Midcarpal Instability: Difference between revisions
Kim Jackson (talk | contribs) No edit summary |
Kim Jackson (talk | contribs) No edit summary |
||
| (5 intermediate revisions by the same user not shown) | |||
| Line 4: | Line 4: | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
</div> | </div> | ||
== Definition/Description == | == Definition/Description == | ||
Midcarpal Instability (MCI) is | Midcarpal Instability (MCI) is a condition affecting the [[Wrist and Hand|wrist joint]]. It manifests as increased, abnormal mobility between the proximal and distal rows of the carpal bones. Common symptoms include persistent wrist pain, clicking, and limited functional capacity. The instability stems from lack of support of the proximal carpal row by ligamentous structures, as well as a disruption of normal joint forces between proximal and distal carpal rows. Palmar midcarpal instability is more prevalent, but dorsal and extrinsic variants also exist.<ref name=":0">Lichtman DM, Wroten ES. Understanding Midcarpal Instability. Journal of Hand Surgery [AM]. 2006; 31A:491–498</ref><br><br> | ||
== Clinically Relevant Anatomy == | == Clinically Relevant Anatomy == | ||
The | The wrist is composed of eight carpal bones arranged in two rows. The proximal row includes the [[scaphoid]], [[lunate]], and [[triquetrum]]. The distal row consists of the [[trapezium]], [[trapezoid]], [[capitate]], and [[hamate]]. Ligaments connect these bones, stabilising the joint. | ||
== | <div class="row"> | ||
<div class="col-md-6"> [[File:Ligaments of the hand dorsal aspect Primal.png|frameless]]</div> | |||
<div class="col-md-6"> [[File:Ligaments of the hand palmar aspect Primal.png|frameless]]</div> | |||
</div> | |||
Key to the stability of the midcarpal joint is the arcuate ligament complex. This complex has two parts: an ulnar part, comprised of the triquetrohamatecapitate ligament, and a radial part that extends distally from the radioscaphocapitate ligament. Another important stabilising element for the proximal carpal row is the dorsal radiolunotriquetral ligament. | |||
== Epidemiology /Aetiology == | |||
Midcarpal instability is an uncommon condition but is more frequently seen in younger adults and athletes.<ref name=":3">Jing SS, Smith G, Deshmukh S. Demystifying palmar midcarpal instability. Journal of Wrist Surgery. 2020 Aug 27;10(02):094-101.</ref> It often results from factors such as ligament laxity, trauma, or repetitive strain on the wrist. Two main forms, congenital and acquired, exist.<ref name=":3" /> The acquired form is commonly linked with wrist trauma or repetitive stress, and certain systemic conditions like rheumatoid arthritis may also contribute. The types of instability are: | |||
* Palmar Midcarpal Instability (PMC): This subtype is primarily caused by laxity in specific ligaments, namely the ulnar component of the arcuate ligament and the dorsal radiolunotriquetral ligament. These ligament issues result in abnormal movement in the carpal rows, leading to a condition known as a flexion deformity. The deformity disrupts the normal rotational coupling of the carpal bones, leading to the "catch-up clunk" sound during extreme ulnar deviation.<ref name=":0" /><ref name=":1">Buchler U. Wrist instability. Ln: Gaenslen ES, Lichtman DM. Midcarpal instability: description, classification, and treatment. First ed. UK; The livery house, 1996. pg 163-168</ref>Notably, up to 70% of Ehlers–Danlos syndrome patients, particularly those with the hypermobility type, experience painful midcarpal laxity. However, this instability often tightens up over time, making it self-limiting in these patients.<ref>Niacaris T, Ming BW, Lichtman DM. Midcarpal instability: a comprehensive review and update. Hand Clin 2015;31(03):487–493</ref><ref>1 Woerdeman LAE, Ritt MJPF, Meijer B, Maas M. Wrist problems in patients with Ehlers-Danlos syndrome. Eur J Plast Surg 2000; 23:208–210</ref> | |||
* Dorsal Midcarpal Instability: Laxity in the palmar radioscapocapitate ligament results in dorsal subluxation of the midcarpal joint. This creates a unique "subluxation clunk" sound. | |||
* Extrinsic Midcarpal Instability: This form is usually secondary to distal radius malunions that result in malalignment. This causes a dorsal displacement of the distal radius and an adaptive Z-deformity in the carpal bones.<ref>Stoller DW. Midcarpal instabilities. Magnetic resonance imaging in orthopaedics and sports medicine.3rd ed. Baltimore US: wolters kluwer health, 2007. Pg 1729</ref><br> | |||
== Characteristics/Clinical Presentation == | == Characteristics/Clinical Presentation == | ||
Patients with midcarpal instability typically present a range of symptoms, which may include wrist pain, clicking or snapping sounds, and reduced functional ability such as loss of strength and impaired prehension. Interestingly, many patients do not have a history of traumatic events. The symptoms can differ based on the specific subtype of midcarpal instability: | |||
* Palmar Midcarpal Instability (PMC): In addition to a "catch-up clunk" sound during extreme ulnar deviation, patients may find that activities requiring flexion exacerbate wrist pain. | |||
* Dorsal Midcarpal Instability: This subtype is often marked by dorsal wrist pain and a distinct "subluxation clunk" during wrist movements. | |||
* Extrinsic Midcarpal Instability: Persistent pain, particularly when lifting objects, is common. This subtype may also present with a deformity in wrist alignment. | |||
Discomfort, laxity, and an uncomfortable feeling in the wrist are also frequent complaints. | |||
== Differential Diagnosis == | == Differential Diagnosis == | ||
When assessing midcarpal instability, it's crucial to rule out other conditions that may present similar symptoms. These can include: | |||
* '''Carpal Tunnel Syndrome''': Characterised by numbness and tingling, particularly in the thumb and fingers. | |||
* '''Wrist Arthritis''': Involves joint pain and may show radiographic changes. | |||
* '''Wrist Sprain or Fracture''': Acute pain and swelling, often following a traumatic event. | |||
* '''Triangular Fibrocartilage Complex (TFCC) Tears''': Present with ulnar-sided wrist pain and may show positive findings on imaging tests like MRI. | |||
* '''Ganglion Cysts''': These can cause localised pain and may be visible as a lump near the wrist joint. | |||
== Diagnostic Procedures == | == Diagnostic Procedures == | ||
For an accurate diagnosis of midcarpal instability, often involves a combination of clinical assessment and imaging techniques. | |||
=== Radiology === | |||
While standard [[X-Rays|X-rays]], wrist arthrography, and [[MRI Scans|MRI]] are generally not useful for directly diagnosing midcarpal instability due to its dynamic nature, they are valuable for ruling out other conditions like fractures or lunotriquetral dissociation. These imaging techniques can also assess joint surfaces prior to surgical interventions. In cases of Palmar Midcarpal Instability (PMCI), MRI may show a VISI (Volar Intercalated Segmental Instability) pattern. | |||
=== Fluoroscopy === | |||
[[X-Rays|Fluoroscopy]] is often the primary imaging method for diagnosing midcarpal instability.<ref>Braunstein EM et al. Fluoroscopic and arthrographic evaluation of carpal instability. AJR Am J. Roentgenol.. 1985 Jun;14(6):1259-62</ref> It provides real-time insights into wrist joint movement. In patients with Palmar Midcarpal Instability (PMCI), a lateral view during radioulnar deviation often reveals a jump in the proximal row from flexion to extension. For those with Dorsal Midcarpal Instability (DMCI), dorsal subluxation of the capitate on the lunate becomes evident when pushing the capitate dorsally. This action not only produces a recognisable click but also causes patient apprehension, serving as a diagnostic sign.<ref>Slutsky D, Osterman A. Fractures and Injuries of the Distal Radius and Carpus. Ln: Carlos Heras-Palou MD. Midcarpal instability. First ed. Philadelphia: Saunders Elsevier, 2008</ref> <ref name=":2">Cooney WP. The wrist: Diagnosis and operative treatment. 2nd ed. Philadelphia, PA,:Lippincott Williams & Wilkins; 2010.pg 655-666</ref><br> | |||
Fluoroscopy is the imaging method | |||
== Outcome Measures == | == Outcome Measures == | ||
Effective treatment of midcarpal instability hinges on accurate outcome measurement tools. Some commonly used metrics include: | |||
* '''[[Visual Analogue Scale|Visual Analogue Scale (VAS)]]''': For pain assessment. | |||
* '''[[Patient-Rated Wrist Evaluation|Patient-Rated Wrist Evaluation (PRWE)]]''': Measures wrist pain and function. | |||
* '''[[Range of Motion|Range of Motion (ROM)]]''': Assesses wrist flexibility and movement limitations. | |||
* '''[[Grip Strength]]''': Measures the wrist and hand's ability to grasp objects securely. | |||
== Examination == | == Examination == | ||
A thorough clinical examination is key for the diagnosis of midcarpal instability. Key components include: | |||
[[File:Carpal Tunnel Syndrome.png|alt=Image showing carpal tunnel syndrome|right|frameless]] | |||
* '''Physical Inspection''': Checking for visible deformities, swelling, or redness. A palmar sag on the ulnar side of the carpus can be observed when the wrist is in neutral deviation, which often disappears with extreme ulnar deviation. | |||
* '''Palpation''': Feeling the wrist and surrounding areas for tenderness, especially over the ulnar carpus at the triquetrohamate joint. Localised synovitis may also be present. | |||
* '''Range of Motion Tests''': Assessing wrist flexibility and movement limitations, including a noticeable and painful clunk on the ulnar side during active ulnar deviation. | |||
* '''Provocative Tests''': Reproducing symptoms through tests like the midcarpal shift test, which is often positive in these patients. | |||
* '''Neurological Exam''': Ruling out similar conditions such as [[Carpal Tunnel Syndrome|carpal tunnel syndrome]]. A prominent ulnar head can often be observed when the wrist is in a neutral position. | |||
== Medical Management == | |||
Management of midcarpal instability often involves a combination of non-surgical and surgical treatments, tailored to the severity and specific needs of the patient.<ref name=":0" /><ref name=":1" /><ref name=":2" /> | |||
In order to meet all of the patient's needs, a multidisciplinary team approach is adopted and involves not only medical specialists like surgeons, rheumatologists, and radiologists but also healthcare professionals such as physiotherapists and occupational therapists. This well-rounded team plays a crucial role in both diagnosis and treatment planning, focusing on effective recovery that addresses physical symptoms as well as functional and emotional aspects of living with MCI. | |||
=== Non-surgical Treatment === | |||
Before exploring surgical avenues, it's essential to explore non-surgical management methods for Palmar Midcarpal Instability (PMCI). Common non-surgical treatments involve activity adjustment, proprioceptive retraining and may be suggested along with<ref name=":4">Ming BW, Niacaris T, Lichtman DM. Surgical techniques for the management of midcarpal instability. Journal of wrist surgery. 2014 Aug;3(03):171-4</ref>: | |||
* '''Wrist Braces or Splints''': Useful for providing support and restricting abnormal movements. | |||
* '''Physiotherapy''': Emphasises strengthening exercises and joint stabilisation. | |||
* '''Pain Management''': Via over-the-counter or prescribed medications. | |||
=== Surgical Treatment === | |||
For patients who find little or no relief through non-surgical methods, surgical options may be recommended as the next step. The selection of a particular surgical method may depend on the individual symptoms and underlying causes<ref name=":4" />: | |||
* '''Ligament-Specific Augmentation''': If ligaments are weakened and the ligament laxity can be pinpointed to a specific location, reinforcing the ligament may be beneficial. This is achieved through autografts, allografts, or synthetic materials. | |||
* '''Ligament Reconstruction:''' This involves replacing the damaged ligament entirely. A graft is often taken, or rerouted, from another ligament and is indicated when a ligament is severely damaged or torn. <ref name=":4" /> | |||
* '''Soft Tissue Procedures''': Such as distal advancement of the volar arcuat ligament or dorsal radiocarpalcapsulodesis, used in mild to moderate cases. | |||
* '''Midcarpal Arthrodesis''': Employed in severe cases, and includes 4-quadrant fusions, radial fusions, or triquetrohamate fusion. | |||
* '''Treatment for Extrinsic MCI''': Consists of radial shortening, radial osteotomy, or ulnar lengthening. | |||
* '''Treatment for Dorsal MCI''': Involves closing the space of Poirier by imbricating specific palmar ligaments. | |||
== Physiotherapy Management == | == Physiotherapy Management == | ||
Physiotherapy plays a vital role in the management of midcarpal instability, offering both preventive and rehabilitative approaches. | |||
''< | * Non-Surgical Treatment | ||
** '''Medication''': Initial treatment often includes nonsteroidal anti-inflammatory drugs (NSAIDs) and sometimes steroid injections for substantial synovitis. | |||
** '''Education''': Therapists guide patients to recognise and avoid compensatory movements and pain-provoking activities. | |||
* Splint Immobilisation | |||
** Gutter splints are often used in conjunction with a pisiform boost pad. This pisiform boost pad is often combined with a dorsal pressure pad over the ulnar head. | |||
** Modified perilunate stabilising splints can be used if other methods are not successful in controlling the subluxation. This forearm based wrist support splint controls the scaphoid and the scaphotrapezial trapezoid joint by exerting dorsally directed pressure on the scaphoid tuberosity and the trapezoid ridge. This controls flexion tendency of the proximal carpal row by dorsally directed pressure on the pisiformis. <ref name=":2" /> | |||
* Dynamic Strengthening Exercises - Once symptom reduction is observed, focus shifts to strengthening specific muscles including the M. flexor carpi ulnaris, M. flexor carpi radialis, and M. extensor carpi radialis longus and brevis. | |||
** Palmarflexion and Dorsiflexion | |||
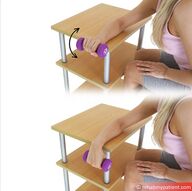
*** [[File:Wrist Extension with weightRMP.jpg|alt=Image showing wrist extension with a weight|right|frameless|192x192px]]'''Table Exercise''': With your forearm fixed on a table, use weights or a Theraband to slowly lift your hand upwards. Increase resistance as you progress. | |||
*** '''Wrist Roll''': Stand with arms extended holding a roller. Slowly roll the chain up and down using wrist motion, keeping the rest of your body stationary. Add weights for more resistance. | |||
** Ulnar and Radial Deviation[[File:Resisted Radial Deviation.gif|alt=Image of resisted radial deviation|right|frameless|175x175px]] | |||
*** '''Arm Extension Exercise''': With your arm extended and holding a weight or using a theraband, move your hand forwards for radial deviation and backwards for ulnar deviation. | |||
== Occupational Therapists == | |||
Occupational therapists (OTs) also play a major role in rehabilitating patients with Midcarpal Instability (MCI). They focus on enabling patients to engage in everyday activities, minimising pain, and enhancing wrist stability and function. Their aim is to facilitate independence in daily living and work tasks. This involves setting achievable, patient-centred goals aimed at symptom management, function restoration, and quality-of-life improvement. | |||
* Functional Assessment and Adaptation | |||
** Evaluate the patient's ability to perform essential tasks and recommend ergonomic adaptations for work and home settings. | |||
* Splinting and Orthotic Management | |||
** Provide specialised splints to improve wrist stability, often customising them to meet individual needs. | |||
* Pain Management Strategies | |||
** Employ non-pharmacological methods, such as thermal modalities and soft tissue mobilisation, to manage symptoms. | |||
* Develop a tailored rehabilitation programme which may include: | |||
** Strengthening exercises | |||
** Range-of-motion exercises | |||
** Activity pacing strategies | |||
* Education and Training | |||
** Teach patients about wrist anatomy and MCI, compensatory movements, and techniques to avoid exacerbation of symptoms. | |||
* Activity Re-Training | |||
** Instruct on techniques and aids for daily living tasks such as cooking, writing, and other hand-intensive activities. | |||
== Conclusion == | |||
Midcarpal Instability is a complex wrist condition that necessitates a comprehensive diagnostic and management approach. Management is a multidisciplinary effort, requiring input from various healthcare professionals to offer comprehensive care. While physiotherapists mainly target functional recovery and muscular strengthening, occupational therapists concentrate on facilitating the patient's return to everyday activities and work tasks, offering a holistic approach to rehabilitation. A blend of surgical and nonsurgical interventions, physiotherapy, and occupational therapy can lead to significant improvements in patient outcomes. | |||
<br><br> | |||
== References == | == References == | ||
<references/> | <references/> | ||
Latest revision as of 11:08, 16 October 2023
Original Editors - Hannah Willocx
Top Contributors - Hannah Willocx, Kim Jackson, Admin and WikiSysop
Definition/Description[edit | edit source]
Midcarpal Instability (MCI) is a condition affecting the wrist joint. It manifests as increased, abnormal mobility between the proximal and distal rows of the carpal bones. Common symptoms include persistent wrist pain, clicking, and limited functional capacity. The instability stems from lack of support of the proximal carpal row by ligamentous structures, as well as a disruption of normal joint forces between proximal and distal carpal rows. Palmar midcarpal instability is more prevalent, but dorsal and extrinsic variants also exist.[1]
Clinically Relevant Anatomy[edit | edit source]
The wrist is composed of eight carpal bones arranged in two rows. The proximal row includes the scaphoid, lunate, and triquetrum. The distal row consists of the trapezium, trapezoid, capitate, and hamate. Ligaments connect these bones, stabilising the joint.


Key to the stability of the midcarpal joint is the arcuate ligament complex. This complex has two parts: an ulnar part, comprised of the triquetrohamatecapitate ligament, and a radial part that extends distally from the radioscaphocapitate ligament. Another important stabilising element for the proximal carpal row is the dorsal radiolunotriquetral ligament.
Epidemiology /Aetiology[edit | edit source]
Midcarpal instability is an uncommon condition but is more frequently seen in younger adults and athletes.[2] It often results from factors such as ligament laxity, trauma, or repetitive strain on the wrist. Two main forms, congenital and acquired, exist.[2] The acquired form is commonly linked with wrist trauma or repetitive stress, and certain systemic conditions like rheumatoid arthritis may also contribute. The types of instability are:
- Palmar Midcarpal Instability (PMC): This subtype is primarily caused by laxity in specific ligaments, namely the ulnar component of the arcuate ligament and the dorsal radiolunotriquetral ligament. These ligament issues result in abnormal movement in the carpal rows, leading to a condition known as a flexion deformity. The deformity disrupts the normal rotational coupling of the carpal bones, leading to the "catch-up clunk" sound during extreme ulnar deviation.[1][3]Notably, up to 70% of Ehlers–Danlos syndrome patients, particularly those with the hypermobility type, experience painful midcarpal laxity. However, this instability often tightens up over time, making it self-limiting in these patients.[4][5]
- Dorsal Midcarpal Instability: Laxity in the palmar radioscapocapitate ligament results in dorsal subluxation of the midcarpal joint. This creates a unique "subluxation clunk" sound.
- Extrinsic Midcarpal Instability: This form is usually secondary to distal radius malunions that result in malalignment. This causes a dorsal displacement of the distal radius and an adaptive Z-deformity in the carpal bones.[6]
Characteristics/Clinical Presentation[edit | edit source]
Patients with midcarpal instability typically present a range of symptoms, which may include wrist pain, clicking or snapping sounds, and reduced functional ability such as loss of strength and impaired prehension. Interestingly, many patients do not have a history of traumatic events. The symptoms can differ based on the specific subtype of midcarpal instability:
- Palmar Midcarpal Instability (PMC): In addition to a "catch-up clunk" sound during extreme ulnar deviation, patients may find that activities requiring flexion exacerbate wrist pain.
- Dorsal Midcarpal Instability: This subtype is often marked by dorsal wrist pain and a distinct "subluxation clunk" during wrist movements.
- Extrinsic Midcarpal Instability: Persistent pain, particularly when lifting objects, is common. This subtype may also present with a deformity in wrist alignment.
Discomfort, laxity, and an uncomfortable feeling in the wrist are also frequent complaints.
Differential Diagnosis[edit | edit source]
When assessing midcarpal instability, it's crucial to rule out other conditions that may present similar symptoms. These can include:
- Carpal Tunnel Syndrome: Characterised by numbness and tingling, particularly in the thumb and fingers.
- Wrist Arthritis: Involves joint pain and may show radiographic changes.
- Wrist Sprain or Fracture: Acute pain and swelling, often following a traumatic event.
- Triangular Fibrocartilage Complex (TFCC) Tears: Present with ulnar-sided wrist pain and may show positive findings on imaging tests like MRI.
- Ganglion Cysts: These can cause localised pain and may be visible as a lump near the wrist joint.
Diagnostic Procedures[edit | edit source]
For an accurate diagnosis of midcarpal instability, often involves a combination of clinical assessment and imaging techniques.
Radiology[edit | edit source]
While standard X-rays, wrist arthrography, and MRI are generally not useful for directly diagnosing midcarpal instability due to its dynamic nature, they are valuable for ruling out other conditions like fractures or lunotriquetral dissociation. These imaging techniques can also assess joint surfaces prior to surgical interventions. In cases of Palmar Midcarpal Instability (PMCI), MRI may show a VISI (Volar Intercalated Segmental Instability) pattern.
Fluoroscopy[edit | edit source]
Fluoroscopy is often the primary imaging method for diagnosing midcarpal instability.[7] It provides real-time insights into wrist joint movement. In patients with Palmar Midcarpal Instability (PMCI), a lateral view during radioulnar deviation often reveals a jump in the proximal row from flexion to extension. For those with Dorsal Midcarpal Instability (DMCI), dorsal subluxation of the capitate on the lunate becomes evident when pushing the capitate dorsally. This action not only produces a recognisable click but also causes patient apprehension, serving as a diagnostic sign.[8] [9]
Outcome Measures[edit | edit source]
Effective treatment of midcarpal instability hinges on accurate outcome measurement tools. Some commonly used metrics include:
- Visual Analogue Scale (VAS): For pain assessment.
- Patient-Rated Wrist Evaluation (PRWE): Measures wrist pain and function.
- Range of Motion (ROM): Assesses wrist flexibility and movement limitations.
- Grip Strength: Measures the wrist and hand's ability to grasp objects securely.
Examination [edit | edit source]
A thorough clinical examination is key for the diagnosis of midcarpal instability. Key components include:

- Physical Inspection: Checking for visible deformities, swelling, or redness. A palmar sag on the ulnar side of the carpus can be observed when the wrist is in neutral deviation, which often disappears with extreme ulnar deviation.
- Palpation: Feeling the wrist and surrounding areas for tenderness, especially over the ulnar carpus at the triquetrohamate joint. Localised synovitis may also be present.
- Range of Motion Tests: Assessing wrist flexibility and movement limitations, including a noticeable and painful clunk on the ulnar side during active ulnar deviation.
- Provocative Tests: Reproducing symptoms through tests like the midcarpal shift test, which is often positive in these patients.
- Neurological Exam: Ruling out similar conditions such as carpal tunnel syndrome. A prominent ulnar head can often be observed when the wrist is in a neutral position.
Medical Management[edit | edit source]
Management of midcarpal instability often involves a combination of non-surgical and surgical treatments, tailored to the severity and specific needs of the patient.[1][3][9]
In order to meet all of the patient's needs, a multidisciplinary team approach is adopted and involves not only medical specialists like surgeons, rheumatologists, and radiologists but also healthcare professionals such as physiotherapists and occupational therapists. This well-rounded team plays a crucial role in both diagnosis and treatment planning, focusing on effective recovery that addresses physical symptoms as well as functional and emotional aspects of living with MCI.
Non-surgical Treatment[edit | edit source]
Before exploring surgical avenues, it's essential to explore non-surgical management methods for Palmar Midcarpal Instability (PMCI). Common non-surgical treatments involve activity adjustment, proprioceptive retraining and may be suggested along with[10]:
- Wrist Braces or Splints: Useful for providing support and restricting abnormal movements.
- Physiotherapy: Emphasises strengthening exercises and joint stabilisation.
- Pain Management: Via over-the-counter or prescribed medications.
Surgical Treatment[edit | edit source]
For patients who find little or no relief through non-surgical methods, surgical options may be recommended as the next step. The selection of a particular surgical method may depend on the individual symptoms and underlying causes[10]:
- Ligament-Specific Augmentation: If ligaments are weakened and the ligament laxity can be pinpointed to a specific location, reinforcing the ligament may be beneficial. This is achieved through autografts, allografts, or synthetic materials.
- Ligament Reconstruction: This involves replacing the damaged ligament entirely. A graft is often taken, or rerouted, from another ligament and is indicated when a ligament is severely damaged or torn. [10]
- Soft Tissue Procedures: Such as distal advancement of the volar arcuat ligament or dorsal radiocarpalcapsulodesis, used in mild to moderate cases.
- Midcarpal Arthrodesis: Employed in severe cases, and includes 4-quadrant fusions, radial fusions, or triquetrohamate fusion.
- Treatment for Extrinsic MCI: Consists of radial shortening, radial osteotomy, or ulnar lengthening.
- Treatment for Dorsal MCI: Involves closing the space of Poirier by imbricating specific palmar ligaments.
Physiotherapy Management[edit | edit source]
Physiotherapy plays a vital role in the management of midcarpal instability, offering both preventive and rehabilitative approaches.
- Non-Surgical Treatment
- Medication: Initial treatment often includes nonsteroidal anti-inflammatory drugs (NSAIDs) and sometimes steroid injections for substantial synovitis.
- Education: Therapists guide patients to recognise and avoid compensatory movements and pain-provoking activities.
- Splint Immobilisation
- Gutter splints are often used in conjunction with a pisiform boost pad. This pisiform boost pad is often combined with a dorsal pressure pad over the ulnar head.
- Modified perilunate stabilising splints can be used if other methods are not successful in controlling the subluxation. This forearm based wrist support splint controls the scaphoid and the scaphotrapezial trapezoid joint by exerting dorsally directed pressure on the scaphoid tuberosity and the trapezoid ridge. This controls flexion tendency of the proximal carpal row by dorsally directed pressure on the pisiformis. [9]
- Dynamic Strengthening Exercises - Once symptom reduction is observed, focus shifts to strengthening specific muscles including the M. flexor carpi ulnaris, M. flexor carpi radialis, and M. extensor carpi radialis longus and brevis.
- Palmarflexion and Dorsiflexion
- Table Exercise: With your forearm fixed on a table, use weights or a Theraband to slowly lift your hand upwards. Increase resistance as you progress.
- Wrist Roll: Stand with arms extended holding a roller. Slowly roll the chain up and down using wrist motion, keeping the rest of your body stationary. Add weights for more resistance.
- Ulnar and Radial Deviation

- Arm Extension Exercise: With your arm extended and holding a weight or using a theraband, move your hand forwards for radial deviation and backwards for ulnar deviation.
- Palmarflexion and Dorsiflexion


Occupational Therapists[edit | edit source]
Occupational therapists (OTs) also play a major role in rehabilitating patients with Midcarpal Instability (MCI). They focus on enabling patients to engage in everyday activities, minimising pain, and enhancing wrist stability and function. Their aim is to facilitate independence in daily living and work tasks. This involves setting achievable, patient-centred goals aimed at symptom management, function restoration, and quality-of-life improvement.
- Functional Assessment and Adaptation
- Evaluate the patient's ability to perform essential tasks and recommend ergonomic adaptations for work and home settings.
- Splinting and Orthotic Management
- Provide specialised splints to improve wrist stability, often customising them to meet individual needs.
- Pain Management Strategies
- Employ non-pharmacological methods, such as thermal modalities and soft tissue mobilisation, to manage symptoms.
- Develop a tailored rehabilitation programme which may include:
- Strengthening exercises
- Range-of-motion exercises
- Activity pacing strategies
- Education and Training
- Teach patients about wrist anatomy and MCI, compensatory movements, and techniques to avoid exacerbation of symptoms.
- Activity Re-Training
- Instruct on techniques and aids for daily living tasks such as cooking, writing, and other hand-intensive activities.
Conclusion[edit | edit source]
Midcarpal Instability is a complex wrist condition that necessitates a comprehensive diagnostic and management approach. Management is a multidisciplinary effort, requiring input from various healthcare professionals to offer comprehensive care. While physiotherapists mainly target functional recovery and muscular strengthening, occupational therapists concentrate on facilitating the patient's return to everyday activities and work tasks, offering a holistic approach to rehabilitation. A blend of surgical and nonsurgical interventions, physiotherapy, and occupational therapy can lead to significant improvements in patient outcomes.
References[edit | edit source]
- ↑ 1.0 1.1 1.2 Lichtman DM, Wroten ES. Understanding Midcarpal Instability. Journal of Hand Surgery [AM]. 2006; 31A:491–498
- ↑ 2.0 2.1 Jing SS, Smith G, Deshmukh S. Demystifying palmar midcarpal instability. Journal of Wrist Surgery. 2020 Aug 27;10(02):094-101.
- ↑ 3.0 3.1 Buchler U. Wrist instability. Ln: Gaenslen ES, Lichtman DM. Midcarpal instability: description, classification, and treatment. First ed. UK; The livery house, 1996. pg 163-168
- ↑ Niacaris T, Ming BW, Lichtman DM. Midcarpal instability: a comprehensive review and update. Hand Clin 2015;31(03):487–493
- ↑ 1 Woerdeman LAE, Ritt MJPF, Meijer B, Maas M. Wrist problems in patients with Ehlers-Danlos syndrome. Eur J Plast Surg 2000; 23:208–210
- ↑ Stoller DW. Midcarpal instabilities. Magnetic resonance imaging in orthopaedics and sports medicine.3rd ed. Baltimore US: wolters kluwer health, 2007. Pg 1729
- ↑ Braunstein EM et al. Fluoroscopic and arthrographic evaluation of carpal instability. AJR Am J. Roentgenol.. 1985 Jun;14(6):1259-62
- ↑ Slutsky D, Osterman A. Fractures and Injuries of the Distal Radius and Carpus. Ln: Carlos Heras-Palou MD. Midcarpal instability. First ed. Philadelphia: Saunders Elsevier, 2008
- ↑ 9.0 9.1 9.2 Cooney WP. The wrist: Diagnosis and operative treatment. 2nd ed. Philadelphia, PA,:Lippincott Williams & Wilkins; 2010.pg 655-666
- ↑ 10.0 10.1 10.2 Ming BW, Niacaris T, Lichtman DM. Surgical techniques for the management of midcarpal instability. Journal of wrist surgery. 2014 Aug;3(03):171-4

