Kinesio Taping
Introduction[edit | edit source]
Kinesiology taping (KT) is a therapeutic tool and has become increasingly popular within the sporting arena. Taping has been used for a long time for the prevention and treatment of sporting injuries. KT is not only used for sporting injuries but fro a variety of other conditions. It was developed by Japanaese Chiropractor Dr. Kenzo Kase in the 1970's with the intention to alleviate pain [1] and improve the healing in soft tissues[2]. There are many proposed benefits to KT including: proprioceptive facilitation, reduced muscle fatigue, muscel facilitation, reduced delayed-onset muscle soreness, pain inhibition, enhanced healing such as reducing oedema and improvement of lymphatic drainage and blood flow[3]
Properties[edit | edit source]
KT is manufactured prestretched by 15-25% as it is applied to the backing paper. It si characterised by the ability to stretch to 120-140% of its original length and, following application, recoil back towards its unstretched length. KT purportedly mimics the physical qualities of the skin as it is believed to be the same weight and thickness of the epidermis along with its inherent elastic properties[4] It is comprised of polymer elastic, wrapped in 100% cotton fibres which allows for evaporation of moisture. The glue is heat activated and is applied in a wave like pattern to mimic the qualities of the fingerprint on the finger tip.
Theory[edit | edit source]
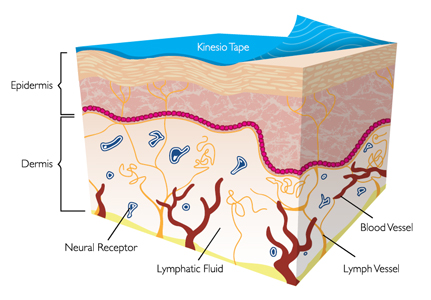
The type of application theoretically determines the physiological outcome. For example, KT is applied unstretched over manually stretched skin above the injured muscle. This typeof application will cause the skin to form convolutions which lifts the skin[5] Theories suggest that these convolutions encourage regeneration of injured tissue by increasing interstitial space and alleviating interstitial pressures which occur from swelling post injury[6]. This decrease in pressure also decompresses suncutaneous nociceptors leading to decreased pain[7]. It is also theorised that lifting the skin dettaches filaments which attach the skin to endothelial cells of the lymphatic and capillary beds. This is proposed to to create channels which allows for lymph to drain ths reducing swelling and allowing increased blood flow to the area[8]. The evidence for these theories is still in its infancy and require extensive research.
 [edit | edit source]
[edit | edit source]

References[edit | edit source]
- ↑ Liu YH, Chen SM, Lin CH, Huang CI, Sun YN. Motion tracking on elbow tissue from ultrasonic image sequence for patients with alteral epicondylitis.Proceedings of the 29th Annual International Conference of the IEEE EMBS Cite Interbationale, Lyon, France, 2007.
- ↑ Kahanov L. Kinesio taping, Part 1: An overview of its use in athletes.Athletic Therapy Today 2007;12:17-18.
- ↑ Basset KT, Lingman SA, Ellis RF. The use and treatment efficacy kinaesthetic taping for musculoskeletal conditions: a systematic review. New Zealand Journal of Physiotherapy 2010;38(2):56-62.
- ↑ Kase K. Clinical therapeutic application of the kinesio taping method. Ken-i Kai Information 2003
- ↑ Cite error: Invalid
<ref>tag; no text was provided for refs namedKahanov L - ↑ Hammer WI. Functional soft tissue examination and treatment by manual methods. 3rd ed. Boston: Jones and Bartlett Publishers, 2006
- ↑ Cite error: Invalid
<ref>tag; no text was provided for refs namedKahanov 2007 - ↑ Lipinska A, Sliwinski Z,Kiebzak W, Senderek T, Kirenko J. Influence of kinesiotaping application on lymphoedema of an upper limb in women after mastectomy. Polish Journal of Physiotherapy 2007:7;258-269.

