The Effectiveness of Core Stability Exercise in the Management of Chronic Non-Specific Low Back Pain: Difference between revisions
Kim Jackson (talk | contribs) (Formatting, correct reference formatting, grammar and spelling) |
Kim Jackson (talk | contribs) (Formatting references) |
||
| Line 27: | Line 27: | ||
The first acknowledgment of core stability was by Henry and Florence Kendall who were both Physiotherapist's and first developed the idea of a “neutral pelvis” in 1940/1950’s (Kent 2012). | The first acknowledgment of core stability was by Henry and Florence Kendall who were both Physiotherapist's and first developed the idea of a “neutral pelvis” in 1940/1950’s (Kent 2012). | ||
They initially suggested that the surrounding superficial muscle groups were responsible for the maintenance of alignment and of “neutral spine” . The muscles they were referring to were the erector spinae, hamstrings, abdominals, and the hip flexors. Following on from this, it was suggested that pelvic tilt was pelvic movement deviating from the neutral position. | They initially suggested that the surrounding superficial muscle groups were responsible for the maintenance of alignment and of “neutral spine”. The muscles they were referring to were the erector spinae, hamstrings, abdominals, and the hip flexors. Following on from this, it was suggested that pelvic tilt was pelvic movement deviating from the neutral position. | ||
Over the years, the concept of core stability has changed and authors such as Paul Hodges have highlighted the significance and contribution of the Transverus Abdominus muscle, especially in lumbopelvic stability. Upon this basis, it has now become an important part | Over the years, the concept of core stability has changed and authors such as Paul Hodges have highlighted the significance and contribution of the Transverus Abdominus muscle, especially in lumbopelvic stability. Upon this basis, it has now become an important part of the management of spinal stability and e<span style="line-height: 1.5em;">xercises orientated upon the activation, recruitment, and strengthening of the core are a common avenue of treatment</span><ref>Hodges PW. Is there a role for transversus abdominis in lumbo-pelvic stability?. Manual therapy. 1999 May 1;4(2):74-86.</ref><span style="line-height: 1.5em;">. </span> | ||
== Theories and Applications == | |||
== Theories and Applications | |||
< | In an attempt to add some clarity to the phenomena of the stabilisng system of the spine, Panjabi proposed a classification model that offered an explanation into the functioning of the spine. His model consisted of three categories<ref name=":6">Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. Journal of spinal disorders. 1992 Dec 1;5:390-.</ref><span style="line-height: 1.5em;">Active, Passive and Neural and the evident importance of core stability can be seen.</span> | ||
==== <u> | === Passive === | ||
<u></u>The passive category consists of the basic components of the spine which allow for soft tissue attachment<ref name=":6" />. | |||
* The lumbar vertebrae | |||
* The joint capsules | |||
* The intervertebral disc | |||
* Ligaments surrounding the area | |||
These structures of the spine do not contribute to any significant spinal stability in the neutral alignment. The skeletal structure does support the basic framework and the tensile properties in the various ligaments do start to resist end range movement, however, do not have the capability to produce forces that initiate spinal movement is not caused by the passive structures. | |||
=== Active === | |||
The | <u></u>The active structures hold responsibility for the initiation of gross spinal movement as well as providing contributing to spinal segmentation. <br>Bergmark (1989) further classified the active system into the local and global stabilising system<ref name=":7">Bergmark A. Stability of the lumbar spine: a study in mechanical engineering. Acta Orthopaedica Scandinavica. 1989 Jan 1;60(sup230):1-54.</ref>. The '''local globalising system''' was slated to have a primary role in the maintenance of spinal segment stability and stiffness. The '''global stabilising system''' was stated to be more superficial and with a primary function to generate force to control movement, there is often eccentric contractions to control motion segments throughout the range | ||
<br> | === Global Mobilisers<u></u> === | ||
<u></u>A further active functional classification was suggested by Comerford and Mottram (2001)<ref name=":8">Comerford MJ, Mottram SL. Functional stability re-training: principles and strategies for managing mechanical dysfunction. Manual therapy. 2001 Feb 1;6(1):3-14.</ref>. They have proposed the idea of '''<u>“global mobilisers</u>'''<u></u>”. The primary role of these muscles is for shock absorption and to generate the gross spinal concentric contractions required for gross motor function. | |||
=== Neural<u></u> === | |||
<u></u>The neural component, according to Punjabi, is responsible for receiving information from the various transducers and relaying the relative signal onto the active system to achieve segmental stability. Until sufficient stability has been achieved, the neural components continue to control the active systems.<br> | |||
===== Figure 1. ===== | ===== Figure 1. ===== | ||
A <span style="line-height: 1.5em;">model showing the relationship between the three models proposed by Punjabi (1992), Comerford and Mottram's (2001) and Bergmark (1989), which | A <span style="line-height: 1.5em;">model showing the relationship between the three models proposed by Punjabi (1992), Comerford and Mottram's (2001) and Bergmark (1989), which influence "spinal stability"</span><ref name=":8" /><ref name=":7" /><span style="line-height: 1.5em;">.</span> | ||
[[Image:Spinal assessment types.jpg]] | [[Image:Spinal assessment types.jpg]] | ||
| Line 81: | Line 60: | ||
===== Figure 2. ===== | ===== Figure 2. ===== | ||
A table proposed by Norris (2008), identifying the different characteristics between the stablisers and mobilisers | A table proposed by Norris (2008), identifying the different characteristics between the stablisers and mobilisers<ref name=":9">Norris CM. Back stability: integrating science and therapy. Human Kinetics; 2008.</ref>. | ||
< | |||
< | |||
[[Image:Spinal assessment 2.png]]<ref name=":9" /> | |||
== Relevant anatomy == | == Relevant anatomy == | ||
| Line 233: | Line 205: | ||
= References = | = References = | ||
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006 Mar;15 Suppl 2:S192-300.<span style="line-height: 1.5em;">.</span><span style="line-height: 1.5em;"> </span> | Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006 Mar;15 Suppl 2:S192-300.<span style="line-height: 1.5em;">.</span><span style="line-height: 1.5em;"> </span> | ||
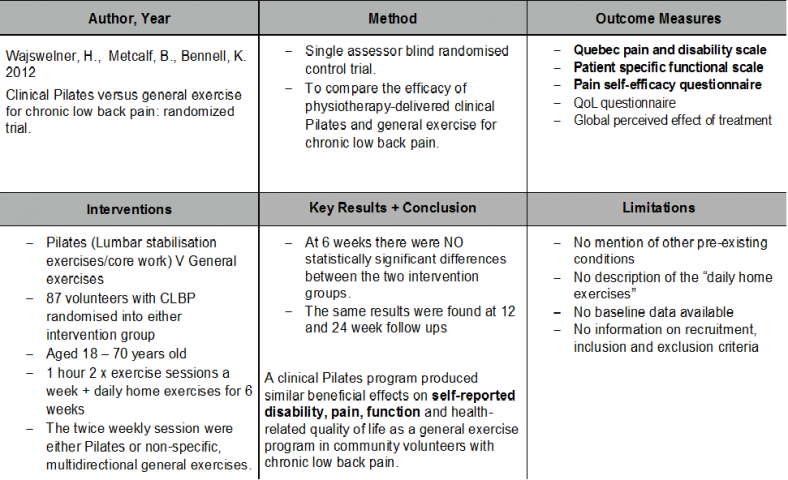
Gladwell ,Valerie, Samantha Head, Martin Haggar And Ralph Beneke. Does a Program of Pilates Improve Chronic Non-Specific Low Back Pain? Journal of sports rehabilitation, 2006, 15, 338-350 | Gladwell ,Valerie, Samantha Head, Martin Haggar And Ralph Beneke. Does a Program of Pilates Improve Chronic Non-Specific Low Back Pain? Journal of sports rehabilitation, 2006, 15, 338-350 | ||
| Line 250: | Line 218: | ||
Mcgill, SM and RW Norman. Reassessment of the role of intra-abdominal pressure in spinal compression. Ergonomics, 1987, 30(11):1565-88 | Mcgill, SM and RW Norman. Reassessment of the role of intra-abdominal pressure in spinal compression. Ergonomics, 1987, 30(11):1565-88 | ||
Putnam, CA. Sequential motions of body segments in striking and throwing skills: descriptions and explanations. Journal of Biomechanics, 1993, 26 (1):125-35 | Putnam, CA. Sequential motions of body segments in striking and throwing skills: descriptions and explanations. Journal of Biomechanics, 1993, 26 (1):125-35 | ||
Revision as of 19:55, 4 January 2020
Top Contributors - Josh Plail, Yann Moysey, Timothy Sheehy, Samuel Soroya, Kim Jackson, Rachael Lowe and Admin
Introduction[edit | edit source]

Low back pain is an extremely common patient complaint with approximately 80% of the World population developing low back pain at some point[1]. 1/3 of the UK population will experience back pain each year[2]. It is the main cause of years lived with disability[3]. It is among 10 of the leading reasons for patient visits to medical facilities.[4] Non-specific low back pain is tension/soreness and or stiffness in the lower back region whereby it is not possible to find a cause for the pain[2]. Most cases resolve fairly quickly, but a significant number of patients develop chronic lower back pain. Patients experience unremitting pain and often become functionally impaired. Chronic LBP represents a greater financial burden in the form of direct costs resulting from loss of work and medical expenses, as well as indirect costs[5].
Prevalence[edit | edit source]
Generally there is a scarcity of information on the prevalence and incidence of chronic low back pain, partly due to lack of agreement about its definition. Chronic low back pain is mostly defined as persistent pain occurring on most days and lasting longer than 3 months[6][7][8]. Others also define it as pain exceeding normal healing times and frequently reoccurring back pain over long periods. Acute and chronic LBP warrant separate consideration as they may respond differently to the same interventions[9][10].
Causes[edit | edit source]
Mechanical disorders are the cause in 90% of cases with the remaining 10% of cases being due to manifestation of systemic illness[11]. Despite a large number of pathological conditions that give rise to low back pain cases, 85% are without pathoanatomical or radiological abnormalities[1]. Most episodes of low back pain resolve quickly and are not incapacitating, nonetheless, pain and disability are often ongoing and recurrences are common[12]. It is estimated 10 to 20% of affected adults develop symptoms of chronic low back painback-pain[13].

Risk Factors[edit | edit source]
Many different patient characteristics have been described that predict who is at risk of developing chronic LBP. However, only a few have been replicated consistently in multiple studies. These include increasing age, previous back pain, job dissatisfaction, pain below the knee and depression.[14][15][16] Depression has long been noted to be associated with various chronic pain syndromes, and several studies have reported it’s relationship with chronic back pain in particular in multiple studies[16]. Women are more commonly affected with LBP and some studies show increases in chronic LBP[15]. Thomas et al. (1999) found that persistent back pain was associated with “premorbid factors” such as poor baseline functional status, high levels of psychological stress, poor self-rated health, low levels of physical activity, smoking and obesity[17]. Smoking has been found in multiple epidemiological studies to be a risk factor for the development of chronic low back pain[18].
Prognosis[edit | edit source]
The longer the patient suffers from back pain the worse the prognosis. The chance of low back pain resolving is its highest during the first week[14]. By the end of year one that chance diminishes significantly. In Van den Hoogen et al. 1998's study on the course of low back pain, 35% patients had pain at 12 weeks and 10% of patients had pain at 1 year.[19] Thomas et al. 1999 reported similar outcomes at 1 year with 10% of patients complaining of the same back pain form the first episode[17]. Carey et al. 2000 found that 2/3 of patients with chronic low back pain at 3 months still had functionally disabling symptoms at 22months and only 16% of patients became symptom-free[20]. Most patients on disability for more than 6 months will not return to work. The number of patients returning to work approaches zero at 2 years[14]. Once established, chronic low back pain is persistent and achieving complete remission becomes less likely as time goes by. The question remains how to treat chronic low back pain, and can you prevent it from occurring in the first place?
Core Stability[edit | edit source]
Many authors have attempted to define core stability, which consequently means a globally accepted definition is yet to be confirmed[21]. However, a widely accepted definition of core stability is:
“Comprises of the lumbopelvic-hip complex and is the capacity to maintain the equilibrium of the vertebral column within its physiologic limits by reducing displacement from perturbations and maintaining structural integrity.”[22][23][24][25][26]
The first acknowledgment of core stability was by Henry and Florence Kendall who were both Physiotherapist's and first developed the idea of a “neutral pelvis” in 1940/1950’s (Kent 2012).
They initially suggested that the surrounding superficial muscle groups were responsible for the maintenance of alignment and of “neutral spine”. The muscles they were referring to were the erector spinae, hamstrings, abdominals, and the hip flexors. Following on from this, it was suggested that pelvic tilt was pelvic movement deviating from the neutral position.
Over the years, the concept of core stability has changed and authors such as Paul Hodges have highlighted the significance and contribution of the Transverus Abdominus muscle, especially in lumbopelvic stability. Upon this basis, it has now become an important part of the management of spinal stability and exercises orientated upon the activation, recruitment, and strengthening of the core are a common avenue of treatment[27].
Theories and Applications[edit | edit source]
In an attempt to add some clarity to the phenomena of the stabilisng system of the spine, Panjabi proposed a classification model that offered an explanation into the functioning of the spine. His model consisted of three categories[28]Active, Passive and Neural and the evident importance of core stability can be seen.
Passive[edit | edit source]
The passive category consists of the basic components of the spine which allow for soft tissue attachment[28].
- The lumbar vertebrae
- The joint capsules
- The intervertebral disc
- Ligaments surrounding the area
These structures of the spine do not contribute to any significant spinal stability in the neutral alignment. The skeletal structure does support the basic framework and the tensile properties in the various ligaments do start to resist end range movement, however, do not have the capability to produce forces that initiate spinal movement is not caused by the passive structures.
Active[edit | edit source]
The active structures hold responsibility for the initiation of gross spinal movement as well as providing contributing to spinal segmentation.
Bergmark (1989) further classified the active system into the local and global stabilising system[29]. The local globalising system was slated to have a primary role in the maintenance of spinal segment stability and stiffness. The global stabilising system was stated to be more superficial and with a primary function to generate force to control movement, there is often eccentric contractions to control motion segments throughout the range
Global Mobilisers[edit | edit source]
A further active functional classification was suggested by Comerford and Mottram (2001)[30]. They have proposed the idea of “global mobilisers”. The primary role of these muscles is for shock absorption and to generate the gross spinal concentric contractions required for gross motor function.
Neural[edit | edit source]
The neural component, according to Punjabi, is responsible for receiving information from the various transducers and relaying the relative signal onto the active system to achieve segmental stability. Until sufficient stability has been achieved, the neural components continue to control the active systems.
Figure 1. [edit | edit source]
A model showing the relationship between the three models proposed by Punjabi (1992), Comerford and Mottram's (2001) and Bergmark (1989), which influence "spinal stability"[30][29].

Figure 2.[edit | edit source]
A table proposed by Norris (2008), identifying the different characteristics between the stablisers and mobilisers[31].

Relevant anatomy[edit | edit source]

(Kibler, Press and Sciascia 2006)
Physiology[edit | edit source]



It has been stated that core is characterised by “Proximal stability for distal mobility” (Putnam 1993, Zattara and Bouisset 1988)
When contracting, the primary role of the core stability muscles is to raise the intra-abdominal pressure and to increase the tension in the thoracolumbar fascia.
The increase in intra-abdominal pressure stiffens and strengthens the relevant structural support around the spine, compacts the arthrogenic structures and in combination with abdominal contraction, it can encourage a rigid cyclinder and stiffness to occur around the spine (McGill and Norman 1987).
This gives the spine a relative degree of stability which is needed to facilitate superficial muscle activation and gross motor action.
Core stability functions[edit | edit source]
• Anticipatory postural adjustments – pre-programmed muscle activation which helps the body to anticipate the subsequent force
• To create interactive moments that help to control the exposure of force and loading that is applied to a joint
• To help in force control throughout the various locations in the body
(Kibler, Press and Sciascia 2006)
Typical core exercises[edit | edit source]
A lumbo-pelivic stability programme is constructed in three sections (Richardson, Hodges and Hides (2004).
Section 1 - Entails segmental control and active recruitment over global mobilisers - specifically transversus abdominus, pelvic floor and diaphragm
Section 2 - Whislt maintianing segmental control and activation, introducing closed chain exercises, with low velocity and low load.
Section 3 - Whilst maintaining segmental control, introducing open chain exercises with high velocity and load. Movement of adjacent body segements can be used to stress the core structures
Many of the specific exercises listed below have been proven to significantly increase general health, sports functioning, and significantly decrease in pain.(Gladwell, Head, Haggar et al 2006)
Phase 2[edit | edit source]
Bridging
Single leg fall out
Single leg extension in supine
Basic 4 point Kneeling
Advanced 4 point Kneeling
The modified one leg stretch: Crook lying, slide one leg away as far as possible and then return to start position.
The modified shoulder bridge: Crook lying, “peeling” the bottom off the mat. Progression: Increase the range of movement (more of the spine away from the mat).
Swimming (a modification from a four point base): Box position, slide one foot along the floor behind, return to the start position. Repeat on other leg.
Phase 3.[edit | edit source]
Bridging progression onto a pilates ball
Pilates ball plank
Recent Evidence[edit | edit source]
This chapter will look at the evidence which shows positive effects and ambiguity of core stability for chronic low back pain. The European Guidelines have stated that the following are recommended in the management of chronic non-specific low back pain: cognitive behavioural therapy, exercise therapy and educational therapy (Airaksinen el al, 2006). When searching the literature, studies only compared core stability exercise with general exercise therapy out of the European Guidelines recommendations.
Pain and function were selected as outcome measures to determine the effectiveness of core stability exercises as these were the consistent outcome measures in the evidence and have been shown to be major factor of psychosocial well-being of patients (Gureje et al, 1998; Stevens et al, 1996).
Evidence For[edit | edit source]

Evidence Against[edit | edit source]
 [edit | edit source]
[edit | edit source]


Conclusion[edit | edit source]
The meta-analysis showed core stability exercise has signficant improvement in both pain and function compared to general exercise for patients with chronic low back pain. However these findings were only significant in the short term. In contrast, evidence published since this meta-analysis has found no significant difference between core stability and general exercises neither short term nor long term even though both interventions did improve pain and function. It should be noted though that no study reported adverse effects from core stability exercise when compared to general exercise with respect to pain and function.
In conclusion these findings show that clinicians have a choice to either administer core stability exercise or general exercise when a patient has chronic non-specific low back pain. Core stability exercise can be used as an alternative to general strengthening and stretching if patient is more suitable and if it would encourage compliance. However clinicians should not expect a significant improvement by choosing core stability in regards to pain and function especially in the long term.
Limitations[edit | edit source]
The wealth of literature available compared core stability exercises to general exercise. Although there is literature to support the use of other therapies e.g. CBT, mobilisations and pharmacology they have not been compared directly to core stability exercises. Therefore further research is required into these areas.
References[edit | edit source]
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006 Mar;15 Suppl 2:S192-300..
Gladwell ,Valerie, Samantha Head, Martin Haggar And Ralph Beneke. Does a Program of Pilates Improve Chronic Non-Specific Low Back Pain? Journal of sports rehabilitation, 2006, 15, 338-350
Gureje O, Von Korff M, Simon GE, Gater R. Persistent pain and well-being: a World Health Organization Study in Primary Care. JAMA. 1998 Jul 8;280(2):147-51.
Kent, Christine. The end of the “neutral pelvis” – part 1[online]. Albuquerque, 2012 [ 10/01/14]. Available from: http://wholewoman.com/blog/?p=1074
Kibler, Ben W, Joel Press and Aaron Sciascia. The role of core stability in athletic function, Sports medicine, 2006, 36(3): 189-98
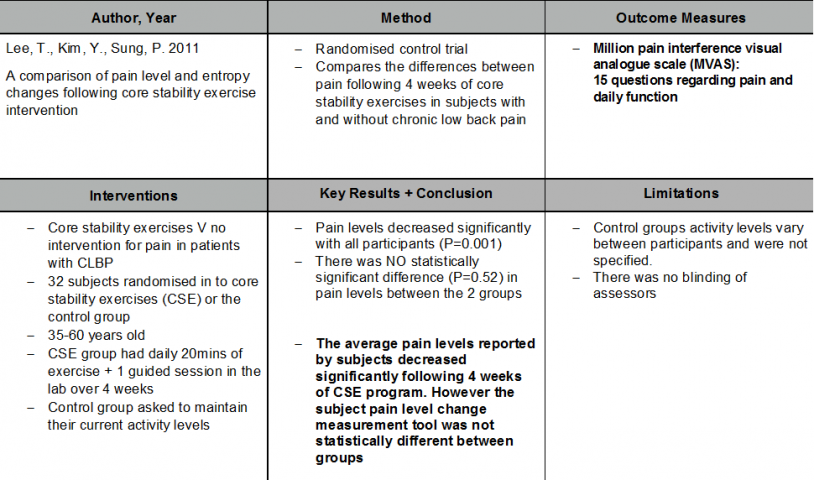
Lee, T., Kim, Y., Sung, P. (2011) A comparison of pain level and entropy changes following core stability exercise intervention. International medical journal of experimental and clinical research. 17(7): pp.362-368
Mcgill, SM and RW Norman. Reassessment of the role of intra-abdominal pressure in spinal compression. Ergonomics, 1987, 30(11):1565-88
Putnam, CA. Sequential motions of body segments in striking and throwing skills: descriptions and explanations. Journal of Biomechanics, 1993, 26 (1):125-35
Richardson CA, PW Hodges, J Hides. Therapeutic Exercise for Lumbo-pelvic Stabilization: A Motor Control Approach for the Treatment and Prevention of Low Back Pain. 2 edition. Edinburgh: Churchill Livingstone; 2004.
Savigny, P., Watson, P., & Underwood, M. (2009). Early management of persistent non-specific low back pain: summary of NICE guidance. BMJ, 338.
Stevens SE, Steele CA, Jutai JW, Kalnins IV, Bortolussi JA, Biggar WD. Adolescents with physical disabilities: some psychosocial aspects of health. J Adolesc Health. 1996 Aug;19(2):157-64.
Wajswelner, H., Metcalf, B., Bennell, K. (2012). Clinical pilates versus general exercise for chronic low back pain: randomized trial. Medicine and science in sports and exercise. 44(7): pp.1197-1205
Wang XQ, Zheng JJ, Yu ZW, Bi X, Lou SJ, Liu J, Cai B, Hua YH, Wu M, Wei ML, Shen HM, Chen Y, Pan YJ, Xu GH, Chen PJ. A meta-analysis of core stability exercise versus general exercise for chronic low back pain.PLoS One. 2012;7(12):e52082.
- ↑ 1.0 1.1 Deyo RA, Weinstein JN. New England Journal of Medicine. NEJM. 2001;344(5)):363-70.
- ↑ 2.0 2.1 Savigny P, Watson P, Underwood M. Early management of persistent non-specific low back pain: summary of NICE guidance. Bmj. 2009 Jun 4;338:b1805.
- ↑ Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S, Aboyans V, Abraham J. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The lancet. 2012 Dec 15;380(9859):2163-96.
- ↑ Patel AT, Ogle AA. Diagnosis and management of acute low back pain. American family physician. 2000 Mar;61(6):1779-86.
- ↑ Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. The spine journal. 2008 Jan 1;8(1):8-20.
- ↑ Maher CG. Effective physical treatment for chronic low back pain. Orthopedic Clinics. 2004 Jan 1;35(1):57-64.
- ↑ Von Korff M, Saunders K. The course of back pain in primary care. Spine. 1996 Dec 15;21(24):2833-7.
- ↑ Waddell G, Schoene M. The back pain revolution. Elsevier Health Sciences; 2004.
- ↑ Sierpina V, Curtis P, Doering J. An integrative approach to low back pain. Clinics in Family Practice. 2002 Dec;4(4):817-31.
- ↑ Van Tulder MW, Koes BW, Bouter LM. Conservative treatment of acute and chronic nonspecific low back pain: a systematic review of randomized controlled trials of the most common interventions. Spine. 1997 Sep 15;22(18):2128-56.
- ↑ Nachemson AL. The lumbar spine an orthopaedic challenge. spine. 1976 Mar 1;1(1):59-71.
- ↑ Pengel LH, Herbert RD, Maher CG, Refshauge KM. Acute low back pain: systematic review of its prognosis. Bmj. 2003 Aug 7;327(7410):323.
- ↑ Diamond S, Borenstein D. Chronic low back pain in a working-age adult. Best practice & research Clinical rheumatology. 2006 Aug 1;20(4):707-20.
- ↑ 14.0 14.1 14.2 Andersson GB. The epidemiology of spinal disorders. Frymoyer JW The adult spine: principles and practice. 1997. Philadelphia.
- ↑ 15.0 15.1 Cherkin DC, Deyo RA, Street JH, Barlow W. Predicting poor outcomes for back pain seen in primary care using patients' own criteria. Spine. 1996 Dec 15;21(24):2900-7.
- ↑ 16.0 16.1 Epping-Jordan JE, Wahlgren DR, Williams RA, Pruitt SD, Slater MA, Patterson TL, Grant I, Webster JS, Atkinson JH. Transition to chronic pain in men with low back pain: predictive relationships among pain intensity, disability, and depressive symptoms. Health Psychology. 1998 Sep;17(5):421.
- ↑ 17.0 17.1 Thomas E, Silman AJ, Croft PR, Papageorgiou AC, Jayson MI, Macfarlane GJ. Predicting who develops chronic low back pain in primary care: a prospective study. Bmj. 1999 Jun 19;318(7199):1662-7.
- ↑ Deyo RA, Bass JE. Lifestyle and low-back pain. The influence of smoking and obesity. Spine. 1989 May;14(5):501-6.
- ↑ van den Hoogen HJ, Koes BW, van Eijk JT, Bouter LM, Devillé W. On the course of low back pain in general practice: a one year follow up study. Annals of the rheumatic diseases. 1998 Jan 1;57(1):13-9.
- ↑ Carey TS, Garrett JM, Jackman AM. Beyond the good prognosis: examination of an inception cohort of patients with chronic low back pain. Spine. 2000 Jan 1;25(1):115.
- ↑ Huxel Bliven KC, Anderson BE. Core stability training for injury prevention. Sports health. 2013 Nov;5(6):514-22.
- ↑ Akuthota V, Nadler SF. Core strengthening. Archives of physical medicine and rehabilitation. 2004 Mar 1;85:86-92.
- ↑ Liemohn WP, Baumgartner TA, Gagnon LH. Measuring core stability. Journal of Strength and Conditioning Research. 2005 Aug 1;19(3):583.
- ↑ Panjabi MM. Clinical spinal instability and low back pain. Journal of electromyography and kinesiology. 2003 Aug 1;13(4):371-9.
- ↑ Smith CE, Nyland J, Caudill P, Brosky J, Caborn DN. Dynamic trunk stabilization: a conceptual back injury prevention program for volleyball athletes. journal of orthopaedic & sports physical therapy. 2008 Nov;38(11):703-20.
- ↑ Willson JD, Dougherty CP, Ireland ML, Davis IM. Core stability and its relationship to lower extremity function and injury. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2005 Sep 1;13(5):316-25.
- ↑ Hodges PW. Is there a role for transversus abdominis in lumbo-pelvic stability?. Manual therapy. 1999 May 1;4(2):74-86.
- ↑ 28.0 28.1 Panjabi MM. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis. Journal of spinal disorders. 1992 Dec 1;5:390-.
- ↑ 29.0 29.1 Bergmark A. Stability of the lumbar spine: a study in mechanical engineering. Acta Orthopaedica Scandinavica. 1989 Jan 1;60(sup230):1-54.
- ↑ 30.0 30.1 Comerford MJ, Mottram SL. Functional stability re-training: principles and strategies for managing mechanical dysfunction. Manual therapy. 2001 Feb 1;6(1):3-14.
- ↑ 31.0 31.1 Norris CM. Back stability: integrating science and therapy. Human Kinetics; 2008.

