine from being completely rigid and help the spine to tolerate a little bit more compression. To understand the normal curves of a spine, there are 2 terms you need to know—lordosis and kyphosis. Lordosis is when the spine curves inward and a kyphosis is when the spine curves outward. The cervical portion of the spine is in a lordosis, the thoracic portion is in a kyphosis, and the lumbar spine is in a lordosis. These nice curves of the back increase the load bearing capacity of the spine.

The spine has 4 main motions—forward bending, backward bending, sidebending, and rotation. These motions can also be coupled. For instance, you can have forward bending with rotation or backward bending with sidebending. Below, we demonstrate these motions and report typical lumbar spine active range of motion.
'Forward bending (flexion): 60 degrees '[2]

Backward bending (extension): 25 degrees[2]

Lateral flexion (sidebending): 25 degrees to each side[2]

Rotation: 30 degrees to each side[2]

An example of coupled motion: Forward bending with coupled rotation

Muscles:
Many muscles work together to help make these spinal motions possible! These back muscles can be classified into three different layers-- superficial, intermediate, and deep.[5]
Superficial Layer:
| Muscle | Origin | Insertion | Action |
| Trapezius | Medial 1/3 of nuchal line; external occipital protuberance; nuchal ligament; C7-T12 spinous processes | Lateral third of clavicle; acromion; spine of scapula | Upper fibers: scapular elevation; Lower fibers: scapular depression; middle fibers: scapular retraction |
| Latissimus dorsi | T6-T12 spinous processes; thoracolumbar fascia; iliac crest; inferior ribs | Intertubercular sulcus of humerus | Extends, adducts, and medially rotates humerus, shoulder girdle depression |
| Rhomboid major | T2-T5 spinous processes | Medial border of scapula from base of the spine to inferior angle | Scapular elevation and inferior rotation; stabilizes scapula to thoracic wall |
| Rhomboid minor | Nuchal ligament and C7-T1 spinous processes | Base of scapular spine | Scapular elevation and inferior rotation; stabilizes scapula to thoracic wall |
| Levator scapulae | C1-C4 transverse process, posterior tubercles | Medial border of scapula superior to base of spine |
Elevation and downward rotation of scapula |
Intermediate Layer:
| Muscle | Origin | Insertion | Action |
| Serratus posterior inferior | T11-12 spinous processes | Inferior borders of 8th-12th ribs near the angle | Elevate ribs |
| Serratus posterior superior | Nuchal ligament and C7-T3 spinous process | Superior borders ribs 2-4 | Elevate ribs |
For the deep layer, the following acronym helps to remember the muscles: I Love Spaghetti Says Mama Ragu. The Iliocostalis, Longissiums, and Spinalis muscles make up what is known as the erector spinae. The Semisplinalis, Multifidus, and Rotatores together make up the transversospinalsi muscles.
Deep Layer:
| Muscle | Origin | Insertion | Action |
| Iliocostalis (I) | From common tendon from posterior iliac crest, sacrum, SI ligaments, spinous processes, and supraspinous ligaments | Angle of lower ribs and cervical transverse processes | Acting together with the other erector spinae muscles, extend the trunk and neck; acting alone laterally flex the trunk toward side of activity |
| Longissimus (Love) | Same as above | Ribs between the angle and tubercle; thoracic and cervical transverse process and mastoid process | Same as above |
| Spinalis (Spaghetti) | Same as above | Spinous processes and cranium | Same as above |
| Semispinalis (Says) | C4-T10 transverse processes | Occiput; cervical upper thoracic spinous process; spans 4-6 ligaments | Acting together with the other transversospinalis muscles, extends head, cervical, and thoracic spine; acting along rotates away from activity |
| Multifidus (Mama) | Spinous processes 2-4 segments above lateral attachment | Sacrum; ilium; thoracic and lumbar transverse processes | Vertebral stablization |
| Rotatores (Ragu) | From thoracic vertebra transverse processes | Lamina and transverse process or spinous process junction; 1-2 segments above proximal attachment | Segmental stabilization |
About Neck Pain[6][edit | edit source]
How common is neck pain? Here are a few statistics on its prevalance:
- Neck pain reported to be 2nd most common musculskeletal disorder that leads to disability and injury claims[2]
- 2002: 13.8% of population > 18 years old in U.S. reported neck pain[2]
Anatomy of the neck:
Just as with low back pain, it is important to understand the anatomy behind your neck pain! The neck is anatomically separated into the upper cervical spine and the lower cervical spine. There are 7 vertebrae that make up the cervical spine.
The first cervical vertebra (C1) is called the Atlas. It has no vertebral body or spinous process. This vertebra articulates with the occiput, which is the base of the skull. This articulation is labeled as the OA joint; its primary motion is flexion and extension at the joint. It also performing sidebending with opposite rotation.
The second cervical vertebra (C2) is called the Axis; it has a large spinous process. The articulation between the Atlas and Axis is called the AA joint and its primary motion is rotation.

The following pictures demonstrate the motions of the lower cervical spine (C3-C7) and report the typical active range of motion.[2]
Flexion: 54 degrees Extension: 77 degrees (pic)


Left Sidebending: 41 degrees/Right Sidebending: 45 degrees

Left Rotation: 69 degrees/Right rotation: 69 degrees

Coupled motion -- Sidebending with ipsilateral rotation

Non-coupled motion -- Sidebending with contralateral rotation

Muscles:
The muscle mentioned in the section About Back Pain also can play a role in neck pain, especially those muscles of the superficial layer. Also, deep inside the back of the neck are four important muscles called the suboccipital muscles.[5]
| Muscles | Origin | Insertion | Action |
| Rectus capitus posterior major | C1 spinous process | Lateral part of inferior nuchal line | extend occiput (head) on C1; rotate C1 on C2 |
| Rectus capitus posterior minor | C1 posterior tubercle | Medial part of inferior nuchal line | same as above |
| Obliquus capitus superior | C1 transverse process | occiput | same as above |
| Obliquus capitus superior | C2 spinous process | C1 transverse process | same as above |
There are certain factors that can put you at risk for neck pain. See if any of these describe you:
- Working at a desk that is ill fitting to your body
- Working at a computer for long periods of time
- Sitting with bad posture for long periods of time
- Working on above head activities (i.e. painting) for long periods of time
For Physical Therapists: What information should you be collecting when treating a patient with neck pain? The following classification system will lead you you to a treament a patient would benefit from.
Neck Classifications [2]
Cervical Hypomobility
- Loss of ROM/flexibility
- No symptoms beyond the shoulder
- Sudden onset- sudden awkward movements can theoretically cause entrapment of the facet joint meniscus
- Gradual onset- joint stiffness can come from osteoarthritic changes, adaptive shortening of connective tissues, or adhesions after trauma to spinal segments
Cervical Radiculopathy
- Disorder of the spinal nerve root caused by disc herniation or other space-occupying lesion (i.e. spondolytic spurs or cervical osteophytes)
- Usually present with pain in the neck and in one arm, loss of motor function, or reflex changes in affect nerve root distribution
- Most common cause is foraminal encroachment of the spinal nerve secondary to decreasing disc height and degenerative changes to the uncovertebral and facet joints
Cervical Instability
- Remote history of trauma
- Symptoms occur with sustained weight-bearing posture and relieve from non-weight bearing position
- Hypermobility with lose end feels
- Poor strength of deep cervical muscles
- Aberrant movement with AROM
Acute Pain (whiplash)
- Recent history of trauma
- Referred symptoms into upper quarter
- Poor tolerance to most interventions
- High pain a disability scores
Cervicogenic Headache
- Unilateral headache with onset proceeded by neck pain
- Triggered by neck movements or positions
- Pain elected by pressure on posterior neck especially at upper cervical joints
Why Does My Back hurt?
[edit | edit source]
Back pain is becoming increasingly prevelent in our population. Pain is an indication that your body is working to protect that part of the body. Pain can be a good guide to the best healing behaviors; understanding pain can help you to deal with it effectively.[7] Back pain can be caused by a multitude of structures, but most cases are not identified-85%. Back pain can come from the disc, facet joint, nerve root, muscles, bones, fascia, or neurogenic claudication. The intervertebral disc usually has no nerve supply inside, but the oustide has some innervation.
Musculoskeletal causes of back pain
- Facet: 15-40% depending on the author
- Disc: 39%
- SIJ: 13%
- Undefined: 33%
- Instability in the spine is also a cause of back pain
Pain sensitive structures around the disc that can cause pain
- Muscles
- Anterior longitudinal ligament
- Posterior longitudinal ligament
- Vertebral body
- Nerve root
- Cartilage of facet joint
Intervertebral Disc:
The natural lordotic posture decreases the pressure on the disc compared to the straight posture which can put pressure on the disc and can push fluid from the nucleus pulposis into the vertebral body (schmorl’s nodes). It is important to differentiate herniated disc (space occupying) which refers into the leg vs other conditions (inflammation reaction, spasms, strains, facet syndrome) which are more localized in pain.
Functional anatomy of the intervertebral disc:[8]
- In forward bending or flexion, the disc bulges anteriorly/forwards and the nucleus pulposis goes posteriorly
- In backward bending or extension, the disc bulges posteriorly/backwards and the nucleus pulposis goes anteriorly
- In sidebending or lateral flexion, the disco bulges towards the side in which in movement is occurring (eg. right sidebending, right disc bulge)
- If the disc looses height, can put pressure on the facet joints, possibly increasing the risk of arthritis, and put pressure the nerve roots by decreasing the foraminal height
Injury to the disc:
- Protrusion: disc bulge posteriorly without rupture of annulus fibrosis
- Prolapse: outermost fibers of the annulus fibrosis contain the nucleus
- Extrusion: annulus fibrosis is perforated and discal material into the epidural space
- Sequestrated: fragments of annulus and nucleus are outside the disc proper (can lead to pressure on neurological tissues and cause an inflammatory response)
Anterior disc herniation:[8]
- Occurs when someone is in extension, or leaning backward, which puts pressure on the anterior/front of the disc causing it to herniated/prolapse/bulge.
- This can put pressure on nerves in the lower abdomen causing weakness or numbess, anterior longitudinal ligament, vertebral body, and transverse abdominus which can all cause pain.
Posterior disc herniation:[8]
- Occurs when some is in flexion, leaning forward, which puts pressure on the posterior/back of the disc causing it to herniate/prolapse/bulge.
- This can put pressure on your spinal cord or nerve root causing pain/weakness/numbness/reduced reflexes and the posterior longitudinal ligament causing pain
For Physical Therapists: What information should you be collecting when treating a patient with low back pain? The following classification system will lead you to a treatment patients will benefit from[2]
Lumbar and leg pain that centralizes with repeated movements
Extension syndrome:
- Symptoms centralize with extension
- Peripheralize with flexion
Flexion syndrome:
- Symptoms centralize with flexion
- Peripheralize with extension
Lateral shift:
- Visible frontal plane deviation of the shoulders relative to the pelvis
- Centralize with side glide and backward bending
Lumbar hypomobility:
- Hypomobility with passive intervertebral motion
- Does not travel below knee (manipulation)
Lumbopelvic instability:
- Hypermobility with posterior-anterior segmental mobility testing
- Positive prone instability test
Postpartum Instability:
- Positive pelvic pain provocation
- Positive ASLR
- Positive modified Tendelenburg's test
- Pain with palpation of pubic symphysis or sacroiliac ligament
Lumbar radiculopathy that does not centralize with movement:
- Traction, symptoms are alleviated
- No lumbar movement centralizes pain
- No directional preference in subjective or objective to alleviate leg pain
- Peripheralize leg pain with backward bending
- Positive SLR >45 degrees for lower leg pain
- Positive crossed SLR <45 degrees
- Lower extremity neurologic signs poor tolerance to weight-bearing postures
RED FLAGS for the Lumbar Spine
Immediate referral
- AAA
- Bowel or bladder weakness
Physician follow up but not immediate referral
- Unexplained weight loss
- Non-healing sores
Requires further physical testing
- Unexplained weakness
- Unexplained referred pain
What can I do about my Low Back Pain?[edit | edit source]
Treatment may include:
Proper posture
Aerobic conditioning
Traction
Manual therapy (mobilizations, stretching)
Self-stretching
Exercise
For Physical Therapists: Stanton et. al created a treatment based classification based system for low back pain.[9]
Manipulation and Mobilization Category [10] [11]
Subjective:
- Symptoms < 16 days
- Symptoms not below knee
- Not afraid to work (FABQ < 19)
Objective:
- Lumbar hypomobility
- Hip internal rotation > 35 degrees for at least one hip
Traction Category [12]
Subjective:
- Symptoms distal to buttocks
Objective:
- Pain peripheralizes with a specific movement (can be flexion or extension)
- (+) Crossed straight leg raise
A licensed Physical Therapist is able to perform manual therapy/mobilizations and traction. Please contact a Physical Therapist near you if these exercises and proper movement techniques do not help resolve your pain and discomfort.
- Find a PT on the APTA website: [http://www.apta.org/apta/findapt/index.aspx?navID=10737422525 http://www.apta.org/apta/findapt/index.aspx?navID=10737422525
Stabilization Category [13] [11]
Subjective:
- Age < 40 degrees
Objective:
- Average straight leg raise > 90 degrees
- Abberant movement present
- (+) prone instability test
Which exercises does research show to be effective for lumbopelvic stabilization? [13]
Exercise is a significant factor in the rehabiliation process. Studies have found that exercise is more effective at improving function and decreasing pain than seeing a family physician. [14] Goal of exercises: to restore strength and endurance of the transverse abdominis and lumbar multifidus.
Abdominal bracing
- Abdominal bracing with heel slides


- Abdominal bracing with leg lifts

- Abdominal bracing with bridges

- Abdominal bracing with standing row exercise

- Abdominal bracing with walking/standing
Erector Spinae/Multifidus
- Quadruped arm lifts and bracing

- Quadruped leg lifts and bracing

- Quadruped alternate arms and legs with bracing

Specific Exercise Category [11] [15]
Subjective:
- Symptoms distal to buttocks
Objective:
- Pain centralizes with a specific movement (can be flexion or extension)
Aerobic Activity[16]
Types: Walking, jogging, running, cycling, swimming, climbers, steppers, elliptical machines, ski machines, aerobic dance
Warm up/cool down – low to moderate activity
- 5-10 minutes of warm up (adjust to demands placed on the body)
- 5-10 minutes of cool down (recovery of heart rate and BP)
- 10 minutes of stretching AFTER the warm up OR cool down
ACSM Guidelines:
- Frequency: 5 days/week
- Duration: 150 minutes per week (minimum)
- Intensity: 40-60% HRmax (HRmax = 220-age)
Benefits of exercise are improved joint health due to low impact exercises, increase bone density due to weight bearing exercises, improving energy, reducing health risks, improving circulation, and reducing stress and improving your mood. Aerobic activity is equally effective at reconditioning muscles as exercise and can also help in decreasing pain, improving your mood, and improving your functional capabilities.[17] Lack of exercise increases your risk of obesity and other co-morbidities increases; this can lead to increased pressure on the spine and decreased flexibility.
What can I do about my Neck Pain?[edit | edit source]
There are specific treatments based on each classification of neck pain: [2]
Cervical Hypomobility
- AROM exercises
- Cervical and thoracic mobilization/manipulation isometric or thrust manipulation techniques
- Nonthrust manipulation
Cervical Radicuopathy
- Cervical traction (manual/mechanical)
- ULNT 1 AROM
- Thoracic spine manipulation
- Postural exercises
Cervical Instability
- Postural education
- Cervical stabilization exercise program
- Mobilization/manipulation above and below hypermobilities
- Ergonomic corrections
Acute Pain (Whiplash)
- Gentle AROM within patient tolerance
- Activity modification to control pain
- Relative rest
- Physical modalities
- Intermittent use of cervical collar
- Gentle manual therapy and exercises, but avoidance of pain-inducing manual therapy techniques or exercises
Cervicogenic Headache
- Cervical and thoracic mobilization/manipulation
- Strengthening neck and postural muscles
- Postural education
What does the literature say about neck pain?
Exercise!
Evidence from the literature says that exercise has a significant effect in reducing chronic non-specific neck pain for short term (<1 month) and intermediate term (1-6 months) [18]
Neck Exercises:
- OA flexion (chin tuck): A slight nod while keeping your head in neutral


- Flexion with chin tuck: While lying on your back tuck in your chin, lift off until your head clears the table and hold for 3-5 seconds maintaining the chin tuck

- Extension with chin tuck: While laying on your s tomach tuck your chin, lift your head off table while maintaining chin tuck and hold 3-5 seconds
- 4-way Isometrics: Lightly press into your hand in flexion, extension, side bending, and rotation




Exercises for Scapular Stabilizers (muscles attached to your shoulder blade)
- Middle Trapezius: With band or lying on stomach, Thumb pointing in the direction exercise is moving, Pinch shoulder blades

- Lower Trapezius: Lying down making a half Y bring your shoulder blade back and down

- Seated Row: Upright Sitting Posture, Pull at elbows, Pinch shoulder blades together

- External Rotation: Elbows at sides, Thumbs pointing out, Shoulders back, Rotate outward


- Scapular Clock: Turn shoulder blade into a clock, Move shoulder blade to each number, retraction and depression are critical, Numbers 9, 8, 7, 6 are important

Stretches:
Seatbelt Stretch
- Trapezius/Sternocleidomastoid

- Scalenes

- Levator Scapulae

Don't forget the thoracic spine! A clinical prediction rule was developed to help classify patients with mechanical neck pain that will experience early success from thoracic spine manipulation. Six variables were found: [19]
1. Symptoms < 30 days
2. No symptoms distal to the shoulder
3. Looking up does not aggravate symptoms
4. FABQPA score < 12
5. Diminished upper thoracic spine kyphosis
6. Cervical extension < 30 degrees
If a patient demonstrates 3 of the 6 variables the chance of experiencing a successful outcome improves from 54% to 86%. If a patient has 4 of the 6 variables the chance of a successful outcome rises to 95%.
Resources
[edit | edit source]
Chou, MD Lumbar imaging guidelines
APTA Low Back Pain Infographic
Find a PT on the American Physical Therapy Association website
Orthopaedic Section - APTA: Clinical Guidlines for Neck Pain
Orthopaedic Section - APTA: Clinical Guidlines for Low Back Pain
Recent Related Research (from Pubmed)[edit | edit source]
<div class="researchbox"><rss>Feed goes here!!|charset=UTF-8|short|max=10</rss></div>
References[edit | edit source]
- ↑ Cynergy Physical Therapy. Back Pain. http://www.cynergypt.com (assessed September 23 2013).
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 Olson, KA. Manual Physical Therapy of the Spine. St. Louis, MO: Saunders; 2009.
- ↑ Hebert J, Koppenhaver S, Walker B. Subgrouping Patients with Low Back Pain: A Treatment-Based Approach to Classification. Sports Health. 2011; 3:534-542.
- ↑ Physicians Plus.Vertebrae. http://www.physiciansplus.net (accessed September 16 2013).
- ↑ 5.0 5.1 Tank P. Grant's Dissector. 15th ed. Little Rock, AR: Wolters Kluwer; 2013.
- ↑ Ahern Family Chiropractic. Seizures. http://ahernfamilychiro.com (accessed September 24 2013).
- ↑ Butler D, Moseley. Explain Pain. Adelaide City Way, SA: Noigroup Publications; 2003.
- ↑ 8.0 8.1 8.2 Neumann, DA. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation 2nd Edition. St. Louis, MO: Mosby Inc; 2010.
- ↑ Stanton T et al. Evaluation of a Treatment-Based Classication Algorithm for Low Back Pain: A Cross-Sectional Study. Physical Therapy. 2011; 91:496-509.
- ↑ Childs et al. A Clinical Prediction Rule to Identify Patients with Low Back Pain Most Likely from Spinal Manipulation: A Validation Study. Annals of Internal Medicine. 2004; 141: 920-928.
- ↑ 11.0 11.1 11.2 Brennan et al. Identifying Subgroups of Patients with Acute/Subacute "Nonspecific" Low Back Pain Spine. 2006; 31:623-631.
- ↑ Fritz et al. Is There a Subgroup of Patients with Low Back Pain Likely to Benefit From Mechanical Traction? Spine. 2007; 32:793-800.
- ↑ 13.0 13.1 Hicks et al. Preliminary Development of a Clinical Prediction Rule for Determining Which Patients with Low Back Pain Will Respond to a Stabilization Exercise Program. Arch Phys Med Rehabil. 2005; 86: 1753-1762.
- ↑ Hettinga et al. A systematic review and synthesis of higher quality evidence of the effectiveness of exercise interventions for non-specific low back pain of at least 6 weeks' duration. Physical Therapy Reviews [serial online]. September 2007;12(3):221-232. Available from: CINAHL with Full Text, Ipswich, MA. Accessed October 6, 2013.
- ↑ Browder D, Childs J, Cleland J, Fritz J. Effectiveness of an Extension-Oriented Treatment Approach in a Subgroup of Subjects with Low Back Pain: A Randomized Clinical Trial. Physical Therapy. 2007; 87: 1608-1617.
- ↑ Thompson WR, Gordon NF, Pescatello LS, eds. ACSM's Guidelines for Exercise Testing and Prescription. 8th ed. Baltimore: American College of Sports Medicine; 2010.
- ↑ Hettinga D, Jackson A, Moffett J, May S, Mercer C, Woby S. A systematic review and synthesis of higher quality evidence of the effectiveness of exercise interventions for non-specific low back pain of at least 6 weeks' duration. Physical Therapy Reviews [serial online]. September 2007;12(3):221-232. Available from: CINAHL with Full Text, Ipswich, MA. Accessed October 6, 2013.
- ↑ Bertozzi et. al. Effect of Therapeutic Exercise on Pain and Disability in the Management of Chronic Nonspecific Neck Pain: Systematic Review and Meta-Analysis of Randomized Trials. Phys Ther. 2013; 93:1026-1036
- ↑ Cleland et al. Development of a Clinical Prediction Rule for Guiding Treatment of a Subgroup of Patients with Neck Pain: Use of Thoracic Spine Manipulation, Exercise, and Patient Education. Phys Ther. 2007; 87: 9-23.

