Telerehabilitation and Smartphone Apps in Physiotherapy
Original Editor - Oriana Catenazzi, Alicia Rebellato, Hannah Meredith, Aaron Kirk, Martin Fitheridge, Marco Zavagni
Introduction to Telerehabilitation and smartphone physiotherapy applications
[edit | edit source]
add text here relating to introduction
Learning Outcomes
[edit | edit source]
add text here relating to the learning outcomes
Table of Contents [edit | edit source]
add text here relating to the table of contents
Overview of Telerehabilitation[edit | edit source]
add text here relating to diagnostic tests for the condition
Telerehabilitation[edit | edit source]
Progression of technology[edit | edit source]
Applications for specific conditions[edit | edit source]
Scotlands Telehealth and Telecare delivery plan[edit | edit source]
The patient perspective on telerehabilitation[edit | edit source]
Key points[edit | edit source]
Understanding the patient[edit | edit source]
Introduction[edit | edit source]
Over the last decade the development and use of telehealth interventions for changing patient behaviours has greatly increased (Riley et al.2011). The use of mobile applications must take in account the physical and socio-psychological needs of health practitioners and patients. The user approaching a device, is not purely interested in what the device does, but rather how the device makes them feel: the developer must remember that the application is developed focusing on the customer and is designed to satisfy all their needs (Ruiz et al., 2012). The ability to access extensive and multifaceted programs provides health care professionals with the opportunity deliver behavioural change interventions that can be adapted to meet the patient’s characteristics, behaviours and environment (Patrick et al. 2008). In order to analyse the effectiveness of these interventions, health behaviour theories and models are used to guide the development and delivery of the intervention (Riley et al. 2011). Bandura’s Transtheoretical Model (bandura, 1982) and Self-Determination Theory (Prochaska and Velicer, 1999) have served as the basis for many health care interventions and it is important that the physiotherapist understands the underlying principles behind these theories. The use of health behaviour models and theories will assist the health care professional at the initiation stage of the intervention to meet their baseline characteristics of the patient and also during the intervention when behaviour change is taking place. To understand our patient fully it is necessary to examine their motivation, efficacy, and goals, then apply a theoretical model to our intervention.
Transtheoretical model[edit | edit source]
Self-efficacy theory[edit | edit source]
Motivation[edit | edit source]
Motivation is complex term, and has been subjected to various definitions and approaches. Csikszentmihalyi (1990) defines motivation as “a phenomenal experience being a sufficient reason for action”, which then lead Deci and Ryan (2000) to further develop its content focusing on the “functional significance of events” as the main determinant for motivation.
In Self-Determination Theory (Deci and Ryan, 1985) separate motivation into types, centred on the different goals that lead to the development of an action:
1.Intrinsic motivation, which denotes the act of doing something because it is inherently interesting or enjoyable thus leading a person to act for the fun or challenge rather than because of external prods, pressures, or rewards. Spontaneous behaviours, which confer benefits to the organism, are not completed for any instrumental reason rather than constructive experience associated with exercising and empowering one’s capacities.
2.Extrinsic motivation, which denotes the act doing something because it leads to a separable outcome: social demands and roles that require individuals to assume responsibility for non-intrinsically stimulating duties. It can be further defined into four categories:
External regulation, in which individuals perform tasks to satisfy an externally imposed demand. Introjection, in which individuals perform tasks in order to avoid guilt or anxiety or to enhance self-esteem. Identification, in which individuals identify the own importance of a behaviour, accepting its rules as his or her own. Integration, in which individuals entirely assimilate rules and regulations and those are congruent with his or her own values and needs.
3. Amotivation, which refers to the state of lacking an intention to act. Individuals who are amotivated lack intentionality and sense of personal causation due to the fact that they are not valuing an activity, not feeling competent to do it, or not believing it will lead to a desired outcome.
Motivation between individuals varies in amount, level (how much?) and orientation (what type?). Orientation of motivation refers to the essential attitudes and goals that lead to the development of a certain action (why are we doing this?). Research across various settings supports the role of communication in enhancing psychological functioning, self-regulation and intrinsic motivation.
The ideal situation is that an individual is able to self-monitor himself because he truly believes in the intervention and knows how this is intrinsically important for him/her (Teixeira et al. 2012) or because enjoyment of the activity leads to the adoption of a certain lifestyle (Cocosila et al. 2009). If neither self-consciousness or enjoyment could lead an individual to change its behaviour towards a healthier lifestyle, family encouragement and family cohesion could determine better outcomes within the rehabilitation setting (Rosland et al. 2011)
Self-determination theory[edit | edit source]
Goal setting[edit | edit source]
Clinical implications[edit | edit source]
Research[edit | edit source]
Current smartphone applications and modernization of physiotherapy
[edit | edit source]
Introduction
[edit | edit source]
Current physiotherapy applications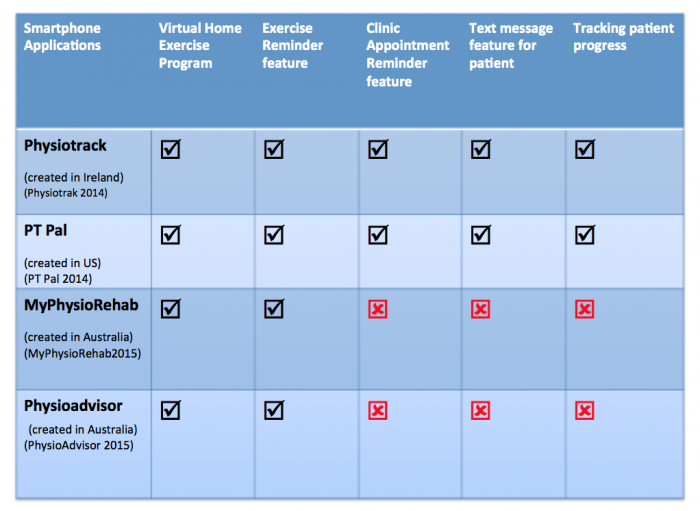 [edit | edit source]
[edit | edit source]

Further considerations: Improved communication [edit | edit source]
Facilitating patient-provider relationship[edit | edit source]
Utilising reminder services to enhance communication[edit | edit source]
Facilitating Knowledge and Education through Physiotherapist communication[edit | edit source]
Communicating the right exercise prescription[edit | edit source]
Further considerations: Facilitating behaviour change[edit | edit source]
Intrinsic and extrinsic motivation towards rehabilitation[edit | edit source]
Self-efficacy and goal setting[edit | edit source]
Cost effectiveness[edit | edit source]
Limitations
[edit | edit source]
add text here relating to the limitations
Conclusing Remarks [edit | edit source]
add text here relating to key evidence with regards to any of the above headings
CPD Test your knowledge [edit | edit source]
add appropriate resources here
References[edit | edit source]
References will automatically be added here, see adding references tutorial.

