Myocardial Infarction
Original Editors - Jessica King & Melissa Tuemler from Bellarmine University's Pathophysiology of Complex Patient Problems project.
Top Contributors - Jessica King, Melissa Tuemler, Lucinda hampton, Vidya Acharya, Kim Jackson, Admin, Elaine Lonnemann, WikiSysop, Wendy Walker, Evan Thomas, Venus Pagare and Karen Wilson
Definition/Description[edit | edit source]

Myocardial infarction (MI) or “heart attack,” is caused by decreased or complete cessation of blood flow to a portion of the myocardium.
Myocardial infarction
- May be “silent” and go undetected, or it could be a catastrophic event leading to hemodynamic deterioration and sudden death.
- Mainly due to underlying coronary artery disease. When the coronary artery is occluded, the myocardium is deprived of oxygen. Prolonged deprivation of oxygen supply to the myocardium can lead to myocardial cell death and necrosis.
- May be associated with ECG changes and elevated biochemical markers such as cardiac troponins
Patients can present with chest discomfort or pressure that can radiate to the neck, jaw, shoulder, or arm.[1]
Etiology[edit | edit source]

Myocardial infarction is closely associated with coronary artery disease, and the risk factors for MI are similarly associated with the below:
- Smoking
- Abnormal lipid profile/blood apolipoprotein (raised ApoB/ApoA1)
- Hypertension
- Diabetes mellitus
- Abdominal obesity (waist/hip ratio) (greater than 0.90 for males and greater than 0.85 for females)
- Psychosocial factors such as depression, loss of the locus of control, global stress, financial stress, and life events including marital separation, job loss, and family conflicts
- Lack of daily consumption of fruits or vegetables
- Lack of physical activity
Some non-modifiable risk factors for myocardial infarction include:
- Advanced age
- Male gender (males tend to have myocardial infarction earlier in life)
- Genetics (there is an increased risk of MI if a first-degree relative has a history of cardiovascular events before the age of 50). The role of genetic loci that increase the risk for MI is under active investigation[1]
Epidemiology[edit | edit source]
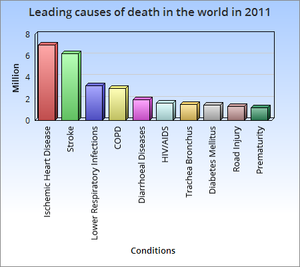
- The most common cause of death and disability in the western world and worldwide is coronary artery disease[1].
- There are 32.4 million myocardial infarctions and strokes worldwide every year.
- Patients with previous myocardial infarction (MI) are the highest risk group for further coronary events.
- Survivors of MI are at increased risk of recurrent infarctions and have an annual death rate of 5% - six times that in people of the same age who do not have coronary heart disease.[2]
- Myocardial Infarctions are the leading cause of death in the industrialized nations of the world. In the United States, there are about 450,000 deaths due to MIs each year. Now 95% of patients hospitalized with an MI will survive due to improvements in emergency response time, and treatment techniques. The risk of having an MI increases with age, but 50% of MIs in the United States occur in people under the age of 65 years old.[3]

Characteristics/Clinical Presentation[edit | edit source]

Myocardial ischemia can present as
- Chest pain, upper extremity pain, mandibular, or epigastric discomfort that occurs during exertion or at rest and is usually not affected by positional changes or active movement of the region. Chest pain (usually retrosternal), sometimes described as the sensation of pressure or heaviness.
- Pain radiating to the left shoulder, neck, or arms (with no obvious precipitating factors), and it may be intermittent or persistent.
- Dyspnea or fatigue.
- Pain lasting more than 20 minutes
- Additional symptoms, such as sweating, nausea, abdominal pain, dyspnea, and syncope, may also be present.
- Atypical with subtle findings such as palpitations
- Dramatic manifestations, such as cardiac arrest. [1]
- Silent ie with no symptoms.
Signs and symptoms vary based on gender.
- The most common symptom experienced by both genders is chest pain or discomfort.
- Women typically experience other symptoms such as SOA, nausea and vomiting, and neck or jaw pain[4].
Treatment[edit | edit source]

The diagnosis and management of patients with MI is best done with an interprofessional team. In most hospitals, there are cardiology teams that are dedicated to the management of these patients.
For patients who present with chest pain, the key to the management of MI is time to treatment.
- A cardiology consult should be made immediately to ensure that the patient gets treated within the time frame recommendations.
- As MI can be associated with several serious complications, these patients are best managed in an ICU setting.
Long term management
There is no cure for ischemic heart disease, and all treatments are symptom-oriented.
- The key to improving outcomes is to prevent coronary artery disease.
- The primary care provider, physiotherapist and nurse practitioner should educate the patient on the benefits of a healthy diet, the importance of controlling blood pressure and diabetes, exercising regularly, discontinuing smoking, maintaining healthy body weight, and remaining compliant with medications.
- The pharmacist should educate the patient on types of medication used to treat ischemic heart disease, their benefits, and potential adverse effects.
Prognosis[edit | edit source]
Acute MI carries a mortality rate of 5-30%; the majority of deaths occur prior to arrival to the hospital.
- Within the first year after an MI, there is an additional mortality rate of 5% to 12%.
- Overall prognosis depends on the extent of heart muscle damage and ejection fraction. Patients with preserved left ventricular function tend to have good outcomes.
Factors that worsen prognosis include:
- Diabetes
- Advanced age
- Delayed reperfusion
- Low ejection fraction
- Presence of congestive heart failure
- Elevations in C-reactive protein and B-type natriuretic peptide (BNP) levels
- Depression[1]
Evaluation[edit | edit source]

The three components in the evaluation of the MI are clinical features, ECG findings, and cardiac biomarkers.
The resting 12 lead ECG is the first-line diagnostic tool for the diagnosis of acute coronary syndrome (ACS). It should be obtained within 10 minutes of the patient’s arrival in the emergency department. Acute MI is often associated with dynamic changes in the ECG waveform. Serial ECG monitoring can provide important clues to the diagnosis if the initial EKG is non-diagnostic at initial presentation[1].
2. Biomarker Detection of MI
- Cardiac troponins (I and T) are components of the contractile apparatus of myocardial cells and expressed almost exclusively in the heart.
- A troponin test measures the levels of troponin T or troponin I proteins in the blood. These proteins are released when the heart muscle has been damaged, such as occurs with a heart attack. The more damage there is to the heart, the greater the amount of troponin T and I there will be in the blood[5].
3. Imaging
- Used to assess myocardial perfusion, myocardial viability, myocardial thickness, thickening and motion, and the effect of myocyte loss on the kinetics of para-magnetic or radio-opaque contrast agents indicating myocardial fibrosis or scars.
- Some imaging modalities that can be used are echocardiography, radionuclide imaging, and cardiac magnetic resonance imaging (cardiac MRI).
Physical Therapy Management[edit | edit source]

- Beneficial to patients of all ages who have had a heart attack, CAD, angina, or CHF.
- Other individuals who may gain benefits from this include post-surgical CABG, percutaneous intervention (PCI), or coronary angioplasty patients.
Cardiac Rehab.
- A medical examination is completed at the initial consultation to determine the needs and limitations of the patient.
- The results of the exam are interpreted, the team creates a rehab program and sets goals for treatment.
- Treatment typically consists of a physical activity program in a group setting where vital signs can consistently be monitored. As the program progresses, the patient is taught how to monitor their own vitals and progresses to more challenging aerobic activities.
- Cycle Ergometer Use in the post-operative period following cardiac surgery is a safe choice for patient rehabilitation[6].
- Along with physical activity, patient education is also a very important part of cardiac rehab. Patients may work with a dietician or be given advice on how to stop smoking if necessary.
According to the American Heart Association, the benefits of cardiac rehab include:
- Regular physical activity helps your heart and the rest of your body get stronger and work better. Physical activity improves your energy level and lifts your spirits. It also reduces your chances of future heart problems, including heart attack.
- Counseling and education can help you quit smoking, eat right, lose weight, and lower your blood pressure and cholesterol levels. Counseling may also help you learn to manage stress and to feel better about your health.
- You have the advice and close supervision of healthcare professionals to help you improve your health and lower your risk of future problems. These professionals can also communicate with your primary care doctor or cardiologist. [7]
Prevention[edit | edit source]
Evidence based interventions for secondary prevention include the use of aspirin, beta-blockers, angiotensin converting enzyme inhibitors; lipid lowering drugs and other anti- hypertensives, as well as modifying lifestyle related risk behaviours.
Physical exercise
Although the role of exercise alone in reducing cardiovascular outcomes is not clear, systematic reviews of RCTs have found that cardiac rehabilitation which includes physical exercise improves coronary risk factors and reduces the risk of major cardiac events in people after MI.
Dietary Modification

RCTs have found that advising people with MI to eat more fish, fruit and vegetables, bread, pasta, potatoes, olive oil and margarine may result in a substantial survival advantage.
Stopping smoking
Apart from these pharmacological measures for secondary prevention, evidence is available that lifestyle measures such as stopping smoking, encouraging a healthy diet and exercise can also significantly contribute to reduction in cardiovascular mortality in people with established CVD. Evidence from epidemiological studies indicates that people with coronary heart disease who stop smoking rapidly reduce their risk of recurrent coronary events or death. In the case of stroke survivors, observational studies have shown that the excess risk of stroke among former smokers largely disappeared 2-4 years after smoking cessation[2].
Medications[edit | edit source]
Following an MI, patients will most likely be prescribed some form of medication for the rest of their lives[8].
| Vasodilators (Nitrates) |
Relaxes blood vessels and increases the supply of blood and oxygen to the heart while reducing its workload. Can come in pills to be swallowed, chewable tablets and as a topical application (cream). |
| Digitalis Preparations (Lanoxin) |
Increases the force of the heart's contractions, which can be beneficial in heart failure and for irregular heartbeats. |
| Statins |
Various medications can lower blood cholesterol levels. They may be prescribed individually or in combination with other drugs. They work in the body in different ways. Some affect the liver, some work in the intestines and some interrupt the formation of cholesterol from circulating in the blood. |
Resources[edit | edit source]
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 Ojha N, Dhamoon AS. Myocardial Infarction. InStatPearls [Internet] 2019 Dec 4. StatPearls Publishing. Available from:https://www.ncbi.nlm.nih.gov/books/NBK537076/ (last accessed 27.8.2020)
- ↑ 2.0 2.1 WHO Prevention MI Available from:https://www.who.int/cardiovascular_diseases/priorities/secondary_prevention/country/en/index1.html (last accessed 27.8.2020)
- ↑ Cleveland Clinic. Acute Myocardial Infarction. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/cardiology/acute-myocardial-infarction/#s0015 (12 Feb 2013)
- ↑ American Heart Association. Warning signs of a Heart Attack. http://www.heart.org/HEARTORG/Conditions/HeartAttack/WarningSignsofaHeartAttack/Warning-Signs-of-a-Heart-Attack_UCM_002039_Article.jsp (accessed 10 Feb 2013).
- ↑ Medline plus Troponin test Available from:https://medlineplus.gov/ency/article/007452.htm (last accessed 27.8.2020)
- ↑ Gama Lordello GG, Gonçalves Gama GG, Lago Rosier G, Viana PA, Correia LC, Fonteles Ritt LE. Effects of cycle ergometer use in early mobilization following cardiac surgery: a randomized controlled trial. Clinical Rehabilitation. 2020 Jan 29:0269215520901763.
- ↑ American Heart Association.What is Cardiac Rehab? http://www.heart.org/HEARTORG/Conditions/More/CardiacRehab/What-is-Cardiac-Rehabilitation_UCM_307049_Article.jsp (accessed 11 Feb 2013).
- ↑ American Heart Association. Cardiac Medications. http://www.heart.org/HEARTORG/Conditions/HeartAttack/PreventionTreatmentofHeartAttack/Cardiac-Medications_UCM_303937_Article.jsp (accessed 11 Feb 2013).

