Rhabdomyolysis
Original Editors - Students from Bellarmine University's Pathophysiology of Complex Patient Problems project.
Lead Editors - Your name will be added here if you are a lead editor on this page. Read more.
Definition/Description
[edit | edit source]
Rhabdomyolysis is the breakdown of skeletal muscle tissue that occurs quickly due to a large release of creatinine phosphokinase enzymes due to mechanical, physical, or chemical traumatic injuries.[1] Due to the quick breakdown of the skeletal muscle there is a big accumulation of the breakdown products which can cause renal failure.[1]
Historical Background[edit | edit source]
The first known report of rhabdomyolysis occurred in Sicily in 1908 after an earthquake, this was also the first case of crush syndrome as well and was found in German military literature.[2][3] [4] While this was the first report there has been some speculation that there are references in the bible about rhabdomyolysis during the Jews exodus from Egypt. It was described as a plague that occurred after a large intake of quail.[2] [4] A similar incident occurred in 1930 in the Baltic sea area where there was a large consumption of intoxicated fish.[3]
Military
The focus of rhabdomyolysis really came about during World War II, especially during the bombing that occurred in London, where crush victims developed acute renal failure.[2][3] Reports were also present during the Korean War as well as during Vietnam. During Vietnam the incidence actually decreased which is thought to be due to the faster evacuation techniques and improved fluid resuscitation to victims.[2]
Natural Disasters
As seen through history the most common incidence of rhabdomyolyisis occurs during natural disasters where there are less resources available to helped trapped victims, making their time under rubble longer increasing their chances of developing rhabdomyolysis. On August 17, 1999 in Marmara, a region of Turkey, an earthquake with a 7.4 magnitude devastated the area. This earthquake caused 17,480 deaths. Many victims were sent to hospitals, 9,843 patients were hospitalized with 425 of them dying. Of those 9,843 patients, 639 patients developed renal failure, this was 12% of the patients that were hospitalized. The victims average time spent under rubble was 11.7 hours. [2]
Collapse of World Trade Center
On September 11, 2001 in New York City the twin towers collapsed trapping many victims under rubble. Hospitals were prepared to have dialysis ready the days following the attacks to treat the many victims to prevent renal failure. Fortunately very few victims had crush injuries and only victim developed rhabdomyolysis, a 38 year-old police officer who had been trapped under rubble for 24 hours.[2]
Prevalence[edit | edit source]
Eighty-five percent of victims of traumatic injuries develop rhabdomyolysis.[2] Of those patients with rhabdomyolysis 10-50% of those patients will develop acute renal failure.[2] It is also suggested that victims of severe injury that develop rhabdomyolysis and later acute renal failure have a mortality of 20%.[2]
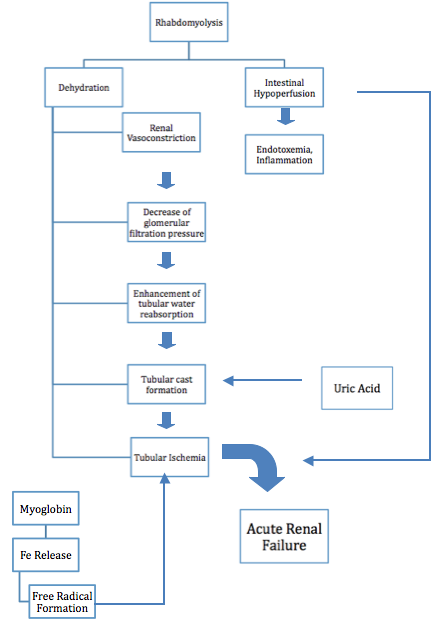 Courtesy Of: Efstratiadis G, Voulgaridou A, Nikiforou D, et al. Rhabdomyolysis updated. Hippokratia 2007; 11(3): 129-137.Pathophysiology[edit | edit source]
Courtesy Of: Efstratiadis G, Voulgaridou A, Nikiforou D, et al. Rhabdomyolysis updated. Hippokratia 2007; 11(3): 129-137.Pathophysiology[edit | edit source]

Rhabdomyolysis occurs due to injury whether it is mechanical, chemical, toxins, poisons, or burns, these injuries have a detrimental effect to the cell membranes throughout the body, When a cell membrane is damaged the breakdown or lysis releases organic and inorganic intracellular components such as potassium, myoglobin, lactic acid, purines, and phosphate which enter the circulation. Exhaustive work of cells and stretching can increase sarcoplasmic influx of sodium, chloride, and water, which can result in swelling and autodestruction.[4] After the restoration of blood flow after the injury these components become toxic to the body and in most cases are life threatening, making rhabdomyolysis a medical emergency. [3]
Myoglobin is usually filtered through glomeruli and reabsorbed in the proximal tubules by endocytosis, however when rhabdomyolysis occurs there is an excess of myoglobin, which overloads the proximal tubule cells ability to convert iron to ferritin, which then results in intracellular ferruhemate accumulation. Since iron is able to donate and except electrons as well as having the ability to generate free radicals the urine’s pH can lead to metabolic acidosis. This process puts oxidative stress and injury to the renal cells, which if untreated can lead to renal cell failure.[3]
When there is an excess of myoglobin the tubules are unable to reabsorb it.[3][4] Systemic vasoconstriction sets in which results in water reabsorption in renal tubules, which then increases myoglobin concentration in urine. This in turn causes formation of casts that obstruct renal tubules, another contributing factor of cast formation is apoptosis that occurs in epithelial cells. This obstruction causes formation of free radicals from iron, which can lead to renal failure.[3]
Potassium is another byproduct of muscle lysis.
If there is too much potassium in the circulation then hyperkalemia can occur which is life threatening, because of its cardiotoxicty effects, this is a medical emergency.[3] Cardiac arrhythmias can occur due to increased levels of potassium in the blood, in some cases early death occurs due to ventricular fibrillation.[5]
Calcium accumulation in the muscles occurs in the early stages of rhabdomyolysis. Massive calcification of necrotic muscles can occur which can lead to hypercalcemia. If hyperkalemia is present hypercalcemia can lead to cardiac arrhythmias, muscular contraction, or seizures.[4]
Causes[edit | edit source]
Causes for rhabdomyolysis can be broken down into 2 categories, hereditary causes and acquired causes.
Hereditary Causes[edit | edit source]
Those that are at risk for rhabdomyolysis have a family history of disorders dealing with carbohydrate metabolism as well as disorders of lipid metabolism. Disorders of lipid metabolism include malignant hyperthermia, mitochondrial disorders, as well as other genetic disorders.
Acquired Causes[edit | edit source]
Some of the most common acquired causes include trauma or crush injury, toxic, sever muscle exertion, seizures, shaking chills, delerium tremors, ischemia or muscle necrosis, metabolic disorders, bacterial and viral infections, heat-induced (malignant hyperthermia, heat intolerance, heat stroke), inflammatory, certain drugs (overuse or overdose) such as cocaine, amphetamines, statins, heroin, PCP, as well as low phosphate levels.
Below is a chart that describes the risk factors for rhabdomyolysis as well as examples of the risk factors and associated signs and symptoms.

Risk Factors For Postoperative Rhabdomyolysis[edit | edit source]
- Male
- Age > 10 years
- BMI > 55 kg/m2
- History of hypertension, diabetes mellitus, or peripheral vascular disease
- History of statin use
- Elevated preoperative serum CPK level
- Operation duration > 5hours
- Anesthesia time > 6 hours
- Inadequate hydration
- Urine output < 1.5ml/kg/h
- Bleeding and/or hypotension
- Use of propofol and/or succinylcholine
- Complaints of muscle pain and weakness
- Delayed ambulation
- Urine output <1.5mL/kg/h
- Serum CPK > 1,000IU/L
- Urine myoglobin > 250m g/L
Characteristics/Clinical Presentation[edit | edit source]
The signs and symptoms of rhabdomyolyis vary from person to person. The three most common signs and symptoms are muscle pain, weakness, and dark urine.[2][3] Muscle pain as well as weakness and tenderness may be general or specific to muscle groups. The calves and low back are the most general muscle groups that are affected.[2] According to the author Efstratiadis, back pain and limb pain are the most frequent sites in patients with rhabdomyolysis.[3] However, over 50% of the patients with rhabdomyolysis may not complain of muscle pain or weakness.[2] The initial sign of rhabdomyolysis is discolored urine which can range from pink to dark black.[2][3] Other signs and symptoms include, local edema, cramps, hypotension, malaise, fever, tachycardia, nausea and vomiting.[2][3] Often during the early stages of rhabdomyolysis the following conditions may also be present: hyperkalemia, hypocalcemia, elevated liver enzymes, cardiac dysrrhythmias and cardiac arrest.[2] Some late complications include acute renal failure and disseminated intravascular coagulation.[2]
Associated Co-morbidities[edit | edit source]
add text here
Diagnostic Tests/Lab Tests/Lab Values[edit | edit source]
from the patient to look at various serum values, one of the most important serum indicators of myocyte injury is creatinine kinase.[3]
Creatinine Kinase
“ Under normal conditions, CK levels are 45-260 U/L. After rhabdomyolysis, the levels of CK can be raised to 10.000-200.000 U/L or even 3.000.000.000 U/L. No other condition except rhabdomyolysis can cause such extreme CK elevation.”[3] Creatine Kinase has several forms that include the muscles, heart, brain and kidneys, as well as mitochndria so it is important to look at all values.
Uric Acid
Uric Acid is important to check due to the fact that rhabdomyolysis breaks down skeletal muscle creating more creatinine, which then becomes creatinine which can then lead to acute renal failure, therefore causing the levels of uric acid to rise.
UrinalysisUrine
analysis can be very helpful in diagnosing rhabdomyolysis. Urinalysis will be able to detect changes in the body’s waste, such as increases in uric acid, albumin, as well as myoglobin.[3] Often patients that are positive for rhabdomyolysis have brown tinted urine. Table 3 has a description of common findings in urinalysis.
Causes of Reddish-Brown Discoloration of the Urine[4]
- Myoglobinuria
Rhabdomyolysis
Traumatic
Non-Traumatic
- Hemoglobinuria
Hemolysis
Mechanical Damage
Immunologic Damage
Structural Fragility of Erythrocytes
Microangiopathy
- Hematuria
Renal Causes
Postrenal Causes
- External Factors
Red Beets
Drugs
Vitamin B12
Rifampicin
Phenolphthalein
Phenytoin
Metabolites
Bilirubin
Porphyrin
Systemic Involvement[edit | edit source]
add text here
Medical Management (current best evidence)[edit | edit source]
The best medical management for rhabdomyolysis is stabilizing the patient and aggressive fluid replacement with saline to preserve renal function.[2][3] It is also suggested that fluids be given to victims before extraction. The increase in fluids helps to expand the intravascular volume, thereby inducing diuresis and clearance of toxins.[3] It Is recommended that patients should be given 10 or more liters of fluid per day, so that they maintain a urine output of 150-300 ml/per hour.[3] Sometimes mannitol and bicarbonate are given during the initial resuscitation. It is believed that mannitol acts as a free-radical scavenger minimizing cell injury. Mannitol is also a renal vasodilator to prevent renal failure. Bicarbonate is given to help correct the effects of metabolic acidosis and enhance myoglobin.[3] Along with the patient’s vital signs and urine output, the patient’s electrolytes should be closely monitored.
Prehospital Care[6]
- If Rhabdomyolysis is suspected, establish peripheral access and begin IV rehydration with normal saline
Initial Hospital Stabilization[6]
- Supportive care: ABC measures; treat associated life threatening injuries
- Confirm/establish diagnosis with history, physical examination, laboratory studies (eg. creatine kinase, creatinine, electrolytes, etc.)
- Rehydrate aggressively with normal saline at 10-15 mL/kg/hr to achieve urinary output of 2 mL/kg/hr; switch to hypotonic saline after resuscitation is complete
- Continue rehydration for first 24-72 hours in moderate to severe cases or until patient is hemodynamically stable
- In moderate to severe cases with risk of progression to acute renal failure, preexisting renal disease, or evidence of metabolic acidosis and dehydration, consider urinary alkalinization. The goal urine pH of > 6.5 is achieved by adding 3 ampules of sodium bicarbonate to 1 L of 5% dextrose in water; the solution is infused at an initial rate of 100 mL/hr
- In the nonoliguric patient, consider mannitol 1g/kg IV over 30 min, followed by 5 g/hr IV, for a total of 120 g/day; use mannitol to assist diuresis only in patients who have received adequate volume replacement
- Monitor for and treat hyperkalemia aggressively
- Monitor urinary output and renal function closely
- Monitor for coagulopathy, compartment syndrome, and sepsis in severe cases
- Consider hemodialysis in conjunction with a nephrologist for:
Fulminant renal failure with uremic encephalopathy
Uremic pericardial effusion with tamponade physiology
Refractory hyperkalemia, volume overload, or metabolic acidosis
- Attempt to identify the inciting factor and stop further muscle damage and disease progression
Disposition[6]
- Mild to moderate cases with stable electrolytes that are responding to rehydration, admit to a general medicine ward
- In patients with electrolyte abnormalities or underlying cardiac or renal disease, admit to a monitored bed
- In severe cases, including those with fulminant renal failure with sequelae (pulmonary edema, symptomatic hyperkalemia, oliguria/ anuria), persistent hypotension, or DIC, admit to intensive care unit.
Dialysis
Unfortunately patients that have rhabdomyolysis are more likely to develop acute renal failure. A common treatment for acute renal failure is dialysis to correct fluid, electrolytes, and acid-base abnormalities. This is a slow process to correct the fluid overload and as well as removal of potassium and urea.[2]
Medications[edit | edit source]
Physical Therapy Management (current best evidence)[edit | edit source]
add text here
Alternative/Holistic Management (current best evidence)[edit | edit source]
add text here
Differential Diagnosis[edit | edit source]
Most Common Differential Diagnoses[7]
- Burns, Electrical
- Carnitine Deficiency
- Child Abuse and Neglect, physical abuse
- Dermatomyositis
- Multisystem Organ Failure of Sepsis
- Myoglobinuria[4]
- Neuroleptic Malignant Syndrome
- Sepsis
- Systemic Inflammatory Response Syndrome
- Systemic Lupus Erythmatosus
- Thromboembolism
- Toxic Shock Syndrome
- Toxicity, Ethanol
Other Problems to Consider[7]
Traumatic injuries Viral infections, Myalgias from other etiologies, Bacterial infections, Pyomyositis, Heatstroke , Cold exposure, Snakebite, Malignant hyperthermia, Muscle phosphorylase deficiency, Phosphofructokinase deficiency, Carnitine palmityl transferase deficiency, Phosphoglycerate mutase deficiency, Other inborn errors of metabolism, Hyperosmotic conditions, Guillain-Barré syndrome, Inflammatory myositis.
Case Reports[edit | edit source]
add links to case studies here (case studies should be added on new pages using the case study template)
Resources
[edit | edit source]
add appropriate resources here
Recent Related Research (from Pubmed)[edit | edit source]
see tutorial on Adding PubMed Feed
Extension:RSS -- Error: Not a valid URL: Feed goes here!!|charset=UTF-8|short|max=10
1. : <div class="researchbox"><rss>feed://eutils.ncbi.nlm.nih.gov/entrez/eutils/erss.cgi?rss_guid=1XIG91fZAX3bz2eEvtc9gszJjf_iagixop2cdQYCcbumewWcZo|charset=UTF-8|short|max=10</rss></div> <o:p></o:p>
References[edit | edit source]
see adding references tutorial.
- ↑ 1.0 1.1 Goodman CC, Fuller KS. Pathophysiology: Implications for the Physical Therapist. 3rd ed. St. Louis, MO: Saunders-Elsevier; 2009
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 2.13 2.14 2.15 2.16 2.17 Huerta-Alardin AL, Varon J, Marik P. Bench-to-beside review: Rhabdomyolysis - an overview for clinicians. Critical Care 2005; 9: 158-169
- ↑ 3.00 3.01 3.02 3.03 3.04 3.05 3.06 3.07 3.08 3.09 3.10 3.11 3.12 3.13 3.14 3.15 3.16 3.17 3.18 Efstratiadis G, Voulgaridou A, Nikiforou D, et al. Rhabdomyolysis updated. Hippokratia 2007; 11(3): 129-137.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 Vanholder R, Mehmet S, Erek E, Lameire N. Rhabdomyolysis. Journal of the American Society of Nephrology 2000; 1553-1561.
- ↑ Savage DCL, Forbes M. Idiopathic Rhabdomyolysis. Archieves of Disease in Childhood 1971; 26: 594-607
- ↑ 6.0 6.1 6.2 Walter LA, Catenacci MH. Rhabdomyolysis. Hospital Physician 2008; 25-31.
- ↑ 7.0 7.1 Muscal E. Rhabdomyolysis: Differential Diagnoses and Workup. eMedicine 2009.
Goodman CC, Fuller KS. Pathophysiology: Implications for the Physical Therapist. 3rd ed. St. Louis, MO: Saunders-Elsevier; 2009.
Huerta-Alardin AL, Varon J, Marik P. Bench-to-beside review: Rhabdomyolysis - an overview for clinicians. Critical Care 2005; 9: 158-169.
Efstratiadis G, Voulgaridou A, Nikiforou D, et al. Rhabdomyolysis updated. Hippokratia 2007; 11(3): 129-137.
Goodman CC, Snyder TEK. Differential Diagnosis for Physical Therapists: Screening for Referral. 4th ed. St. Louis, MO: Saunders-Elsevier; 2007
Savage DCL, Forbes M. Idiopathic Rhabdomyolysis. Archives of Disease in Childhood 1971; 26: 594-607.
Muscal E. Rhabdomyolysis: Differential Diagnoses and Workup. eMedicine 2009.
Bagley WH, Yang H, Shah KH. Rhabdomyolysis. Intern Emergency Medicine 2007; 2: 210-218.
Vanholder R, Mehmet S, Erek E, Lameire N. Rhabdomyolysis. Journal of the American Society of Nephrology 2000; 1553-1561.
Walter LA, Catenacci MH. Rhabdomyolysis. Hospital Physician 2008; 25-31.


{kind=link}
{kind=link}