Factors Affecting Wound Healing: Difference between revisions
No edit summary |
No edit summary |
||
| Line 13: | Line 13: | ||
<blockquote>'''Intrinsic factors''' are those related to the person that cannot be changed, but may be managed.<ref name=":0" /> </blockquote> | <blockquote>'''Intrinsic factors''' are those related to the person that cannot be changed, but may be managed.<ref name=":0" /> </blockquote> | ||
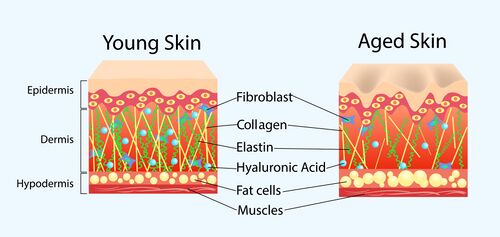
# '''Age'''. The epidermis becomes thinner with age and has a slower turnover. Collagen, elastin, and hyaluronic acid production also decreases as skin ages and this makes older skin more susceptible to tears and wounding. Human growth hormone plays a significant role in tissue healing and this decreases with age as well. Once older skin is wounded, it heals slower due to slower turnover of keratinocytes, reduced blood flow to the dermis, and a slowing of the complex healing cascade.<ref name=":0" /> | # [[File:Young vs aged skin.jpeg|right|frameless|500x500px]]'''Age'''. The epidermis becomes thinner with age and has a slower turnover. Collagen, elastin, and hyaluronic acid production also decreases as skin ages and this makes older skin more susceptible to tears and wounding. Human growth hormone plays a significant role in tissue healing and this decreases with age as well. Once older skin is wounded, it heals slower due to slower turnover of keratinocytes, reduced blood flow to the dermis, and a slowing of the complex healing cascade.<ref name=":0" /> | ||
# '''Genetics.''' | # '''Genetics.''' | ||
# | #* Tipton et al 2020 looked at the microbiomes of chronic wounds and found that people tend to be susceptible to infections by certain pathogens depending on their genotype. The researchers also found that the variety of bacteria present is significantly related to wound healing. The more varied a wound microbiome, the faster that wound will close. While a person's microbiome is somewhat modifiable, much of the baseline is related to genotype and to the microbiome you are born and seeded from during the birthing process.<ref name=":0" /> <ref>Tipton CD, Wolcott RD, Sanford NE, Miller C, Pathak G, Silzer TK, Sun J, Fleming D, Rumbaugh KP, Little TD, Phillips N. [https://journals.plos.org/plospathogens/article?id=10.1371/journal.ppat.1008511 Patient genetics is linked to chronic wound microbiome composition and healing]. PLoS pathogens. 2020 Jun 18;16(6):e1008511.</ref> | ||
#* Skin elasticity and ability to lay down collagen and fibrin is also genetically linked. This process can be seen in the body's ability to form scars, stretch marks, and wrinkles. Research in mice has found wound healing to be genetically controlled with a heritability rate of up to 86%. Other research in humans has found specific gene expression to be associated with the onset and progression of wound healing. <ref name=":0" /><ref>Zhu HJ, Fan M, Gao W. [https://link.springer.com/article/10.1186/s12893-021-01298-w Identification of potential hub genes associated with skin wound healing based on time course bioinformatic analyses]. BMC surgery. 2021 Dec;21(1):1-3.</ref> | |||
# [[File:Sex hormone production.jpeg|thumb|400x400px|This graphic is specifically looking at genetically determined sex hormone averages and does not take into account those with altered sexual expression or hormonal levels outside of the average range. ]]'''Sex hormones'''. This is a complex topic. The research is mixed with some showing oestrogens to speed healing and others in favour of androgens, depending on what phase the wound is in.<ref>Engeland CG, Sabzehei B, Marucha PT. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2746088/ Sex hormones and mucosal wound healing]. Brain, behavior, and immunity. 2009 Jul 1;23(5):629-35.</ref> For most patients, this will not be of concern. However, this may need to be taken into consideration for patients taking synthetic hormones or going through an abrupt hormonal change, such as menopause.<ref name=":0" /> | |||
# '''Systemic diseases'''. Common medical conditions that may affect healing are (1) diabetes, (2) vascular diseases, (3) pulmonary diseases, (4) immunocompromised or autoimmune conditions, and (5) conditions that affect the autonomic nervous system. Both sympathetic and parasympathetic divisions play important roles in the wound healing phases.<ref name=":0" /> | # '''Systemic diseases'''. Common medical conditions that may affect healing are (1) diabetes, (2) vascular diseases, (3) pulmonary diseases, (4) immunocompromised or autoimmune conditions, and (5) conditions that affect the autonomic nervous system. Both sympathetic and parasympathetic divisions play important roles in the wound healing phases.<ref name=":0" /> | ||
#*'''Diabetes.''' Hyperglycaemia delays healing, therefore blood glucose levels need to be kept as close to ideal range as possible. Ideally, blood glucose levels should be kept as close to normal range as possible. However, even a reduction of blood glucose to 11.1 millimoles per litre, (200 milligrammes per decilitre) will still have a beneficial affect on wound healing. Likewise, patients with an A1C of less than 7.1% have improved healing time. Providing this education to patients can help them to feel motivated in their progress toward more control blood glucose levels.<ref name=":0" /> | #*'''Diabetes.''' Hyperglycaemia delays healing, therefore blood glucose levels need to be kept as close to ideal range as possible. Ideally, blood glucose levels should be kept as close to normal range as possible. However, even a reduction of blood glucose to 11.1 millimoles per litre, (200 milligrammes per decilitre) will still have a beneficial affect on wound healing. Likewise, patients with an A1C of less than 7.1% have improved healing time. Providing this education to patients can help them to feel motivated in their progress toward more control blood glucose levels.<ref name=":0" /> | ||
| Line 36: | Line 38: | ||
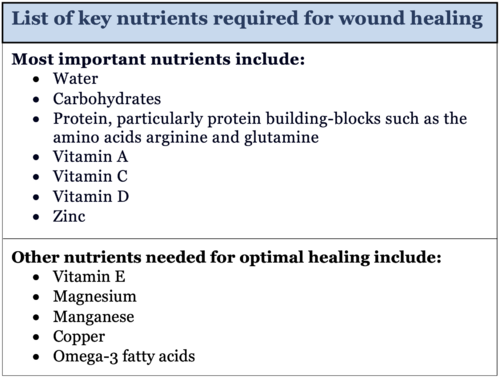
# [[File:Nutrition for wound healing.png|right|frameless|500x500px]]'''Nutrition.''' The nutritional requirements for tissue healing are greater than the levels recommended for routine tissue maintenance or the recommended daily allowance (RDA).<ref>Polcz ME, Barbul A. The role of vitamin A in wound healing. Nutrition in Clinical Practice. 2019 Oct;34(5):695-700.</ref> <ref>T. H. Chan School of Public Health, Harvard University. The nutrition source: Vitamin D. Published May, 2020. Accessed October 25, 2021. </ref><ref>McDaniel JC, Belury M, Ahijevych K, et al. Omega-3 fatty acids effect on wound healing. Wound Repair Regen. 2008;16(3):337–45.</ref> To use water as an example with wound healing, additional water is needed to help with tissue repair depending on size of wound and patient's overall health. It is estimated that a person's water requirements during wound healing are increased by approximately 20 to 30% above their normal requirements. These adjustments will be made by a dietitians or physician while the patient is healing. Typically they will be prescribed supplements at a dose that is above a nutrient's RDAs for two to 12 weeks while wound healing is initiated and then reduces back to the RDA levels or weaned off completely once healing is complete and a regular diet is established.<ref name=":0" /> | # [[File:Nutrition for wound healing.png|right|frameless|500x500px]]'''Nutrition.''' The nutritional requirements for tissue healing are greater than the levels recommended for routine tissue maintenance or the recommended daily allowance (RDA).<ref>Polcz ME, Barbul A. The role of vitamin A in wound healing. Nutrition in Clinical Practice. 2019 Oct;34(5):695-700.</ref> <ref>T. H. Chan School of Public Health, Harvard University. The nutrition source: Vitamin D. Published May, 2020. Accessed October 25, 2021. </ref><ref>McDaniel JC, Belury M, Ahijevych K, et al. Omega-3 fatty acids effect on wound healing. Wound Repair Regen. 2008;16(3):337–45.</ref> To use water as an example with wound healing, additional water is needed to help with tissue repair depending on size of wound and patient's overall health. It is estimated that a person's water requirements during wound healing are increased by approximately 20 to 30% above their normal requirements. These adjustments will be made by a dietitians or physician while the patient is healing. Typically they will be prescribed supplements at a dose that is above a nutrient's RDAs for two to 12 weeks while wound healing is initiated and then reduces back to the RDA levels or weaned off completely once healing is complete and a regular diet is established.<ref name=":0" /> | ||
# '''Stress and elevated cortisol levels.''' Stress results in (1) an increase in incidence of opportunistic infection, (2) reduced expression of human growth hormone, and (3) delayed healing.<ref name=":0" /> | # '''Stress and elevated cortisol levels.''' Stress results in (1) an increase in incidence of opportunistic infection, (2) reduced expression of human growth hormone, and (3) delayed healing.<ref name=":0" /> | ||
#* | #*Gouin et al 2011 compared the healing rate of a small punch biopsy wound on a group of dental students. They found that the participants healed an average of three days slower when they were under the stress of exams as compared to when they were on vacation break. This represented a 40% longer healing time for a small standardised wound in a young and otherwise healthy population.<ref>Gouin JP, Kiecolt-Glaser JK. [https://www.immunology.theclinics.com/article/S0889-8561(10)00081-0/fulltext The impact of psychological stress on wound healing: methods and mechanisms]. Immunology and Allergy Clinics. 2011 Feb 1;31(1):81-93.</ref> | ||
#* Older persons with multiple comorbidities are already at risk for delayed healing, stress further compounds that risk.<ref name=":0" /> | #* Older persons with multiple comorbidities are already at risk for delayed healing, stress further compounds that risk.<ref name=":0" /> | ||
#* People who are stressed are more likely to engage in other habits that can delay wound healing, such as the (1) use of alcohol, tobacco or drugs, (2) less physical activity, (3) less sleep, (4) poor nutrition, and a (5) lack of medication compliance.<ref name=":0" /> | #* People who are stressed are more likely to engage in other habits that can delay wound healing, such as the (1) use of alcohol, tobacco or drugs, (2) less physical activity, (3) less sleep, (4) poor nutrition, and a (5) lack of medication compliance.<ref name=":0" /> | ||
Revision as of 21:52, 3 October 2022
Top Contributors - Stacy Schiurring and Jess Bell
Introduction[edit | edit source]
Disclaimer: This page discusses the use of sharp debridement of the wound bed. This is an advanced treatment technique which requires specialised training to properly and safely perform. Please be aware of your profession's practice act. Traditionally sharp excisional debridement into healthy viable tissue can only be performed by a medical doctor with advanced training, while other health professionals in some areas can perform sharp debridement of nonviable tissue only with advanced training.
There are many factors to take into consideration when practicing wound care. Some of these factors are within the control of the rehabilitation professional, and some are not. By gaining an understanding of these key factors, the rehabilitation professional will be able to adjust the wound care treatment plan to obtain the best possible healing outcome. There are three types of factors which can affect wound healing: (1) intrinsic, (2) extrinsic, and (3) iatrogenic.[1]
Understanding the influence of these factors can help shape and inform a wound care assessment, treatment plan, and prognosis. For example, it is unrealistic to expect a wound to heal in the same manner a young healthy person as in an older person with multiple comorbidities. Providing patients with realistic expectations of the healing process improves goal setting and builds trust between patient can care provider.[1]
Intrinsic Factors[edit | edit source]
Intrinsic factors are those related to the person that cannot be changed, but may be managed.[1]
- Age. The epidermis becomes thinner with age and has a slower turnover. Collagen, elastin, and hyaluronic acid production also decreases as skin ages and this makes older skin more susceptible to tears and wounding. Human growth hormone plays a significant role in tissue healing and this decreases with age as well. Once older skin is wounded, it heals slower due to slower turnover of keratinocytes, reduced blood flow to the dermis, and a slowing of the complex healing cascade.[1]
- Genetics.
- Tipton et al 2020 looked at the microbiomes of chronic wounds and found that people tend to be susceptible to infections by certain pathogens depending on their genotype. The researchers also found that the variety of bacteria present is significantly related to wound healing. The more varied a wound microbiome, the faster that wound will close. While a person's microbiome is somewhat modifiable, much of the baseline is related to genotype and to the microbiome you are born and seeded from during the birthing process.[1] [2]
- Skin elasticity and ability to lay down collagen and fibrin is also genetically linked. This process can be seen in the body's ability to form scars, stretch marks, and wrinkles. Research in mice has found wound healing to be genetically controlled with a heritability rate of up to 86%. Other research in humans has found specific gene expression to be associated with the onset and progression of wound healing. [1][3]
- Sex hormones. This is a complex topic. The research is mixed with some showing oestrogens to speed healing and others in favour of androgens, depending on what phase the wound is in.[4] For most patients, this will not be of concern. However, this may need to be taken into consideration for patients taking synthetic hormones or going through an abrupt hormonal change, such as menopause.[1]
- Systemic diseases. Common medical conditions that may affect healing are (1) diabetes, (2) vascular diseases, (3) pulmonary diseases, (4) immunocompromised or autoimmune conditions, and (5) conditions that affect the autonomic nervous system. Both sympathetic and parasympathetic divisions play important roles in the wound healing phases.[1]
- Diabetes. Hyperglycaemia delays healing, therefore blood glucose levels need to be kept as close to ideal range as possible. Ideally, blood glucose levels should be kept as close to normal range as possible. However, even a reduction of blood glucose to 11.1 millimoles per litre, (200 milligrammes per decilitre) will still have a beneficial affect on wound healing. Likewise, patients with an A1C of less than 7.1% have improved healing time. Providing this education to patients can help them to feel motivated in their progress toward more control blood glucose levels.[1]
- Venous insufficiency. A wound will not heal when persistent oedma is present. Oedema results in fibrinogen leaking out of capillaries into the dermis, which blocks oxygen and nutrients from being delivered to the tissues. This reduces blood flow and results in tissue hypoxia. Tissue hypoxia impairs tissue repair and increases susceptibility to infection by anaerobic microbes. It also inhibits fibroblast function and suppresses epithelial cells.[1]
- Arterial insufficiency. Blood flow to tissue needs to be optimised to facilitate wound closure. Insufficient perfusion reduces delivery of the oxygen cells and nutrients necessary for healing.[1]
- Idiopathic pulmonary fibrosis. Pulmonary fibrosis reduces tissue oxygenation and negatively affects the tissue repair mechanisms via widespread epithelial injury.[1]
- Other chronic pulmonary diseases that affect tissue oxygenation can also impact healing.[1]
- Immunocompromised conditions. Such conditions prevent the necessary inflammatory response to initiate the healing cascade. This leads to an increased risk of infection, decreased phagocytosis, and decreased fibroblast activity.[1]
- Sensory and autonomic neuropathy. The neurotransmitters and neuropeptides produced by the cutaneous nerves are essential for all phases of repair. These substances are responsible for plasma extravasation, vasodilation, and neurogenic inflammation. Neuropathy limit the production of these substances.[1]


Extrinsic Factors[edit | edit source]
Extrinsic factors are things external to the wound that we can directly control.[1]
- Medications. It is important to perform a medication review and investigate any potential effects which could delay healing. Listed below is a non-exhaustive list of common medications which interfere with wound healing.[1]
- Steroids will delay all phases of wound healing. However they can also contribute to elevated glucose levels with long-term use, recall how hyperglycaemia can delay healing as discussed above.[1]
- Anticoagulants inhibit the coagulation cascade and can result in tissue necrosis, this is especially common in fatty tissue.[1]
- Long-term NSAID use delays wound healing by (1) suppressing the inflammatory response, (2) decreasing collagen synthesis, (3) reducing tensile strength and (4) increasing risk of infection.[1]
- Chemotherapy drugs interfere with (1) cell proliferation, (2) prolong inflammation, (3) inhibit protein synthesis, and (4) decrease collagen synthesis. Chemotherapy-associated nausea and vomiting may also impair nutrition (see below for more details on nutrition).[1]
- Immunosuppressive or anti-rejection medications (1) impair fibroblast formation, (2) increase risk of infection and (3) decrease wound tensile strength. The gastrointestinal side effects of these medications can also impair nutrition (see below for more details on nutrition).[1]
- Nutrition. The nutritional requirements for tissue healing are greater than the levels recommended for routine tissue maintenance or the recommended daily allowance (RDA).[5] [6][7] To use water as an example with wound healing, additional water is needed to help with tissue repair depending on size of wound and patient's overall health. It is estimated that a person's water requirements during wound healing are increased by approximately 20 to 30% above their normal requirements. These adjustments will be made by a dietitians or physician while the patient is healing. Typically they will be prescribed supplements at a dose that is above a nutrient's RDAs for two to 12 weeks while wound healing is initiated and then reduces back to the RDA levels or weaned off completely once healing is complete and a regular diet is established.[1]
- Stress and elevated cortisol levels. Stress results in (1) an increase in incidence of opportunistic infection, (2) reduced expression of human growth hormone, and (3) delayed healing.[1]
- Gouin et al 2011 compared the healing rate of a small punch biopsy wound on a group of dental students. They found that the participants healed an average of three days slower when they were under the stress of exams as compared to when they were on vacation break. This represented a 40% longer healing time for a small standardised wound in a young and otherwise healthy population.[8]
- Older persons with multiple comorbidities are already at risk for delayed healing, stress further compounds that risk.[1]
- People who are stressed are more likely to engage in other habits that can delay wound healing, such as the (1) use of alcohol, tobacco or drugs, (2) less physical activity, (3) less sleep, (4) poor nutrition, and a (5) lack of medication compliance.[1]
- Sleep deprivation. Lack of quality sleep can lead to (1) increased cortisol production, (2) elevated rates of illness and infection, (3) delayed skin barrier recovery, (4) reduced growth hormone production, and (5)impaired healing potential. It is important to recall that sleep disturbances can be a common side effect of many medications and underlying health conditions,[9] therefore a thorough patient interview and medication review is indicated. Ideally adults should get 8-9 hours of sleep per night.[1]
- Smoking. Smoking leads to (1) hypoxia, (2) tissue ischaemia, (3) blood vessel inflammation, and (4) interferes with every phase of wound healing. Please see special topic box below for more details on this topic.[1]
- Alcohol. Drinking alcohol (1) delays wound closure, (2) increases the risk of infection, (3) reduces angiogenesis, (4) impairs collagen production, (5) interferes with epithelialisation, and (6) induces tissue hypoxia. Wound healing can be listed after just a few exposures to alcohol drinking above the legal limit.[1]
- Infection.
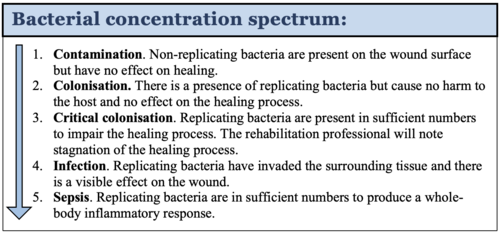
- Bacterial infection. All skin surfaces, including open wounds, are colonised with bacteria. Some bacteria are harmless and are part of the skin's biome. They are necessary for wound healing. Chronic wounds will have more bacterial colonisation than acute wounds and tend to have more pathogenic bacteria. This does not create a problem as long as the body can manage the level of bacterial colonization. The amount of bacteria present in the wound is categorised on a spectrum. Local infection delays wound healing by (1) reducing collagen production, (2) decreasing nutrients available for healing and (3) killing cells vital for the healing process.[1]
- Fungal infection. These infections are particularly problematic for patients who are immunocompromised. They can occur more often with compression therapy dressings, which stay in place for up to seven days. Wound drainage and sweat create a moist environment within compression dressing that are ideal for fungal growth. This is especially true in hot and humid environments. Fungal infections are best managed through (1) topical anti-fungals, (2) more frequent dressing changes and (3) adequate absorption via dressing selection to manage wound drainage.[1]
- Biofilm. This is a topic of new and emerging research, and is not yet fully understood. Bacteria have evolved a variety of strategies that help to ensure their survival. So one of these is the development of a polysaccharide capsule that they sort of make around themselves and it shields them from destruction by the host's immune defences.
- Biofilm adheres to the wound bed and is difficult to remove, making the wound resistant to healing.
- Biofilm can be invisible to the naked eye (will make the wound surface appear shiny or slimy) or it can also resemble a thin layer of slough (yellow in colour) on the wound's surface.
- Mature biofilm can form in a matter of a few days
- 90% of chronic wounds will have biofilms
- Biofilm must be removed in order for wound healing. Regularly repeated sharp debridement is the preferred method to remove biofilm. Antimicrobial dressings are not an acceptable treatment method because they can not penetrate the biofilm in order to kill the invading bacteria.[1]
- Obesity. Obesity is a known risk factor for multiple diseases. It also increases the risk of (1) wound infections, (2) haematomas, (3) surgical complications, (4) venous ulcers, and (5) pressure injuries.[1]
- These risks are likely due to the (1) decreased tissue perfusion and ischaemia in adipose tissue, (2) increased tissue tension on wound edges, and (3) inadequate delivery of antibiotics.
- Adipocytes have been shown to secrete factors that interfere with the normal inflammatory and immune responses.
- Other concerns which have the potential to affect wound healing in patients with obesity include increased risk of (1) pressure, (2) friction, (3) maceration, (4) limited mobility and or a sedentary lifestyle, and (5) oedema.[1]


Special Topic: Smoking and wound healing
Smoking causes (1) hypoxia, (2) tissue ischaemia, (3) blood vessel inflammation, and (4) interferes with every phase of wound healing.
Smoking just one cigarette has been shown to reduce tissue oxygen concentrations. People that are pack-per-day smokers experience tissue hypoxia during a significant portion of each day. Even 20 minutes without smoking has been shown to improve blood flow to the hands and feet. After 12 hours without smoking, the oxygen level in the blood begins to return to near normal levels. And after 24 hours without smoking, the nerves begin to recover. Smoking cessation has been shown to restore the tissue microenvironment and cellular functions within four weeks. For heavy smokers that are unable to quit, even cutting down to less than one pack per day may show improvement in tissue healing ability compared to more than one pack per day. So gradual reduction of smoking should continue as able beyond that point. Strategies such as smoking only three-quarter, one-half, or one-quarter of each cigarette can further reduce the detrimental effects that are caused by smoking. Smokers have also been shown to have significantly lower levels of plasma vitamin C compared to non-smokers. For these people, diets that are higher in vitamin C or including vitamin C supplementation may be considered to mitigate blood vessel damage and then further promote healing.
Iatrogenic Factors[edit | edit source]
Iatrogenic factors are related to how the wound is managed. The rehabilitation professional can have the biggest influence over this factor by modifying the treatment plan throughout the healing process after assessing the wound's response to interventions.[1]
- Dressing selection and management.[1]
- Compression is essential for venous wounds, and is indicated for oedema reduction in other wounds as well. Care must be taken to apply compression appropriately and monitor patient response regularly. Compression applied over an arterial wound or with incorrect technique can reduce tissue perfusion and or create a tourniquet effect that damages both the wound and the peri-wound tissue.
- Dressing removal with poor technique can result in trauma to the healing wound tissues.
- Inappropriate dressing choice for a wound can cause tearing or maceration. Wounds require a moist environment for proper healing, proper dressing selection is finding a balance between keeping to wound bed too moist or too dry. Proper dressing selection requires consideration of drainage type and amount and the planned frequency of dressing changes. Repeated assessments must be performed to monitor the wound's response to the selected dressings.
- Too many dressing changes can also delay healing. When the wound bed is exposed to the outside environment during a dressing change, it can take up to 40 minutes for wound tissue to return to proper temperatures optional for healing. In addition, cellular mitosis is disrupted for up to three hours after a dressing change.
- Incorrect, unnecessary, or too frequent debridement. Excessive debridement is detrimental to healing because it causes a disruption of the wound bed. While maintenance debridement is often needed, attempts should be made to limit interruption to the healing process. This means when debridement is performed, care should be taken to remove as much necrotic tissue and biofilm as possible to allow for wound healing. This may require debridement by a medical doctor or surgeon who can debride deeper into viable tissue and a bleeding base.[1]
- Oedema management via positioning. Many chronic wounds are associated with oedema, particularly venous ulcers. Dependent positioning of an extremity will (1) increase oedema, (2) reduce return of blood and lymphatic flow out of the extremity, and (3) increase pain.
- Leg elevation should be higher than the heart and combined with calf pump exercises. If the patient is unable to tolerate or achieve this position, attempt to elevate the distal leg to the level of the hip.
- The only wounds that should be kept dependent are wounds where tissue perfusion is compromised, such as arterial ulcers. In this case, gravity can help to improve blood flow to the wound.[1]
- Topical antiseptics and antibiotic ointments.
- Cytotoxic antiseptics have a wide spectrum of action on bacteria. However, they also cause an eradication of beneficial bacteria and damage to the healing cells.
- Common examples used in wound care include: (1) betadine (povidone-iodine), (2) Dakin's solution (sodium hypochlorite), (3) chlorhexidine, (4) hydrogen peroxide, (5) Burow's solution (aluminium acetate), and (6)silver nitrate.[1]
- Topical antibiotics have a more narrow spectrum of action and are less cytotoxic than antiseptics. They are typically less destructive to healing cells but can still be detrimental when used inappropriately. Research in both human and animal models has demonstrated that broad-spectrum topical antibiotics slow skin healing.
- Common topical antibiotics used in wound care include: (1) bacitracin, (2) mafenide acetate, (3) mupirocin, (4) neomycin, (5) Neosporin, (6) Polysporin, and (7) silver sulfadiazine.
- In addition to delayed wound healing, some of these products can be harmful to kidney and liver and should be avoided in those with pre-existing kidney or liver impairment.
- Needed indicated, these products are effective when used correctly but should be chosen with careful consideration and used for the shortest amount of time necessary to achieve the desired outcome and minimise detrimental effects.[1]
- Cytotoxic antiseptics have a wide spectrum of action on bacteria. However, they also cause an eradication of beneficial bacteria and damage to the healing cells.
- Local trauma.[1]
- External pressure applied over tissues will collapse capillaries which results in reduced blood flow and tissue oxygenation.
- Friction and shear forces from footwear and dressings can cause tissue damage which can lead to wound formation and also impair current wound healing. This includes bumping, rubbing, scratching, excessive movement, or other disruption of the wound.
- These local traumas can occur through wound cleansing, dressing changes, loose compression dressings, footwear, or patient positioning.
Factors that can Optimise Wound Healing[edit | edit source]
5-key factors that can optimise wound healing:[1]
- Address underlying disease procesess. This can include: (1) blood pressure, (2) blood glucose levels, (3) tissue perfusion, (4) oedema management, (5) reinforce medication compliance, (6) offloading, and (7) pressure relief. The rehabilitation professional can provide education on how these factors can affect wound healing. When appropriate, reinforce treatment plans established by other healthcare providers and refer the patient to other members of the healthcare team as needed.
- Promote nutrition. The rehabilitation professional can (1) refer to a dietitian or nutritionist, (2) reinforce compliance with prescribed diet, (3) emphasise importance of hydration for tissue healing, (4) educate on the benefits of nutrition for healing.
- Exercise and physical activity. Physical activity (1) increases circulation and tissue perfusion, (2) reduces oedema, (3) improves overall health, and can (4) reduce the negative impact of systemic disease.[10]
- Peer support and mindfulness. We know that beliefs and attitudes can contribute to chronic health conditions and this includes chronic wounds. This may mean that the patient puts the onus on the healthcare provider, you, to heal them rather than taking responsibility for the control that they have over their healing process. Alternatively, the patient may feel powerless or feel unsure about how to go about making the recommended changes. Okay. So patients who have been dealing with wounds for a long time and/or have seen multiple healthcare providers may feel hopeless.
- Peer support groups can be helpful in increasing patient adherence to a treatment programme.
- Examples include: (1) walking or exercise groups, (2) nutrition groups, (3) support for health challenges and setbacks, (4) breath-work and breathing exercise groups.
- Mindfulness. Research has found that mindful stress-reduction techniques, relaxation, and guided imagery have been associated with improved wound healing.
- Examples include: (1) positive self-talk about the healing ability of the body, (2) fostering belief in the potential for healing, (3) mindfulness exercises that address tissue oxygenation, nutrition, tissue repair, body resiliency, or (4) turning the focus inward to body repair rather than outward to life stresses. Guided imagery can also be used to talk the patient (1) through the phases of tissue healing, (2) breathwork, (3) directing healing breath and healing cells towards the wound, or (4) positive affirmations. These exercises can be in spoken, written, or audio form. Many patients utilize a combination of these methods.
- Peer support groups can be helpful in increasing patient adherence to a treatment programme.
- Education. Patient education specific to the patient's wound and underlying condition is key yet this is often overlooked as part of the plan of care. Patient understanding of the plan of care and specific recommendations can greatly improve adherence to a treatment plan and improve compliance of interventions that promote healing.
- Patient education should be an interdisciplinary effort and be provided at all levels of the care team.
- It helps with intrinsic versus extrinsic locus-of-control, the patient knows what factors are changeable, what factors can be modified, and what factors are completely within their control.
- Education assists the patient in goal setting and prioritising.
- Patient education can be provided as needed. Rehabilitation professionals are ideal for this role as they often spend more time with the patient and can provide education in smaller and better retained amounts.
Resources[edit | edit source]
- bulleted list
- x
or
- numbered list
- x
References[edit | edit source]
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 1.11 1.12 1.13 1.14 1.15 1.16 1.17 1.18 1.19 1.20 1.21 1.22 1.23 1.24 1.25 1.26 1.27 1.28 1.29 1.30 1.31 1.32 1.33 1.34 1.35 1.36 1.37 1.38 1.39 1.40 1.41 Palmer, D. Physiotherapy Wound Care Programme. Factors Affecting Wound Healing. Plus. 2022.
- ↑ Tipton CD, Wolcott RD, Sanford NE, Miller C, Pathak G, Silzer TK, Sun J, Fleming D, Rumbaugh KP, Little TD, Phillips N. Patient genetics is linked to chronic wound microbiome composition and healing. PLoS pathogens. 2020 Jun 18;16(6):e1008511.
- ↑ Zhu HJ, Fan M, Gao W. Identification of potential hub genes associated with skin wound healing based on time course bioinformatic analyses. BMC surgery. 2021 Dec;21(1):1-3.
- ↑ Engeland CG, Sabzehei B, Marucha PT. Sex hormones and mucosal wound healing. Brain, behavior, and immunity. 2009 Jul 1;23(5):629-35.
- ↑ Polcz ME, Barbul A. The role of vitamin A in wound healing. Nutrition in Clinical Practice. 2019 Oct;34(5):695-700.
- ↑ T. H. Chan School of Public Health, Harvard University. The nutrition source: Vitamin D. Published May, 2020. Accessed October 25, 2021.
- ↑ McDaniel JC, Belury M, Ahijevych K, et al. Omega-3 fatty acids effect on wound healing. Wound Repair Regen. 2008;16(3):337–45.
- ↑ Gouin JP, Kiecolt-Glaser JK. The impact of psychological stress on wound healing: methods and mechanisms. Immunology and Allergy Clinics. 2011 Feb 1;31(1):81-93.
- ↑ Garbarino S, Lanteri P, Bragazzi NL, Magnavita N, Scoditti E. Role of sleep deprivation in immune-related disease risk and outcomes. Communications biology. 2021 Nov 18;4(1):1-7.
- ↑ Keylock KT, Vieira VJ, Wallig MA, et al. Exercise accelerates cutaneous wound healing and decreases wound inflammation in aged mice. Am J Physiol Regul Integr Comp Physiol. 2008;294(1):R179–84

