Sporting Hand and Wrist - What to Consider When Measuring Range of Motion: Difference between revisions
Carin Hunter (talk | contribs) No edit summary |
Carin Hunter (talk | contribs) No edit summary |
||
| Line 11: | Line 11: | ||
* Proximal region of the hand is the carpus (wrist) | * Proximal region of the hand is the carpus (wrist) | ||
* The middle region the metacarpus (palm) | * The middle region the metacarpus (palm) | ||
* The distal region the phalanges (fingers) | * The distal region the phalanges (fingers) | ||
The forearm unit consists of the radius and ulna, a complex and interrelated set of joints (distal radioulnar joint, proximal radioulnar joint) and the soft tissue stabilizers between the 3 bones. Distally, this is represented by the triangular fibrocartilage complex at the wrist, proximally by the annular ligament at the elbow, and in the forearm by the interosseous membrane. Disruptions in any of these structures may lead to forearm instability, with consequences at each of the remaining structures<ref>Adams JE. Forearm instability: anatomy, biomechanics, and treatment options. The Journal of hand surgery. 2017 Jan 1;42(1):47-52.</ref>. | |||
The triangular fibrocartilage complex is the crucial stabiliser of the latter joint since osseous structures are limited. The palmar and dorsal radioulnar ligaments belong to this complex. The superficial and deep parts of the latter ligaments insert both centrically in accordance to the axis of rotation and eccentrically. This arrangement guarantees stability of the joint throughout pronation and supination<ref>Soubeyrand M, Assabah B, Bégin M, Laemmel E, Dos Santos A, Crézé M. Pronation and supination of the hand: anatomy and biomechanics. Hand Surgery and Rehabilitation. 2017 Feb 1;36(1):2-11.</ref> pronosupination. The interosseous membrane is a further relevant stabiliser that guarantees sufficient load transmission from radius to ulna. The distal oblique bundle of the interosseous membrane is outstanding in this context. The pronator quadratus muscle is the relevant dynamic stabiliser of the distal radioulnar joint. Contraction of the muscle prevents diastasis of the joint. The deep head of the muscle is always activated during pronosupination.<ref>Spies CK, Langer M, Müller LP, Oppermann J, Löw S, Unglaub F. Anatomy and biomechanics of the distal radioulnar joint. Der Orthopade. 2018 Aug 1;47(8):621-7.</ref>[[File:Bigstock-Skeletal-System-Phalanges-89698643.jpg|center|Skeletal System Phalanges - 89698643|1000x1000px]] | |||
== Joints in the wrist and hand == | == Joints in the wrist and hand == | ||
{| class="wikitable" | {| class="wikitable" | ||
| Line 300: | Line 302: | ||
== Considerations when measuring wrist flexion and extension == | == Considerations when measuring wrist flexion and extension == | ||
# Coupling | # Coupling | ||
Coupling occurs in the wrist while performing flexion–extension and radial–ulnar deviation movements. Maximal wrist range of motion is near the neutral position. The wrist should be placed at a neutral position in work station design to account for the naturally coupled wrist motion<ref>Li ZM, Kuxhaus L, Fisk JA, Christophel TH. Coupling between wrist flexion–extension and radial–ulnar deviation. Clinical biomechanics. 2005 Feb 1;20(2):177-83.</ref>.<gallery widths="“250px”" heights="“350px”"> | Coupling occurs in the wrist while performing flexion–extension and radial–ulnar deviation<ref>Akhbari B, Moore DC, Laidlaw DH, Weiss AP, Akelman E, Wolfe SW, Crisco JJ. Predicting carpal bone kinematics using an expanded digital database of wrist carpal bone anatomy and kinematics. Journal of Orthopaedic Research®. 2019 Dec;37(12):2661-70.</ref> movements. Maximal wrist range of motion is near the neutral position. The wrist should be placed at a neutral position in work station design to account for the naturally coupled wrist motion<ref>Li ZM, Kuxhaus L, Fisk JA, Christophel TH. Coupling between wrist flexion–extension and radial–ulnar deviation. Clinical biomechanics. 2005 Feb 1;20(2):177-83.</ref>.<gallery widths="“250px”" heights="“350px”"> | ||
File:E RD.png|Extension/radial deviation | File:E RD.png|Extension/radial deviation | ||
File:Neutral.png|Neutral | File:Neutral.png|Neutral | ||
Revision as of 09:52, 24 March 2021
Bony Anatomy[edit | edit source]
The hand and wrist have a total of 27 bones arranged to roll, spin and slide[1]; allowing the hand to explore and control the environment and objects.
The carpus is formed from eight small bones collectively referred to as the carpal bones. The carpal bones are bound in two groups of four bones:
- the pisiform, triquetrum, lunate and scaphoid on the upper end of the wrist
- the hamate, capitate, trapezoid and trapezium on the lower side of the hand.
Other bones of the hand are:
- the metacarpals – the five bones that comprise the middle part of the hand
- the phalanges (singular phalanx) – the 14 narrow bones that make up the fingers of each hand. Each finger has three phalanges (the distal, middle, and proximal); the thumb has two[2].
The hand is divided into three regions[3]
- Proximal region of the hand is the carpus (wrist)
- The middle region the metacarpus (palm)
- The distal region the phalanges (fingers)
The forearm unit consists of the radius and ulna, a complex and interrelated set of joints (distal radioulnar joint, proximal radioulnar joint) and the soft tissue stabilizers between the 3 bones. Distally, this is represented by the triangular fibrocartilage complex at the wrist, proximally by the annular ligament at the elbow, and in the forearm by the interosseous membrane. Disruptions in any of these structures may lead to forearm instability, with consequences at each of the remaining structures[4].
The triangular fibrocartilage complex is the crucial stabiliser of the latter joint since osseous structures are limited. The palmar and dorsal radioulnar ligaments belong to this complex. The superficial and deep parts of the latter ligaments insert both centrically in accordance to the axis of rotation and eccentrically. This arrangement guarantees stability of the joint throughout pronation and supination[5] pronosupination. The interosseous membrane is a further relevant stabiliser that guarantees sufficient load transmission from radius to ulna. The distal oblique bundle of the interosseous membrane is outstanding in this context. The pronator quadratus muscle is the relevant dynamic stabiliser of the distal radioulnar joint. Contraction of the muscle prevents diastasis of the joint. The deep head of the muscle is always activated during pronosupination.[6]

Joints in the wrist and hand[edit | edit source]
| Joint | Proximal articulation | Distal Articulation | Type | Movement |
|---|---|---|---|---|
| Radiocarpal joint | Radius and articular disc/ concave | Scaphoid, lunate, triquetrum / – convex | Ellipsoid | Flexion-extension; Abduction-adduction |
| Midcarpal joint | Scaphoid. Lunate, Triquetrum | Trapezium, Trapezoid, Capitate, Hamate | Gliding | Flexion-extension; Abduction-adduction |
| Carpometacarpal joint (thumb) | 1st metacarpal | trapezium | Saddle | Flexion-extension; Abduction-adduction; circumduction; opposition |
| Carpometacarpal joint (fingers) | 2nd metacarpal
3rd metacarpal 4th metacarpal 5th metacarpal |
trapezoid, trapezium
capitate capitate, hamate hamate |
Ellipsoidal | Flexion-extension |
| Metacarpophalangeal joints | Metacarpals | phalangeal | Ellipsoidal | Flexion, extension, abduction, adduction, circumduction |
| Interphalangeal | Distal phlangeal | Proximal phalangeal | Hinge | Flexion (lots) Extension (minimal) |
Table summarises from - Kapandji I.A. The Physiology of the Joints: Volume 1, The Upper Limb. 5th Ed. London: Churchill Livingstone, 1982
Range of motion in the wrist and hand[edit | edit source]
| Movement | Muscles | Range | Origin | Insertion | Innervation | Joint |
| Flexion | Flexor carpi radialis | 0-80 | Medial Epicondyle of humerus | 2nd and 3rd metacarpals | Median nerve (C6,7) | 60% midcarpal joint
40% radiocarpal joint |
| Flexor carpi ulnaris | Medial epicondyle of humerus and sup.post. border of ulna | Pisiform, hamate and base 5th metacarpal | Ulnar nerve (C7,8) | |||
| Palmaris longus | Medial epicondyle of humerus | Flexor reinaculum and palmar aponeurosis | Median nerve (C8) | |||
| Flexor digitorum superficialis | Medial epicondyle of humerus, coronoid process of
ulna, and a ridge along lateral margin of anterior surface of radius |
Middle phalanges of each finger | Median nerve (C7,8 T1) | |||
| Flexor digitorum profundus | Anterior medial surface of body of ulna | Base of distal phalanx of thumb | Median nerve (C7,8, T1)
Ulnar nerve (C8, T1) |
|||
| Flexor pollicis longus | Anterior surface of radius and interosseous membrane | Base of distal phalanx of thumb | Median nerve (C8, T1) | |||
| Extension | Extensor carpi radialis longus | 0-70 | Lateral supracondylar ridge of humerus | 2nd metacarpal | Radial nerve (C6,7) | 40% midcarpal joint
60% radiocarpal joint |
| Extensor carpi radialis brevis | Lateral epicondyle of humerus | Distal and middle phalanges of each finger | Radial nerve (C6,7) | |||
| Extensor carpi ulnaris | Lateral epicondyle of humerus and posterior border of ulna | 5th metacarpal | Radial nerve (C7,8) | |||
| Extensor digitorum | Lateral epicondyle of humerus | Distal and middle phalanges of each finger | Radial nerve (C7,8) | |||
| Extensor indicis | Posterior surface of ulna | Tendon of extensor digitorum of index finger | Radial nerve (C7, 8) | |||
| Extensor digiti minimi | Lateral epicondyle of humerus | Tendon of extensor digitorum on 5th phalanx | Radial nerve (C7,8) | |||
| Extensor pollicis longus | Posterior surface of middle of radius and ulna and interosseous membrane | 1st metacarpal | Radial nerve (C7,8) | |||
| Extensor pollicis brevis | Posterior surface of middle of radius | Base of proximal phalanx of thumb | Radial nerve (C7,8) | |||
| Radial deviation | Flexor carpi radialias | 30 | Medial Epicondyle of humerus | 2nd and 3rd metacarpals | Median nerve (C6,7) | Radiocarpal Jt |
| Ulnar deviation | Flexor carpi ulnaris | 20 | Medial epicondyle of humerus and sup.post. border of ulna | Pisiform, hamate and base 5th metacarpal | Ulnar nerve (C7,8) | Radiocarpal Jt |
| Supination
(of forearm) |
Supinator | 60 | Lateral epicondyle of humerus and ridge near radial notch of ulna | Lateral surface of proximal one-third of radius | Radial nerve (C5,6) | Sup. and inf.radioulnar jt |
| Biceps brachii | Long head - supraglenoid tubercle; Short head - coracoid process of scapula | Radial tuberosity and bicipital aponeurosis | Musculocutaneous nerve (C5,6) | |||
| Brachioradialis | Medial and lateral borders of distal end of humerus | Superior to styloid process of radius | Radial Nerve (C5,6) | |||
| Pronation
(of forearm) |
Pronator teres | 40 | Medial epicondyle of humerus and coronoid process of ulna | Midlateral surface of radius | Median nerve (C6,7) | Sup.and inf.radioulnar jt |
| Pronator quadratus | Distal portion of shaft of ulna | Distal portion of shaft of radius | Median nerve (C8, T1) | |||
| Brachioradialis | Medial and lateral borders of distal end of humerus | Superior to styloid process of radius | Radial nerve (C5,6) | |||
| Distal Interphalangeal | ||||||
| Proximal Interphalangeal |
Table summarised from Anatomy and Human Movement: Structure and Function. 6th Ed.[7]
Tools used to measure range of motion in the wrist and hand[edit | edit source]

Goniometer position for wrist flexion and extension

Inclinometer

Cellphone Inclinometer



| Goniometer | Inclinometer | Cellphone Inclinometer | |
|---|---|---|---|
| Pros | Compact, easy to use and portable | Accurate and measures multiple planes | Accurate, measures multiple planes, free downloadable appconvenient |
| Limitations | Only one plane of movement | Bulky and expensive |
Considerations when measuring wrist flexion and extension[edit | edit source]
- Coupling
Coupling occurs in the wrist while performing flexion–extension and radial–ulnar deviation[8] movements. Maximal wrist range of motion is near the neutral position. The wrist should be placed at a neutral position in work station design to account for the naturally coupled wrist motion[9].
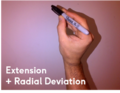
Extension/radial deviation

Neutral
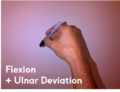
Flexion/Ulnar deviation



2. Open versus closed hand

Flexion
- Open hand = joint
- Closed hand = soft tissue
Extension
- Open hand = soft tissue
- Closed hand = joint
Reason to measure[edit | edit source]
The main reason to measure is that you have an accurate baseline to base your rehab and progression off.
- ↑ Maitland, G.D. Maitland's Peripheral Manipulations. 3rd Edition Edinburg: Elsevier Butterworth-Heinemann, 1999
- ↑ Chim H. Hand and Wrist Anatomy and Biomechanics: A Comprehensive Guide. Plastic and reconstructive surgery. 2017 Oct 1;140(4):865.
- ↑ Physical Examination of the Spine and Extremities. Hoppenfield, S. New York: Appleton-Century-Crofts, 1976.
- ↑ Adams JE. Forearm instability: anatomy, biomechanics, and treatment options. The Journal of hand surgery. 2017 Jan 1;42(1):47-52.
- ↑ Soubeyrand M, Assabah B, Bégin M, Laemmel E, Dos Santos A, Crézé M. Pronation and supination of the hand: anatomy and biomechanics. Hand Surgery and Rehabilitation. 2017 Feb 1;36(1):2-11.
- ↑ Spies CK, Langer M, Müller LP, Oppermann J, Löw S, Unglaub F. Anatomy and biomechanics of the distal radioulnar joint. Der Orthopade. 2018 Aug 1;47(8):621-7.
- ↑ Palastanga N, Soames R. Anatomy and Human Movement: Structure and Function. 6th Ed. London: Churchill Livingstone, 2012
- ↑ Akhbari B, Moore DC, Laidlaw DH, Weiss AP, Akelman E, Wolfe SW, Crisco JJ. Predicting carpal bone kinematics using an expanded digital database of wrist carpal bone anatomy and kinematics. Journal of Orthopaedic Research®. 2019 Dec;37(12):2661-70.
- ↑ Li ZM, Kuxhaus L, Fisk JA, Christophel TH. Coupling between wrist flexion–extension and radial–ulnar deviation. Clinical biomechanics. 2005 Feb 1;20(2):177-83.

