Bankart lesion
Original Editors
Lead Editors - Your name will be added here if you are a lead editor on this page. Read more.
Search Strategy[edit | edit source]
- bankart lesion
- rehabilitation
- operative repair
- shoulder dislocation
Definition/Description[edit | edit source]
A Bankart lesion[1] is a lesion of the anterior part of the glenoid labrum of the shoulder. This injury is caused by repeated anterior shoulder subluxations. The dislocation of the shoulder joint (anterior) can damage the connective tissue ring around the glenoid labrum. It can also bring damage to the connection between the labrum and capsule. Usually it has to do with none or poorly construction of the medial glenohumeral ligament. This injury is common for athletes that practice volleyball, tennis, handball, people who do overhead activities,…
Clinically Relevant Anatomy[edit | edit source]
The Bankart lesion is an injury of the glenohumeral joint. This is a ball-and-socket joint binds the scapular and the humerus. Parts of the joint are the labrum, a fibrocartilaginous structure around the glenoid, the capsule and ligaments and supporting muscle tendons.Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
Epidemiology /Etiology[edit | edit source]
The shoulder is designed for its mobility, with stability being sacrificed to achieve this mobility. Due to poor osseous congruency and capsular laxity, the glenohumeral joint is very unstable, which makes it the most frequently dislocated joint in the human body. It relies on dynamic stabilizers and the neuromuscular system for its stability. Anterior instability is the most common traumatic type of instability, representing approximately 95% of all shoulder instabilities. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title Glenohumeral dislocations are mainly caused by an abduction, extension and external rotation movement. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
In many cases of anterior dislocation patients have a Bankart lesion.
A reverse Bankart lesion can occurs in case of a posterior dislocation.
Characteristics/Clinical [edit | edit source]
We can distinguish to types of Bankart lesions: a soft tissue Bankart lesion and a bony Bankart lesion.
A soft tissue Bankart lesion is an anteroinferior labrum avulsion damage of the glenoid rim. The posterior capsule may be stretched and the inferior glenuhumeral ligament is torn.. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
A bony Bankart lesion shows besides the soft tissue damage also a fracture of the anteroinferior glenoid rim. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
Patients with a Bankart lesion are recognized by shoulder pain which is not localized in a specific point and the pain gets worse when the arm is held behind the back. They also feel weakness and instability of the shoulder. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
The image below shows a spin echo MR arthrographic image. It shows contrast medium interposition between the glenoid rim and the capsulolabral complex, which means that there is a Bankart lesion.
Differential Diagnosis [edit | edit source]
- ALPSA lesion (anterior labral periosteal sleeve avulsion) free and adherent
- Cuff frying
- Rotator Cuff Tears
- SLAP_Lesion(Superior Labrum Anterior Posterior)
- Impingement
If you want to be sure about the diagnosis you will do a MRI. It is the most common imaging tool used to diagnose labral lesions.
Diagnostic Procedures[edit | edit source]
Many patients who sustain a shoulder dislocation will sustain a Bankart lesion. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title Although Bankart lesions often occur in patients with shoulder dislocation, they are hard to detect in physical examination.
For the identification of a Bankart lesion you can use Magnetic Resonance Imaging (MRI). It can be used to quantify the associated medial displacements of the inferior glenohumeral ligament underneath the glenoid. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
According to some studies a Bankart lesion can be diagnosed if contrast medium is interposed between the glenoid and the detached labroligamentous complex. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
The soft tissue Bankart lesion can be seen at arthroscopy and MR arthrography as a fragment of labrum attached to the anterior band of the inferior glenuhumeral ligament and to a rupture in the periosteum of the scapula. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
A bony Bankart lesion can also be discovered by radiographs.
Outcome Measures[edit | edit source]
add links to outcome measures here (also see Outcome Measures Database)
 Examination[edit | edit source]
Examination[edit | edit source]

When you have to examine a patient with internal joint problem you can do a special test: the internal rotation resistance strength test.
The IRRST is a valid stability test, which differentiates an intra-articular pathology from an impingement syndrome. A study was made with 110 patients; the patients were split in 2 groups: people with internal impingement and people with outlet impingement. For this test was reported: a sensibility of 88% and a specificity of 96%[2].
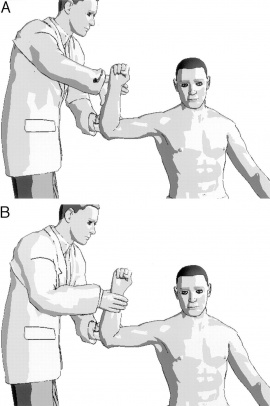
How do you do this test[3]?
You have to stand behind the patient. His injured arm is in a position of 90° abduction and 80° of external rotation. (See picture). You have to ask the patient to resist maximally the first external rotation (A) and then the internal rotation (B). Here you are testing manually the isometric muscle for the external rotation and internal rotation. If the patient has a good strength in external rotation and a weakness while doing the internal rotation, than you can say that the IRRST is positive.
A positive IRRST is based on the fact that at a fixed position of the arm, the medial rotators the caput humerus will do a translocation to the front against the frontal labrum.
A positive result is predictive for an internal impingement, that is frequently a Bankart lesion, and a negative test would suggest a classic outlet impingement[4]
Medical Management
[edit | edit source]
add text here
Physical Therapy Management
[edit | edit source]
There are several options for interventions to the Bankart lesion. First of all we can make the difference between the operative and non-operative interventions.
Possible operative interventions include the arthroscopic Bankart repair and an open Bankart repair. In arthroscopic Bankart repair the muscle strength is regained faster, but the recurrence rates after open Bankart repair are significantly lower.Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title It is proven by several studies that recurrence rate after operative Bankart treatment is significantly reduced compared to a non-operative treatment. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title After surgery there is of course rehabilitation needed which can be slightly comparable to the non-operative rehabilitation program. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
The conservative non-operative Bankart treatment had a significantly worse result with recurrent instability rates ranging from 17% to 96% in patients under age of 30 years. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
Rehabilitation
There are 7 key factors that need to be considered in the rehabilitation of the unstable shoulder. These are:
• Onset of the pathology (traumatic, chronic)
• Degree of instability
• Frequency of dislocation
• Direction of instability (anterior, posterior, multidirectional)
• Concomitant pathologies
• End range neuromuscular control
• Premorbid activity level Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
Besides these key factors physiotherapist should also keep in mind that every patient is different and that we should never forget to personalize a rehabilitation program.
Focus of the rehabilitation program is on maximizing dynamic stability, scapula positioning, proprioception and improving neuromuscular control, as there are no specific exercises to improve the labrum quality. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title Usually the rehabilitation program is divided in 3 phases. The programs for non-operative treatment and postoperative rehabilitation are very similar.
The first phase of rehabilitation consists of sling immobilization with a limited active range of motion for 0 to 4 weeks, this allows 20o of abduction and 40o of internal rotation. [5] This provides an earlier return to functional activity. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title Immobilization in external rotation reduces the risk of recurrent shoulder dislocations. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title After the 14 days passive movement is initiated in a pain free zone. Strengthening exercises are started as isometric contractions to initiate muscle recruitment of the rotator cuff muscles, mostly exercises in a closed kinetic chain, such as pushing your underarm against a wall towards exorotation. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title The goals are to diminish pain and protect healing soft tissues.Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
In the second phase a progressive passive motion is important, together with active-assisted range of motion exercises. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title Strengthening of rotator cuff muscles is initiated in balanced exercises. Examples of exercises are movements of the shoulder executed with elastic bands or dumbbells as dynamic open chain strengthening exercises. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title Rehabilitation should include both closed and open chain exercises. An example of a closed kinetic chain exercise is quadruped position with scapula protraction, progressing to tripod position. A patient can continue to phase three when a normal passive range of motion is achieved.
The third phase focuses on restoration of a full active range of motion. In this phase a progressively increasing resistance in dynamic exercises is stressed to regain full strength for ADL activities. Most imported in this phase is the return to full active activity of normal life. Cite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive titleCite error: Invalid <ref> tag; name cannot be a simple integer. Use a descriptive title
Key Research[edit | edit source]
add links and reviews of high quality evidence here (case studies should be added on new pages using the case study template)
Resources
[edit | edit source]
add appropriate resources here
Clinical Bottom Line[edit | edit source]
add text here
Recent Related Research (from Pubmed)[edit | edit source]
see tutorial on Adding PubMed Feed
Extension:RSS -- Error: Not a valid URL: Feed goes here!!|charset=UTF-8|short|max=10
References[edit | edit source]
see adding references tutorial.
- ↑ Widjaja A, Tran A, Bailey M, Proper S (2006). Correlation between Bankart and Hill-Sachs lesions in anterior shoulder dislocation. ANZ J Surg 76 (6): 436–8.
- ↑ M.H. Moen, R.-J. de vos, E.R.A. van Arkel, A. Weir, J. Moussavi, T. Kraan, D.C. de Winter: De meest waardevolle klinische schoudertesten. Sport en geneeskunde. Oktober 2008, nummer 4. P6-10
- ↑ Zaslav KR. Internal rotation resistance strength test: a new diagnostic test to differentiate intra-articular pathology from outlet (Neer) impingement syndrome in the schoulder. J. Shoulder Elbow Surg 2001 Jan-Feb;10(1):23-7.
- ↑ K. Van Nugteren, D. Winkel, P. van der Tas. Van, Onderzoek en behandeling van de schouder: orthopedisch casuistiek. Maart 2007, hoofdstuk 4, p43-47
- ↑ S-H Kim, K-I Ha, M-W Jung, M-S Lim, Y-M Kim, J-H Park, ‘Accelerated Rehabilitation After Arthroscopic Bankart Repair for Selected Cases: A Prospective Randomized Clinical Study’, Arthroscopy, 2003, Volume 19, Number 7 (Level of Evidence 1B)

