Management of Ankle Osteochondral Lesions: Difference between revisions
No edit summary |
No edit summary |
||
| (21 intermediate revisions by 5 users not shown) | |||
| Line 1: | Line 1: | ||
<div class="editorbox"> '''Original Editor '''- [[User:Ewa Jaraczewska|Ewa Jaraczewska]] based on the course by [https://members.physio-pedia.com/instructor/helene-simpson/ Helene Simpson] | <div class="editorbox"> '''Original Editor '''- [[User:Ewa Jaraczewska|Ewa Jaraczewska]] based on the course by [https://members.physio-pedia.com/instructor/helene-simpson/ Helene Simpson] | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}}</div> | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}}</div> | ||
== Definitions == | == Definitions == | ||
Cartilage is a connective tissue | [[File:Three-types-of-cartilage-hyaline-elastic-and-fibrocartilage.png|thumb|392x392px|The 3 types of cartilage]] | ||
[[Cartilage]] is a connective tissue which has the following components:<ref name=":3">Armiento AR, Alini M, Stoddart MJ. [https://www.sciencedirect.com/science/article/pii/S0169409X18303193?via%3Dihub Articular fibrocartilage - Why does hyaline cartilage fail to repair?] Adv Drug Deliv Rev. 2019 Jun;146:289-305.</ref> | |||
* Polysaccharides ( a cellular component composed of ground substance) | * Polysaccharides (a cellular component composed of ground substance) | ||
* Fibrous proteins | * Fibrous proteins | ||
* Interstitial fluid with water as the main component | * Interstitial fluid with water as the main component | ||
Cartilage gets its nutrition via diffusion from surrounding tissues as it has no direct blood supply, lymphatics | Cartilage gets its nutrition via diffusion from surrounding tissues as it has no direct [[Blood Physiology|blood]] supply, [[Lymphatic System|lymphatics]] or [[Neurone|nerve]]<nowiki/>s.<ref name=":3" /> | ||
There are three types of cartilaginous tissues: hyaline, fibrocartilage and elastic cartilage.<ref name=":3" /> Each type of cartilaginous tissue has a different composition and function: | |||
#[[File:Extracellular Matrix Components of Cartilage.jpeg|right|frameless|364x364px]][[Cartilage|Hyaline cartilage]]: is a connective tissue located at the ends of bones. Its primary cells are chondrocytes. Their role is to maintain the cartilage [[Extracellular Matrix|extracellular matrix]] (ECM), which is responsible for the biological and mechanical function of the cartilage. Hyaline cartilage ECM contains:<ref>Lakin BA, Snyder BD, Grinstaff MW. [https://www.annualreviews.org/doi/full/10.1146/annurev-bioeng-071516-044525 Assessing cartilage biomechanical properties: techniques for evaluating the functional performance of cartilage in health and disease. Annual review of biomedical engineering]. 2017 Jun 21;19:27-55.</ref> | |||
#* Type II [[collagen]] (10-20%) | |||
#* Proteoglycan (1-10%) | |||
#* Water (65-85%) | |||
#[[Cartilage|Fibrocartilage]] is a "transitional tissue between hyaline cartilage and dense regular connective tissue."<ref name=":3" /> This type of tissue can be found in the pubic symphysis, the annulus fibrosus of intervertebral disc, tendons, and ligaments.<ref>Donahue RP, Gonzalez-Leon EA, Hu JC, Athanasiou K. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6611470/pdf/bio-18-1303_070802.pdf Considerations for translation of tissue engineered fibrocartilage from bench to bedside.] J Biomech Eng. 2018 Dec 5;141(7):0708021–07080216.</ref> It contains:<ref name=":3" /> | |||
#* High levels of type I collagen | |||
#* Type II collagen | |||
#* A small component of ground substance | |||
#[[Cartilage|Elastic cartilage]]: is a flexible connective tissue cartilage that can withstand repeated bending.<ref name=":3" /> It consists of:<ref name=":3" /> | |||
#* Type II collagen | |||
#* Elastic fibres | |||
#* Large chondrocytes | |||
[[Bone|Subchondral bone]] is located below the hyaline cartilage and cement line (i.e. the border between calcified cartilage and the subchondral [[bone]]<ref>Li G, Yin J, Gao J, Cheng TS, Pavlos NJ, Zhang C, et al. [https://link.springer.com/article/10.1186/ar4405 Subchondral bone in osteoarthritis: insight into risk factors and microstructural changes]. Arthritis Res Ther. 2013;15(6):223. </ref>). It is responsible for providing mechanical (including shock absorption) and nutritional support for cartilage (the subchondral bone containing vessels that directly interact with the hyaline cartilage layer)<ref>Hu Y, Chen X, Wang S, Jing Y, Su J. [https://www.nature.com/articles/s41413-021-00147-z.pdf Subchondral bone microenvironment in osteoarthritis and pain]. Bone research. 2021 Mar 17;9(1):1-3.</ref>. The perfusion mechanism of the subchondral bone vessels is responsible for distributing 50% of nutrients to the cartilage.<ref>Imhof H, Sulzbacher I, Grampp S, Czerny C, Youssefzadeh S, Kainberger F. Subchondral bone and cartilage disease: a rediscovered functional unit. Investigative radiology. 2000 Oct 1;35(10):581-8.</ref> | |||
'''Osteochondral lesions (OCL)''' are defects affecting the structure of the cartilaginous surface and underlying subchondral bone. When the lesion's healing phase begins and tissue forms, the new tissue is often fibrocartilage. However, this type of cartilage has mechanical disadvantages to hyaline cartilage. In some cases, hyaline cartilage forms during the repair process, but the mechanism of hyaline vs fibrocartilage formation is unknown.<ref name=":3" /> | |||
Osteochondral lesions | |||
== Healing of '''Osteochondral Lesions'''== | |||
Osteochondral lesions have poor healing capacity.<ref name=":4">Lydon H, Getgood A, Henson FMD. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6376560/ Healing of Osteochondral Defects via Endochondral Ossification in an Ovine Model]. Cartilage. 2019 Jan;10(1):94-101.</ref> A study completed in animals<ref>Shapiro F, Koide S, Glimcher MJ. Cell origin and differentiation in the repair of full-thickness defects of articular cartilage. J Bone Joint Surg Am. 1993 Apr;75(4):532-53. </ref> demonstrates that OCLs go through the following stages of healing:<ref name=":4" /> | |||
Week 4-8: Cartilage formation starts adjacent to the damaged cartilage | * Week 1-2: Initial fibrin repair - the damaged site begins to fill with a blood clot and fibrous tissue, mesenchymal cell recruitment begins | ||
* Week 4-8: Cartilage formation starts adjacent to the damaged cartilage | |||
* Weeks 8 -12: Bone formation begins through endochondral ossification | |||
* Week 18: New bone formation continues | |||
* Week 26: Completion of the healing process | |||
=== Aetiology of '''Osteochondral Lesions'''=== | |||
Osteochondral lesions can be caused by: | |||
* Trauma (80% of cases)<ref name=":5">Krause F, Anwander H. [https://eor.bioscientifica.com/view/journals/eor/7/6/EOR-22-0024.xml Osteochondral lesion of the talus: still a problem?]. EFORT open reviews. 2022 Jun 1;7(6):337-43.</ref> | |||
* Joint malalignment<ref name=":0">Mosca M, Grassi A, Caravelli S. Osteochondral Lesions of Ankle and Knee. Will Future Treatments Really Be Represented by Custom-Made Metal Implants?. Journal of Clinical Medicine. 2022 Jul 1;11(13):3817.</ref> | |||
* [[Ligament]] laxity (38% of patients)<ref name=":5" /> | |||
* Instability (39% of patients)<ref name=":5" /> | |||
* [[Genetics and Health|Genetic predisposition]]<ref name=":0" /> | |||
* [[Endocrine Disorders|Endocrine]] factors<ref name=":5" /><ref name=":0" /> | |||
* [[Avascular Necrosis|Avascular necrosis]]<ref name=":0" /> | |||
* Metabolic factors<ref name=":5" /> | |||
Three types of trauma lead to the development of OCLs: compaction, shearing or avulsion. | |||
== Osteochondral Lesions of the Ankle == | |||
[[File:Osteochondral-injury-of-talus-staging-illustration.png|thumb|Osteochondral injuries Talus: Staging]] | |||
According to Ferkel et al.,<ref>Ferkel RD, Chams RN. Chronic lateral instability: arthroscopic findings and long-term results. Foot Ankle Int. 2007 Jan;28(1):24-31.</ref> a high percentage of patients with lateral [[Chronic Ankle Instability|ankle instability]] develop intra-articular pathology. In the [[Ankle and Foot|ankle joint]], OCLs occur in the [[talus]]. Lesions of the talar cartilage (OCT) and subchondral bone can lead to a partial or complete detachment of the fragment. OCLs can be characterised as: | |||
* | * Chondral (cartilage only) | ||
* | * Chondral-subchondral (cartilage and bone) | ||
* Subchondral (intact overlying cartilage) | |||
* | * Cystic | ||
* | * Stable or unstable | ||
* | * Non-displaced or displaced | ||
* | |||
== Osteochondral | === Classification System for Osteochondral Lesions of the Talar Cartilage === | ||
The following classification systems for OCT are used primary for research. Clinically the most important factors are lesion location and depth. In general, the bigger the lesion, the more problematic it becomes.<ref name=":6" /> | |||
* The Berndt and Harty<ref>Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959 Sep;41-A:988-1020.</ref> classification system remains the most commonly used system to stage radiographic OCTs. This system is as follows:<ref name=":1">Badekas T, Takvorian M, Souras N. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3764304/ Treatment principles for osteochondral lesions in foot and ankle]. Int Orthop. 2013 Sep;37(9):1697-706. </ref> | |||
** Stage I: with the foot in an inverted position, the lateral border is compressed against the face of the fibula, and the collateral ligament remains intact | |||
** Stage II: with progressive foot inversion, the lateral ligament is ruptured, and avulsion of the chip begins | |||
In | |||
* Berndt and Harty<ref> | |||
** Stage I: with the foot in an inverted position, the lateral border is compressed against the face of the fibula, and the collateral ligament remains intact | |||
** Stage II: with progressive foot inversion, the lateral ligament is ruptured, and | |||
** Stage III: the chip is fully detached but remains in place | ** Stage III: the chip is fully detached but remains in place | ||
** Stage IV: displacement of a detached fragment following inversion | ** Stage IV: displacement of a detached fragment occurs following inversion | ||
* Loomer et al.<ref>Loomer R, Fisher C, Lloyd-Smith R, Sisler J, Cooney T. Osteochondral lesions of the talus. Am J Sports Med. 1993 Jan-Feb;21(1):13-9. </ref> added a | * Loomer et al.<ref>Loomer R, Fisher C, Lloyd-Smith R, Sisler J, Cooney T. Osteochondral lesions of the talus. Am J Sports Med. 1993 Jan-Feb;21(1):13-9. </ref> added a fifth stage to the Berndt and Harty classification system:<ref name=":1" /> | ||
** Stage I -IV as<nowiki/> above | ** Stage I -IV as<nowiki/> above | ||
** Stage V: the p<nowiki/>resence of a subchondral cyst | ** Stage V: the p<nowiki/>resence of a subchondral cyst | ||
* Ferkel | * Ferkel et al.<ref>Ferkel RD, Sgaglione NA, DelPizzo W. Arthroscopic treatment of osteochondral lesions of the talus: long-term results. Orthop Trans. 1990;14:172–173.</ref> developed a classification system based on computed tomography (CT):<ref name=":2">Elghawy AA, Sesin C, Rosselli M. [https://bmjopensem.bmj.com/content/4/1/e000318 Osteochondral defects of the talus with a focus on platelet-rich plasma as a potential treatment option: a review.] BMJ Open Sport Exerc Med. 2018 Feb 1;4(1):e000318. </ref> | ||
** Stage I: Cystic lesion with the dome of the talus (intact roof) | ** Stage I: Cystic lesion with the dome of the talus (intact roof) | ||
** Stage IIa: Cystic lesion with communication to the talar dome surface | ** Stage IIa: Cystic lesion with communication to the talar dome surface | ||
** Stage IIb: | ** Stage IIb: An open articular surface lesion with an overlying undisplaced fragment | ||
** Stage III: | ** Stage III: An undisplaced lesion with lucency | ||
** Stage IV: Displaced fragment | ** Stage IV: Displaced fragment | ||
* Hepple et al.<ref>Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: a revised classification. Foot Ankle Int. 1999 Dec;20(12):789-93.</ref> developed a classification system based on magnetic resonance imaging (MRI). <ref name=":2" /> | * Hepple et al.<ref>Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: a revised classification. Foot Ankle Int. 1999 Dec;20(12):789-93.</ref> developed a classification system based on magnetic resonance imaging (MRI).<ref name=":2" /> | ||
[[File:OCL MRI classification.png|center|thumb|500x500px|<small>MRI classification of OCL. Adapted from | [[File:OCL MRI classification.png|center|thumb|500x500px|<small>MRI classification of OCL. Adapted from AA, Sesin C, Rosselli M. Osteochondral defects of the talus with a focus on platelet-rich plasma as a potential treatment option: a review. BMJ Open Sport Exerc Med. 2018 Feb 1;4(1):e000318.</small> ]] | ||
== Clinical Presentation == | == Clinical Presentation == | ||
Patients with | Patients with ankle osteochondral lesions will report deep ankle pain associated with weight-bearing, limitations in range of motion, impaired function, stiffness, and a feeling of catching and locking. In addition, the patient may experience tenderness and swelling around the medial and lateral ankle.<ref name=":5" /> Examination often reveals range of motion restrictions in the subtalar and talonavicular joints, impaired ligamentous ankle stability and hindfoot malalignment.<ref name=":1" /> <ref name=":5" /> | ||
== Diagnostic Procedures == | == Diagnostic Procedures == | ||
* AP and lateral | * [[X-Rays|X-ray]] - anteroposterior (AP) and lateral views completed in a weight-bearing position<ref name=":5" /> | ||
* MRI captures the integrity of soft tissue and subchondral cancellous bone | * [[MRI Scans|MRI]] captures the integrity of soft tissue and subchondral cancellous bone<ref>Sophia Fox AJ, Bedi A, Rodeo SA. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3445147/ The basic science of articular cartilage: structure, composition, and function. Sports Health]. 2009 Nov;1(6):461-8. </ref> | ||
* CT | * [[CT Scans|CT]] offers a better resolution to show bony pathologies but provides less information on the soft tissues and articular cartilage wear<ref name=":5" /> | ||
* SPECT CT | * SPECT CT is able to provide information from both MRI and CT; it is important to consider the amount of radiation a patient is exposed to with SPECT CT<ref name=":5" /> | ||
* Ankle arthroscopy allows for direct visualisation of the entire joint | * Ankle arthroscopy allows for direct visualisation of the entire joint<ref name=":5" /> | ||
== Outcome Measures == | == Outcome Measures == | ||
| Line 105: | Line 105: | ||
=== General principles in rehabilitation management === | === General principles in rehabilitation management === | ||
There is a lack of high-quality evidence for a specific treatment protocol | There is a lack of high-quality evidence for a specific treatment protocol to manage osteochondral lesions of the ankle.<ref name=":6">Simpson H. Osteochondral Lesions Course. Plus2022</ref> Therefore, when establishing goals, planning treatment and choosing interventions, the clinician must consider the biological phases of healing. Rehabilitation will also depend on the size of the lesion and its location. In general, the rehabilitation programme should:<ref name=":6" /> | ||
* Be comprehensive and include multi-modal functional training | * Be comprehensive and include multi-modal functional training | ||
* Include a minimum of six weeks of supervised rehabilitation training | * Include a minimum of six weeks of supervised rehabilitation training | ||
* Address postural control, balance and proprioception retraining | * Address postural control, [[Balance Training|balance]] and [[proprioception]] retraining | ||
* Incorporate the entire kinetic chain to improve overall strength | * Incorporate the entire [[Kinetic Chain|kinetic chain]] to improve overall [[Strength Training|strength]] | ||
* Include activities to maintain | * Include activities to maintain [[Range of Motion|range of movement]] | ||
* Include measures to protect the ankle joint by making the patient wear a lace-up brace | * Include measures to protect the ankle joint by making the patient wear a lace-up brace | ||
* Continue to monitor the patient for an unexplained increase in pain for up to 2 years | * Continue to monitor the patient for an unexplained increase in pain for up to 2 years | ||
=== Special Concerns === | === Special Concerns === | ||
When managing osteochondral lesions of the ankle, it is important to apply the following rehabilitation considerations:<ref name=":6" /> | |||
# '''Avoid shear forces''' | # '''Avoid shear forces''' | ||
# '''Avoid | # '''Avoid compressive forces''' | ||
# '''Adequate pacing of the activities due to slow recovery''' | # '''Adequate pacing of the activities due to slow recovery''' | ||
# '''Monitor pain''' | # '''Monitor pain''' | ||
# '''Prevent the development of | # '''Prevent the development of compensatory movements''' | ||
==== Shear forces ==== | ==== Shear forces ==== | ||
Shear forces are often the underlying cause of | Shear forces are often the underlying cause of OCLs in chronic ankle instability. <blockquote>Avoid shear forces for over three months.<ref name=":6" /> </blockquote> | ||
==== Compressive forces ==== | ==== Compressive forces ==== | ||
Fibrocartilage is not as strong as hyaline cartilage.<blockquote>Delay full weight bearing for as long as six weeks, based on specific clinical factors.<ref name=":6" /></blockquote> | Fibrocartilage is not as strong as hyaline cartilage.<blockquote>Delay full [[weight bearing]] for as long as six weeks, based on specific clinical factors.<ref name=":6" /></blockquote> | ||
==== Slow Recovery ==== | ==== Slow Recovery ==== | ||
| Line 133: | Line 133: | ||
==== Monitor pain ==== | ==== Monitor pain ==== | ||
<blockquote>Individualise treatment and respect patient's pain. <ref name=":6" /></blockquote> | <blockquote>Individualise treatment and respect the patient's [[Pain Assessment|pain]].<ref name=":6" /></blockquote> | ||
==== Compensatory movements ==== | ==== Compensatory movements ==== | ||
<blockquote>Correct faulty motor patterns. <ref name=":6" /></blockquote> | <blockquote>Correct faulty motor patterns.<ref name=":6" /></blockquote> | ||
=== Ankle Osteochondral Lesions Treatment Strategies<ref name=":6" /> === | === Ankle Osteochondral Lesions Treatment Strategies<ref name=":6" /> === | ||
| Line 143: | Line 143: | ||
* Take it EASY | * Take it EASY | ||
* Move the talocrural joints, but DO NOT | * Move the talocrural joints, but DO NOT expose to compressive or shear forces | ||
* Incorporate cardiovascular fitness | * Incorporate cardiovascular fitness | ||
* Maintain partial weight bearing | * Maintain partial weight bearing | ||
Examples of exercises: | Examples of exercises: | ||
<gallery widths="250" heights="350"> | |||
File:OCL stage 1.png| Gentle ankle dorsiflexion and plantarflexion exercises | |||
File:OCL.png| Lower extremities exercises in partial weight bearing and proper alignment | |||
</gallery> | |||
==== Stage 2 ==== | ==== Stage 2 ==== | ||
| Line 155: | Line 160: | ||
* Focus on details | * Focus on details | ||
* Progress from partial to full weight bearing and standing on two feet | * Progress from partial to full weight bearing and standing on two feet | ||
* Progress | * Progress the load and complexity of the movement | ||
Example of exercises: | |||
<gallery widths="250" heights="350"> | |||
File:Phase 2 OCL.png| Progression to full weight bearing with proper alignment | |||
</gallery> | |||
==== Stage 3 ==== | ==== Stage 3 ==== | ||
| Line 163: | Line 172: | ||
* Fitness activities | * Fitness activities | ||
Examples of exercises:<blockquote>''Before proceeding to stage 4 patient must:'' | Examples of exercises: | ||
<gallery widths="250" heights="350"> | |||
File:Phase 3 OCL.png| Exercises based on SEBT | |||
File:Phase III ocl.png| Fitness activities: step down/step up | |||
</gallery> | |||
<blockquote>''Before proceeding to stage 4, a patient must:'' | |||
* ''Receive good scores on Star Excursion Balance Test(SEBT)'' | * ''Receive good scores on their [[Star Excursion Balance Test|Star Excursion Balance Test (SEBT)]]'' | ||
* ''Have pain-free full range of loaded dorsiflexion'' | * ''Have pain-free full range of loaded dorsiflexion'' | ||
* ''Perform a single hop test without pain and in good alignment'' | * ''Perform a single hop test without pain and in good alignment'' | ||
* '' | * ''Demonstrate reasonable motor control in posterior medial movement'' | ||
</blockquote> | </blockquote> | ||
==== Stage 4 ==== | ==== Stage 4 ==== | ||
* Plyometrics | * [https://blog.nasm.org/fitness/developing-power-in-everyday-athletes-with-plyometrics Plyometrics] | ||
== Resources == | == Resources == | ||
| Line 187: | Line 203: | ||
[[Category:Ankle - Interventions]] | [[Category:Ankle - Interventions]] | ||
[[Category:Course Pages]] | [[Category:Course Pages]] | ||
[[Category: | [[Category:Plus Content]] | ||
Latest revision as of 22:47, 25 January 2023
Definitions[edit | edit source]

Cartilage is a connective tissue which has the following components:[1]
- Polysaccharides (a cellular component composed of ground substance)
- Fibrous proteins
- Interstitial fluid with water as the main component
Cartilage gets its nutrition via diffusion from surrounding tissues as it has no direct blood supply, lymphatics or nerves.[1]
There are three types of cartilaginous tissues: hyaline, fibrocartilage and elastic cartilage.[1] Each type of cartilaginous tissue has a different composition and function:
- Hyaline cartilage: is a connective tissue located at the ends of bones. Its primary cells are chondrocytes. Their role is to maintain the cartilage extracellular matrix (ECM), which is responsible for the biological and mechanical function of the cartilage. Hyaline cartilage ECM contains:[2]
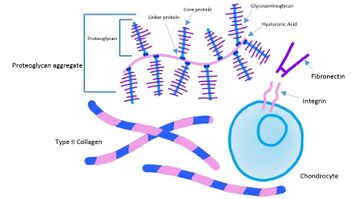
- Type II collagen (10-20%)
- Proteoglycan (1-10%)
- Water (65-85%)
- Fibrocartilage is a "transitional tissue between hyaline cartilage and dense regular connective tissue."[1] This type of tissue can be found in the pubic symphysis, the annulus fibrosus of intervertebral disc, tendons, and ligaments.[3] It contains:[1]
- High levels of type I collagen
- Type II collagen
- A small component of ground substance
- Elastic cartilage: is a flexible connective tissue cartilage that can withstand repeated bending.[1] It consists of:[1]
- Type II collagen
- Elastic fibres
- Large chondrocytes

Subchondral bone is located below the hyaline cartilage and cement line (i.e. the border between calcified cartilage and the subchondral bone[4]). It is responsible for providing mechanical (including shock absorption) and nutritional support for cartilage (the subchondral bone containing vessels that directly interact with the hyaline cartilage layer)[5]. The perfusion mechanism of the subchondral bone vessels is responsible for distributing 50% of nutrients to the cartilage.[6]
Osteochondral lesions (OCL) are defects affecting the structure of the cartilaginous surface and underlying subchondral bone. When the lesion's healing phase begins and tissue forms, the new tissue is often fibrocartilage. However, this type of cartilage has mechanical disadvantages to hyaline cartilage. In some cases, hyaline cartilage forms during the repair process, but the mechanism of hyaline vs fibrocartilage formation is unknown.[1]
Healing of Osteochondral Lesions[edit | edit source]
Osteochondral lesions have poor healing capacity.[7] A study completed in animals[8] demonstrates that OCLs go through the following stages of healing:[7]
- Week 1-2: Initial fibrin repair - the damaged site begins to fill with a blood clot and fibrous tissue, mesenchymal cell recruitment begins
- Week 4-8: Cartilage formation starts adjacent to the damaged cartilage
- Weeks 8 -12: Bone formation begins through endochondral ossification
- Week 18: New bone formation continues
- Week 26: Completion of the healing process
Aetiology of Osteochondral Lesions[edit | edit source]
Osteochondral lesions can be caused by:
- Trauma (80% of cases)[9]
- Joint malalignment[10]
- Ligament laxity (38% of patients)[9]
- Instability (39% of patients)[9]
- Genetic predisposition[10]
- Endocrine factors[9][10]
- Avascular necrosis[10]
- Metabolic factors[9]
Three types of trauma lead to the development of OCLs: compaction, shearing or avulsion.
Osteochondral Lesions of the Ankle[edit | edit source]

According to Ferkel et al.,[11] a high percentage of patients with lateral ankle instability develop intra-articular pathology. In the ankle joint, OCLs occur in the talus. Lesions of the talar cartilage (OCT) and subchondral bone can lead to a partial or complete detachment of the fragment. OCLs can be characterised as:
- Chondral (cartilage only)
- Chondral-subchondral (cartilage and bone)
- Subchondral (intact overlying cartilage)
- Cystic
- Stable or unstable
- Non-displaced or displaced
Classification System for Osteochondral Lesions of the Talar Cartilage[edit | edit source]
The following classification systems for OCT are used primary for research. Clinically the most important factors are lesion location and depth. In general, the bigger the lesion, the more problematic it becomes.[12]
- The Berndt and Harty[13] classification system remains the most commonly used system to stage radiographic OCTs. This system is as follows:[14]
- Stage I: with the foot in an inverted position, the lateral border is compressed against the face of the fibula, and the collateral ligament remains intact
- Stage II: with progressive foot inversion, the lateral ligament is ruptured, and avulsion of the chip begins
- Stage III: the chip is fully detached but remains in place
- Stage IV: displacement of a detached fragment occurs following inversion
- Loomer et al.[15] added a fifth stage to the Berndt and Harty classification system:[14]
- Stage I -IV as above
- Stage V: the presence of a subchondral cyst
- Ferkel et al.[16] developed a classification system based on computed tomography (CT):[17]
- Stage I: Cystic lesion with the dome of the talus (intact roof)
- Stage IIa: Cystic lesion with communication to the talar dome surface
- Stage IIb: An open articular surface lesion with an overlying undisplaced fragment
- Stage III: An undisplaced lesion with lucency
- Stage IV: Displaced fragment

Clinical Presentation[edit | edit source]
Patients with ankle osteochondral lesions will report deep ankle pain associated with weight-bearing, limitations in range of motion, impaired function, stiffness, and a feeling of catching and locking. In addition, the patient may experience tenderness and swelling around the medial and lateral ankle.[9] Examination often reveals range of motion restrictions in the subtalar and talonavicular joints, impaired ligamentous ankle stability and hindfoot malalignment.[14] [9]
Diagnostic Procedures[edit | edit source]
- X-ray - anteroposterior (AP) and lateral views completed in a weight-bearing position[9]
- MRI captures the integrity of soft tissue and subchondral cancellous bone[19]
- CT offers a better resolution to show bony pathologies but provides less information on the soft tissues and articular cartilage wear[9]
- SPECT CT is able to provide information from both MRI and CT; it is important to consider the amount of radiation a patient is exposed to with SPECT CT[9]
- Ankle arthroscopy allows for direct visualisation of the entire joint[9]
Outcome Measures[edit | edit source]
- Lower Extremity Functional Scale (LEFS)
- Foot and Ankle Ability Measure (FAAM)
- The Foot & Ankle Disability Index Score (FADI)
- Foot Function Index (FFI)
Comprehensive Rehabilitation[edit | edit source]
General principles in rehabilitation management[edit | edit source]
There is a lack of high-quality evidence for a specific treatment protocol to manage osteochondral lesions of the ankle.[12] Therefore, when establishing goals, planning treatment and choosing interventions, the clinician must consider the biological phases of healing. Rehabilitation will also depend on the size of the lesion and its location. In general, the rehabilitation programme should:[12]
- Be comprehensive and include multi-modal functional training
- Include a minimum of six weeks of supervised rehabilitation training
- Address postural control, balance and proprioception retraining
- Incorporate the entire kinetic chain to improve overall strength
- Include activities to maintain range of movement
- Include measures to protect the ankle joint by making the patient wear a lace-up brace
- Continue to monitor the patient for an unexplained increase in pain for up to 2 years
Special Concerns[edit | edit source]
When managing osteochondral lesions of the ankle, it is important to apply the following rehabilitation considerations:[12]
- Avoid shear forces
- Avoid compressive forces
- Adequate pacing of the activities due to slow recovery
- Monitor pain
- Prevent the development of compensatory movements
Shear forces[edit | edit source]
Shear forces are often the underlying cause of OCLs in chronic ankle instability.
Avoid shear forces for over three months.[12]
Compressive forces[edit | edit source]
Fibrocartilage is not as strong as hyaline cartilage.
Delay full weight bearing for as long as six weeks, based on specific clinical factors.[12]
Slow Recovery[edit | edit source]
Repair of cartilage takes time.
Take it easy with steps 1 and 2 and maintain partial weight bearing.[12]
Monitor pain[edit | edit source]
Compensatory movements[edit | edit source]
Correct faulty motor patterns.[12]
Ankle Osteochondral Lesions Treatment Strategies[12][edit | edit source]
Stage 1[edit | edit source]
- Take it EASY
- Move the talocrural joints, but DO NOT expose to compressive or shear forces
- Incorporate cardiovascular fitness
- Maintain partial weight bearing
Examples of exercises:

Gentle ankle dorsiflexion and plantarflexion exercises

Lower extremities exercises in partial weight bearing and proper alignment


Stage 2[edit | edit source]
- This phase focuses on function
- It is considered a pre-participation phase
- Focus on details
- Progress from partial to full weight bearing and standing on two feet
- Progress the load and complexity of the movement
Example of exercises:

Progression to full weight bearing with proper alignment

Stage 3[edit | edit source]
- Fitness activities
Examples of exercises:
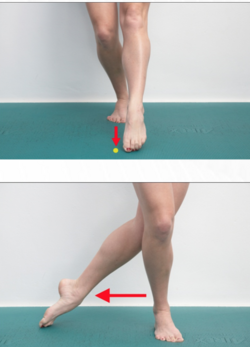
Exercises based on SEBT

Fitness activities: step down/step up


Before proceeding to stage 4, a patient must:
- Receive good scores on their Star Excursion Balance Test (SEBT)
- Have pain-free full range of loaded dorsiflexion
- Perform a single hop test without pain and in good alignment
- Demonstrate reasonable motor control in posterior medial movement
Stage 4[edit | edit source]
Resources[edit | edit source]
- Saccomanni B. Osteochondral Lesions of Talus: A Comprehensive Review. Mathews J Orthop. 2018; 3(1): 021.
- Hannon CP, Smyth NA, Murawski CD, Savage-Elliott I, Deyer TW, Calder JD, Kennedy JG. Osteochondral lesions of the talus: aspects of current management. Bone Joint J. 2014 Feb;96-B(2):164-71.
References[edit | edit source]
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 1.7 Armiento AR, Alini M, Stoddart MJ. Articular fibrocartilage - Why does hyaline cartilage fail to repair? Adv Drug Deliv Rev. 2019 Jun;146:289-305.
- ↑ Lakin BA, Snyder BD, Grinstaff MW. Assessing cartilage biomechanical properties: techniques for evaluating the functional performance of cartilage in health and disease. Annual review of biomedical engineering. 2017 Jun 21;19:27-55.
- ↑ Donahue RP, Gonzalez-Leon EA, Hu JC, Athanasiou K. Considerations for translation of tissue engineered fibrocartilage from bench to bedside. J Biomech Eng. 2018 Dec 5;141(7):0708021–07080216.
- ↑ Li G, Yin J, Gao J, Cheng TS, Pavlos NJ, Zhang C, et al. Subchondral bone in osteoarthritis: insight into risk factors and microstructural changes. Arthritis Res Ther. 2013;15(6):223.
- ↑ Hu Y, Chen X, Wang S, Jing Y, Su J. Subchondral bone microenvironment in osteoarthritis and pain. Bone research. 2021 Mar 17;9(1):1-3.
- ↑ Imhof H, Sulzbacher I, Grampp S, Czerny C, Youssefzadeh S, Kainberger F. Subchondral bone and cartilage disease: a rediscovered functional unit. Investigative radiology. 2000 Oct 1;35(10):581-8.
- ↑ 7.0 7.1 Lydon H, Getgood A, Henson FMD. Healing of Osteochondral Defects via Endochondral Ossification in an Ovine Model. Cartilage. 2019 Jan;10(1):94-101.
- ↑ Shapiro F, Koide S, Glimcher MJ. Cell origin and differentiation in the repair of full-thickness defects of articular cartilage. J Bone Joint Surg Am. 1993 Apr;75(4):532-53.
- ↑ 9.00 9.01 9.02 9.03 9.04 9.05 9.06 9.07 9.08 9.09 9.10 Krause F, Anwander H. Osteochondral lesion of the talus: still a problem?. EFORT open reviews. 2022 Jun 1;7(6):337-43.
- ↑ 10.0 10.1 10.2 10.3 Mosca M, Grassi A, Caravelli S. Osteochondral Lesions of Ankle and Knee. Will Future Treatments Really Be Represented by Custom-Made Metal Implants?. Journal of Clinical Medicine. 2022 Jul 1;11(13):3817.
- ↑ Ferkel RD, Chams RN. Chronic lateral instability: arthroscopic findings and long-term results. Foot Ankle Int. 2007 Jan;28(1):24-31.
- ↑ 12.0 12.1 12.2 12.3 12.4 12.5 12.6 12.7 12.8 12.9 Simpson H. Osteochondral Lesions Course. Plus2022
- ↑ Berndt AL, Harty M. Transchondral fractures (osteochondritis dissecans) of the talus. J Bone Joint Surg Am. 1959 Sep;41-A:988-1020.
- ↑ 14.0 14.1 14.2 Badekas T, Takvorian M, Souras N. Treatment principles for osteochondral lesions in foot and ankle. Int Orthop. 2013 Sep;37(9):1697-706.
- ↑ Loomer R, Fisher C, Lloyd-Smith R, Sisler J, Cooney T. Osteochondral lesions of the talus. Am J Sports Med. 1993 Jan-Feb;21(1):13-9.
- ↑ Ferkel RD, Sgaglione NA, DelPizzo W. Arthroscopic treatment of osteochondral lesions of the talus: long-term results. Orthop Trans. 1990;14:172–173.
- ↑ 17.0 17.1 Elghawy AA, Sesin C, Rosselli M. Osteochondral defects of the talus with a focus on platelet-rich plasma as a potential treatment option: a review. BMJ Open Sport Exerc Med. 2018 Feb 1;4(1):e000318.
- ↑ Hepple S, Winson IG, Glew D. Osteochondral lesions of the talus: a revised classification. Foot Ankle Int. 1999 Dec;20(12):789-93.
- ↑ Sophia Fox AJ, Bedi A, Rodeo SA. The basic science of articular cartilage: structure, composition, and function. Sports Health. 2009 Nov;1(6):461-8.

