The Effectiveness of Core Stability Exercise in the Management of Chronic Non-Specific Low Back Pain
Original Editor - .... as part of the <a _fcknotitle="true" href="Nottingham University Spinal Rehabilitation Project">Nottingham University Spinal Rehabilitation Project</a>
Top Contributors - <img _fck_mw_template="true" _fckrealelement="0" _fckfakelement="true" src="http://www.physio-pedia.com/extensions/FCKeditor/fckeditor/editor/images/spacer.gif" class="FCK__MWTemplate">
Chronic Low Back Pain[edit | edit source]
Low back pain is an extremely common patient complaint with approximately 80% of the World population developing low back pain at some point (Deyo 2001). It is the main cause of years lived with disability (Vos 2012). It is among 10 of the leading reasons for patient visits to medical facilities. (Patel 2000). Most cases resolve fairly quickly, but a significant number of patients develop chronic Lower Back Pain. Patients experience unremitting pain and often become functionally impaired. Chronic LBP represents a greater financial burden in the form of direct costs resulting from loss of work and medical expenses, as well as indirect costs (Dagenais 2008). Most patients on disability for more than 6 months will not return to work. The number of patients returning to work approaches zero at 2 years (Anderson 1997).
Mechanical disorders are the cause in 90% of cases with the remaining 10% of cases being due to manifestation of systemic illness (Nachemson, 1976). Despite the large number of pathological conditions that give rise to low back pain cases 85% are without patho-anotomical or radiological abnormalities (Deyo 2001). Most episodes of low back pain resolve quickly and are not incapacitating, nonetheless pain and disability are often ongoing and recurrences are common (Pengel 2003). It is estimated 10% to 20% of effected adults develop symptoms of chronic low back.
Generally there is a scarcity of information on the prevalence and incidence of CLBP, partly due to lack of agreement about it’s definition. Chronic low back pain is mostly defined as persistent pain occurring on most days and lasting longer than 3 months (Maher 2004;Von Korff 1996; Waddell 2004) Others also define it as pain exceeding normal healing times and frequently reoccurring back pain over long periods. Acute and chronic LBP warrant separate consideration as they may respond differently to the same interventions. (Sierpina 2002; van Tulder 1999)
Core Stability[edit | edit source]
Definition
[edit | edit source]
Many authors have attempted to define core stability, which consequently means a globally accepted definition is yet to be confirmed ( Huxel –Bliven and Anderson 2013). However, a widely accepted definition of core stability is:
“Comprises of the lumbopelvic-hip complex and is the capacity to maintain equilibrium of the vertebral column within its physiologic limits
by reducing displacement from perturbations and maintaining structural integrity.”
(AKUTHOTA, NADLER 2004, LIEMOHN, BAUMGARTNER, GAGNON 2005, PANJABI 2003, PANJABI 1992, SMITH, NYLAND, CAUDILL, BROSKY, CABORN 2008, WILLSON, DOUGHERTY, IRELAND, DAVIS 2005)
History[edit | edit source]
The first acknowledgment of core stability was by Henry and Florence Kendall who were both Physiotherapist's and first developed the idea of a “neutral pelvis” in 1940/1950’s (Kent 2012).
They initially suggested that the surrounding superficial muscle groups were responsible for the maintenance of alignment and of “neutral spine” . The muscles they were referring to were the erector spinae, hamstrings, abdominals and the hip flexors. Following on from this, it was suggested that pelvic tilt was pelvic movement deviating from the neutral position.
Paul Hodges has furthered the research into core stability and has highlighted the significance and contribution of the Transverus Abdominus muscle, especialy in lumbo pelvic stability. Upon this basis, it has now become and important part in the management of spinal stability (Hodges 1999).
Exercises orientated upon the activation, recruitment and strengthening the core muscles are extremely prevalent in modern day practice.
Theories[edit | edit source]
In attempt to add some clarity to the phenomena of spinal stability, Panjabi proposed a classification model which helped explain core stability. His model consisted of three categories, Active, Passive and Neural.
Passive[edit | edit source]
The passive category consists of the basic components of the spine which allow for soft tissue attachment. REF
• The lumbar vertebrae
• The joint capsules
• The intervertebral disc
• Ligaments surrounding the area
These structures of the spine do not contribute to any significant spinal stability in the neutral alignment. The skeletal structure does support the basic framework and the tensile properties in the various ligaments do start to resist end range movement, however do not have the capability to produce forces which initiate spinal movement is not caused by the passive structures.
Active[edit | edit source]
The active structures hold responsibility for the initiation of gross spinal movement as well as providing contributing to spinal segmentation.
Bergmark (1989) further classified the active system into the local and global stabilising system.
The local globalising system was slated to have a primary role in the mainatancence of spinal segement stability and stiffness.
The Global stabilising system was stated to be more superficial and with a primary function to generate force to control movement, there is often eccentric contractions to control motion segments throughout range
Global mobilisers[edit | edit source]
A further active functional classification was suggested by Comerford and Mottram (2001). They have proposed the idea of “global mobilisers”. The primary role of these muscles is for shock absorption and to generate the gross spinal concentric contractions required for gross motor function.
Neural[edit | edit source]
The neural component, according to Punjabi, is responsible for recieving information from the various transducers and relaying the relative signal onto the active system to achieve segmental stability. Until sufficient stability has been achieved, the neural components continue to control the active systems.
Figure 1. [edit | edit source]
A model showing the relationship between the three models proposed by Punjabi (1992), Comerford and Mottram's (2000) and Bergmark (1989), which influecne "spinal stability".

Figure 2.[edit | edit source]
A table proposed by Norris (2008), identifying the different characteristics between the stablisers and mobilisers.

(Norris 2008)
Relevant anatomy
[edit | edit source]
(Kibler, Press and Sciascia 2006)
<img src="/images/8/83/Spinal_assessment_3.png" _fck_mw_filename="Spinal assessment 3.png" alt="" />
<img src="/images/e/e8/Spinal_assessment_4.png" _fck_mw_filename="Spinal assessment 4.png" alt="" />
Physiology[edit | edit source]
PICTUE TO BE PUT IN OF A PRIME MOVER MUSCLE – MOSEY DOINT A TENNIS SERVE OR SOMETHING
Due to many superficial muscles attaching to the Core, intrinsic muscles have a role in gross superficial movements. It has been stated that core is characterised by “Proximal stability for distal mobility” (Putnam 1993, Zattara and Bouisset 1988)
When contracting, the primary role of the core stability muscles is to raise the intra-abdominal pressure and to increase the tension in the thoracolumbar fascia. The increase in intra-abdominal pressure stiffens and strengthens the relevant structural support around the spine and compacts the arthrogenic structures (McGill and Norman 1987).
This gives the spine a relative degree of stability which is needed to facilitate superficial muscle activation and gross motor action.
Core stability functions[edit | edit source]
• Anticipatory postural adjustments – pre-programmed muscle activation which helps the body to anticipate the subsequent force
• To create interactive moments that help to control the exposure of force and loading that is applied to a joint (Kibler, Press and Sciascia 2006)
• To help in force control and shared up
Typical core exercises[edit | edit source]
A lumbo-pelivic stability programme is constructed in three sections. The frist section is Segmental control over primary stabilizers (mainly TrA, deep multifidus, pelvic floor and diaphragm), moving onto exercises in closed chain, with low velocity and low load, progressing onto exercises in open chain, with high velocity and load (Richardson, Hodges and Hides (2004).
Some of the exercises listed below have been proven to significantly increase scores relating to were general health (SF-12) and sports functioning, with a significant decrease in pain.
(GLADWELL , HEAD, HAGGAR and BENEKE (2006)
Phase 2[edit | edit source]
Bridging
Single leg fall out
Single leg extension in supine
Basic 4 point Kneeling
Advanced 4 point Kneeling
The modified one leg stretch: Crook lying, slide one leg away as far as possible and then return to start position.
The modified shoulder bridge: Crook lying, “peeling” the bottom off the mat. Progression: Increase the range of movement (more of the spine away from the mat).
Swimming (a modification from a four point base): Box position, slide one foot along the floor behind, return to the start position. Repeat on other leg.
Phase 3.[edit | edit source]
Bridging progression onto a pilates ball
Pilates ball plank
Recent Evidence[edit | edit source]
This chapter will look at the evidence supporting/ambiguity of core stability versus general exercise for chronic low back pain. These papers needed to include pain and disability as outcome measures to show whether core stability had any significant effect.
Evidence For
[edit | edit source]
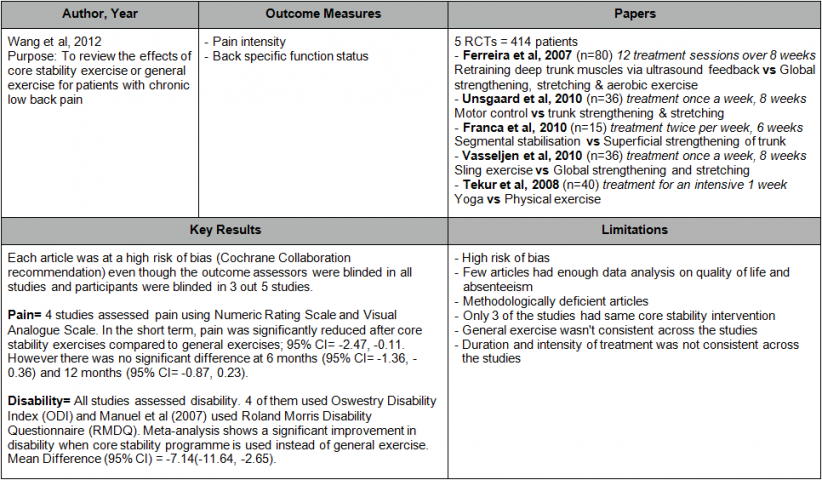
[edit | edit source]

Evidence Against[edit | edit source]
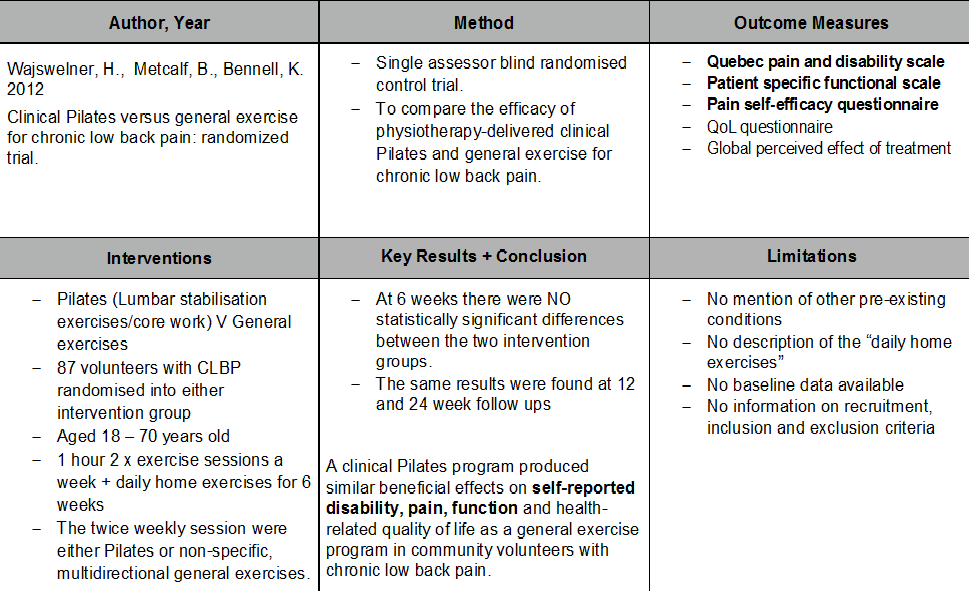
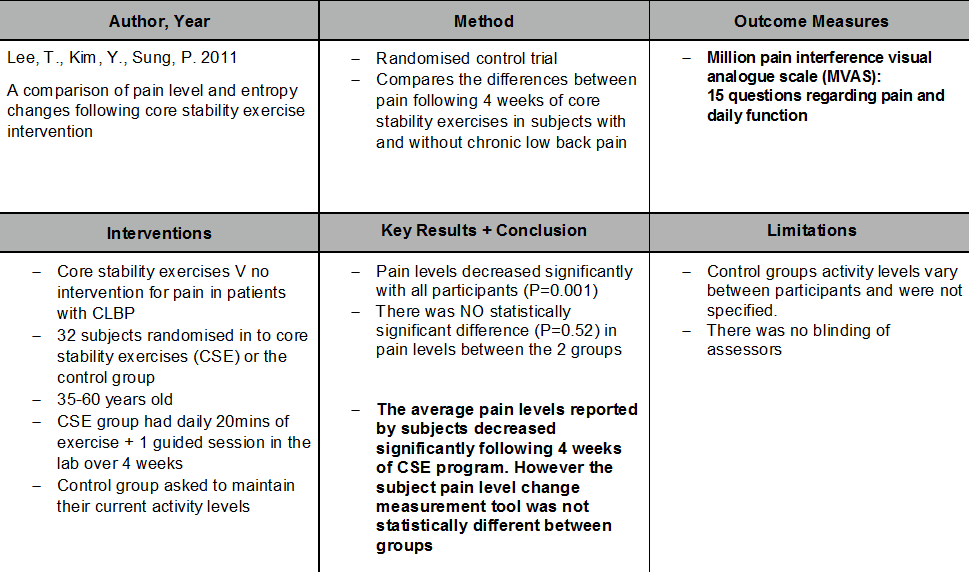 [edit | edit source]
[edit | edit source]


References[edit | edit source]
References will automatically be added here, see <a href="Adding References">adding references tutorial</a>.
<span class="fck_mw_references" _fck_mw_customtag="true" _fck_mw_tagname="references" />


{kind=link}