Stroke Medical Management: Difference between revisions
No edit summary |
No edit summary |
||
| Line 6: | Line 6: | ||
== Introduction == | == Introduction == | ||
The team approach to stroke management starts with Emergency Medical Services and continues at a hospital within a Stroke System of Care capable of delivering Acute Stroke Care in the Emergency Department and in a dedicated Stroke Unit.The goal for the acute medical management of patients with stroke is to stabilize the patient and to complete initial evaluation and assessment, including imaging and laboratory studies, within a short time frame. Critical decisions focus on the need for intubation, blood pressure control, and determination of risk / benefit for thrombolytic intervention.<ref>Adams H, Adams R, Del Zoppo G, Goldstein LB. Guidelines for the early management of patients with ischemic stroke: 2005 guidelines update a scientific statement from the Stroke Council of the American Heart Association/American Stroke Association. Stroke. Apr 2005;36(4):916-23.</ref> Patients presenting with Glasgow Coma Scale scores of 8 or less or rapidly decreasing Glasgow Coma Scale scores, require emergent airway control via intubation.<br> | The team approach to stroke management starts with Emergency Medical Services and continues at a hospital within a Stroke System of Care capable of delivering Acute Stroke Care in the Emergency Department and in a dedicated Stroke Unit.The goal for the acute medical management of patients with stroke is to stabilize the patient and to complete initial evaluation and assessment, including imaging and laboratory studies, within a short time frame. Critical decisions focus on the need for intubation, blood pressure control, and determination of risk / benefit for thrombolytic intervention.<ref>Adams H, Adams R, Del Zoppo G, Goldstein LB. Guidelines for the early management of patients with ischemic stroke: 2005 guidelines update a scientific statement from the Stroke Council of the American Heart Association/American Stroke Association. Stroke. Apr 2005;36(4):916-23.</ref> Patients presenting with Glasgow Coma Scale scores of 8 or less or rapidly decreasing Glasgow Coma Scale scores, require emergent airway control via intubation.<br> | ||
Goals of Emergency Management | Goals of Emergency Management | ||
*Support Vital Functions | *Support Vital Functions | ||
*Restore Cerebral Circulation | *Restore Cerebral Circulation | ||
*Reduce Neurological Deficits | *Reduce Neurological Deficits | ||
*Prevent Progression and Cell Death | *Prevent Progression and Cell Death | ||
*Restore Patient to Optimal Level of Pre-Stroke Function<br> | *Restore Patient to Optimal Level of Pre-Stroke Function<br> | ||
| Line 20: | Line 20: | ||
| colspan="2" align="center" | '''American Stroke Association Stroke Chain of Survival''' | | colspan="2" align="center" | '''American Stroke Association Stroke Chain of Survival''' | ||
|- | |- | ||
| '''Detection''' | | '''Detection''' | ||
| nowrap="nowrap" | | | nowrap="nowrap" | | ||
Patient/Bystander or EMS recognition of Stroke Signs & Symptoms | Patient/Bystander or EMS recognition of Stroke Signs & Symptoms | ||
|- | |- | ||
| '''Dispatch''' | | '''Dispatch''' | ||
| | | | ||
EMS Activation; Priority Dispatch & Response | EMS Activation; Priority Dispatch & Response | ||
|- | |- | ||
| '''Delivery''' | | '''Delivery''' | ||
| nowrap="nowrap" | | | nowrap="nowrap" | | ||
Prompt Triage - In the interest of saving time, some EMS actions can be accomplished enroute. | Prompt Triage - In the interest of saving time, some EMS actions can be accomplished enroute. | ||
Limit assessments / Care on scene to those that are urgently needed or clearly indicated by the patients presentation. | Limit assessments / Care on scene to those that are urgently needed or clearly indicated by the patients presentation. | ||
Transport to most appropriate Stroke Hospital | Transport to most appropriate Stroke Hospital | ||
Prehospital Notification | Prehospital Notification | ||
|- | |- | ||
| '''Door''' | | '''Door''' | ||
| nowrap="nowrap" | | | nowrap="nowrap" | | ||
Immediate Emergency Department triage to high-acuity area | Immediate Emergency Department triage to high-acuity area | ||
|- | |- | ||
| '''Data''' | | '''Data''' | ||
| nowrap="nowrap" | | | nowrap="nowrap" | | ||
Prompt Emergency Department Evaluation. | Prompt Emergency Department Evaluation. | ||
Stroke Team Activation | Stroke Team Activation | ||
Lab Studies and Brain Imaging | Lab Studies and Brain Imaging | ||
Time barriers at the hospital which should be minimised: | Time barriers at the hospital which should be minimised: | ||
*Time to Treatment Area | *Time to Treatment Area | ||
*Time to Physician Assessment | *Time to Physician Assessment | ||
*Time to CT (Goal ≤ 25 min.) | *Time to CT (Goal ≤ 25 min.) | ||
*Time for CT Interpretation (Goal ≤ 45 min.) | *Time for CT Interpretation (Goal ≤ 45 min.) | ||
*Time for Consultation | *Time for Consultation | ||
*Time for Decision | *Time for Decision | ||
*Time for Consent | *Time for Consent | ||
*Time for Preparation | *Time for Preparation | ||
|- | |- | ||
| '''Decision''' | | '''Decision''' | ||
| nowrap="nowrap" | | | nowrap="nowrap" | | ||
Diagnosis and determination of most appropriate therapy; | Diagnosis and determination of most appropriate therapy; | ||
Discussion with Patient and Family | Discussion with Patient and Family | ||
|- | |- | ||
| nowrap="nowrap" | '''Drug''' | | nowrap="nowrap" | '''Drug''' | ||
| | | | ||
<span style="white-space: nowrap;">Administration of appropriate Drugs / Treatment / Interventions </span><br> | <span style="white-space: nowrap;">Administration of appropriate Drugs / Treatment / Interventions </span><br> | ||
<span style="white-space: nowrap;" />Tissue Plasminogen Activator (tPa) for the treatment of acute ischemic stroke must be given within 4.5 hours from the onset of symptoms. Ideally, tPA should be administered (“door to drug”) in less than 60 minutes after Emergency Department arrival. Evidence confirms that the sooner tPA is administered, the more optimal the results. | |||
|- | |- | ||
| '''<span style="white-space: nowrap;">Disposition</span>''' | | '''<span style="white-space: nowrap;">Disposition</span>''' | ||
| | | | ||
Timely Admission to Stroke Unit, ICU, or Transfer | Timely Admission to Stroke Unit, ICU, or Transfer | ||
Outcomes are best when patients are admitted directly to and receive care in a dedicated stroke unit, where recovery and rehab can begin immediately. Hospitals without full stroke care capabilities should have official transfer agreements with hospitals offering a full complement of stroke care, and patients should be transferred as soon as reasonably possible. | Outcomes are best when patients are admitted directly to and receive care in a dedicated stroke unit, where recovery and rehab can begin immediately. Hospitals without full stroke care capabilities should have official transfer agreements with hospitals offering a full complement of stroke care, and patients should be transferred as soon as reasonably possible. | ||
|} | |} | ||
| Line 90: | Line 90: | ||
== Suspected Stroke Algorithm == | == Suspected Stroke Algorithm == | ||
== [[Image:15-1043 l 1.jpg|center]]Imaging == | |||
According to Prasad (2011) brain imaging should be performed immediately for patients with persistent neurological symptoms if any of the following apply<ref name="Prasad">Prasad K, Kaul S, Padma MV, Gorthi SP, Khurana D, Bakshi A. Stroke management. Annals of Indian Academy of Neurology. 2011 Jul 1;14(5):82.</ref>: | |||
*Indication for thrombolysis or early anticoagulation. | |||
*On Anticoagulant Treatment | |||
*Known Bleeding Tendency | |||
*Depressed Level of Consciousness (GCS below 13) | |||
*Severe Headache at onset of Stroke Symptoms | |||
*Papilloedema, Neck Stiffness, Subhyaloid Hemorrhage or Fever | |||
< | Patients with acute stroke without the above indications for immediate brain imaging, scanning should be performed within 24 hours after onset of symptoms. | ||
'''''Level I Clinical Guideline Recommendations''''' | |||
*Emergency imaging of the brain is recommended before initiating any specific treatment for acute stroke (Class I; Level of Evidence A). In most instances, nonenhanced CT will provide the necessary information to make decisions about emergency management. (Unchanged from the 2013 Guideline)<ref name="Powers">Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, Johnston KC, Johnston SC, Khalessi AA, Kidwell CS, Meschia JF. 2015 AHA/ASA focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment. Stroke. 2015 Jan 1:STR-0000000000000074.</ref> | |||
*If Endovascular Therapy is contemplated, a noninvasive intracranial vascular study is strongly recommended during the initial imaging evaluation of the acute stroke patient but should not delay intravenous r-tPA if indicated. For patients who qualify for intravenous r-tPA according to guidelines from professional medical societies, initiating intravenous r- tPA before noninvasive vascular imaging is recommended for patients who have not had noninvasive vascular imaging as part of their initial imaging assessment for stroke. Noninvasive intracranial vascular imaging should then be obtained as quickly as possible (Class I; Level of Evidence A). (New recommendation)<ref name="Powers" /> | |||
== Ischemic Stroke == | == Ischemic Stroke == | ||
In the case of an Ischemic Stroke, the more rapidly blood flow is restrored, the ore likely for improved recovery and fewer brain cell deaths. Primary treatment is aimed at breaking down the clot through means of medication (Thrombolysis) or mechanical removal of clot (Thrombectomy). Other treatments aim to | In the case of an Ischemic Stroke, the more rapidly blood flow is restrored, the ore likely for improved recovery and fewer brain cell deaths. Primary treatment is aimed at breaking down the clot through means of medication (Thrombolysis) or mechanical removal of clot (Thrombectomy). Other treatments aim to minimise the clot becoming larger or prevention of new clot formation by means of anticoagulant type medications such as Aspirin, Clopidogrel or Dipyridamole. In conjunction with this, overall patient medical condition should be managed including montoring of blood sugars, oxygen levels and hydration and providing adequate treatment for same<ref>Verheyen G and Ashbury A. IN Physical Management for Neurological Conditions 3rd Edition. Southampton: Elsevier 2011 pp.12-13</ref>. | ||
*All patients with disabling acute ischemic stroke who can be treated within 3 - 4.5 hours after symptom onset should be evaluated without delay to determine their eligibility for treatment with intravenous tissue plasminogen activator. | |||
=== Thrombolysis === | === Thrombolysis === | ||
Rapid administration of intravenous recombinant tissue-type plasminogen activator (r-tPA) to appropriate patients remains the mainstay of early treatment of acute ischemic stroke. For patients who meet national and international eligibility guidelines, intravenous r-tPA administration improves functional outcomes at 3 to 6 months when given within 4.5 hours of Ischemic Stroke Onset and should be administered. Every effort should be made to shorten any delays in initiation of treatment as earlier treatments are associated with increased benefits. | |||
tPA | The goal of therapy for ischemic stroke is to safely maximize patient functional recovery to pre-stroke baseline by rapidly reperfusing the ischemic penumbra. tPA has optimal use within 3 hours from onset of symptoms but in carefully selected patients there is a longer time window for treatment up to 4.5 hours. Studies continue to support that time from onset to treatment with tPA is directly related to outcomes in Ischemic Stroke. The sooner tPA is given, the greater the benefit (Stroke, 2013). | ||
Beyond the approved and recommended time windows for tPA use, risk of complications rises. tPA is no different from other medications in that it has potential adverse effects, which makes it essential that a careful consideration is given to exclusion criteria, risks and benefits for use in each individual patient. The major complications is symptomatic intracranial hemorrhage which occurs at a rate of roughly 5.2%. Other complications include orolingual angioedema (allergic reaction), acute hypotension, and systemic bleeding. (Circulation 2010: Part 11: Adult Stroke).<br> | |||
'''''Level I Clinical Guideline Recommendations''''' | |||
*Patients eligible for intravenous r-tPA should receive intravenous r-tPA even if endovascular treatments are being considered (Class I; Level of Evidence A). (Unchanged from the 2013 Guideline)<ref name="Powers" /> | |||
=== Endovascular Therapy === | |||
Clot retrieval devices: There are currently four FDA- approved devices for clot disruption or removal.<br>The Mechanical Embolus Removal in Cerebral Ischemia (MERCI) Thrombectomy System is a looped wire with progressively smaller helical loops, advanced via a small catheter through the clot. As the catheter is withdrawn, the coiled wire is deployed, which captures the clot for removal. | |||
Complications from clot retrieval procedures include hemorrhage, internal bleeding, death and recurrence of stroke. | The Penumbra Thrombectomy System is designed to aspirate clots from large intracranial vessels. With a suction catheter at the proximal end of the clot, the device continuously debulks and aspirates clot debris until the vessel is clear. The device can remove a clot in a matter of minutes,<br>whereas fibrinolytics, even those delivered intra-arterially, may take as long as 2 hours to dissolve a thrombus. | ||
The Solitaire Flow Restoration device and the Trevo Retriever device have the unique ability to both immediately bypass the clot and restore flow and retrieve the clot. | |||
Studies have shown that when clot retrieval is performed within eight hours of symptom onset, 60-68% of patients achieved post-procedure revascularization. Patients eligible for clot retrieval are those with recent ischemic stroke, who can receive treatment within at least 12 (preferably 3-6) hours of the onset of stroke. Those patients with uncontrolled HTN, internal bleeding, seizures, blood clotting problems, or those on anticoagulants are not candidates for this procedure.<br> | |||
Complications from clot retrieval procedures include hemorrhage, internal bleeding, death and recurrence of stroke. | |||
'''''Level I Clinical Guideline Recommendations''''' | |||
*Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria (Class I; Level of Evidence A). (New Recommendation):<br> (a) Prestroke mRS score 0 to 1,<br>(b) Acute ischemic stroke receiving intravenous r-tPA within 4.5 hours of onset according to guidelines from professional medical societies,<br>(c) Causative Occlusion of the Internal Carotid Artery or Proximal MCA (M1),<br>(d) Age ≥18 Years,<br>(e) NIHSS Score of ≥6,<br>(f) ASPECTS of ≥6, and<br>(g) Treatment can be initiated (groin puncture) within 6 hours of symptom onset<ref name="Powers" /> | |||
*Reduced time from symptom onset to reperfusion with endovascular therapies is highly associated with better clinical outcomes. To ensure benefit, reperfusion to TICI Grade 2b/3 should be achieved as early as possible and within 6 hours of Stroke Onset (Class I; Level of Evidence B-R). (Revised from the 2013 Guideline)<ref name="Powers" /> | |||
== Haemorrhagic Stroke == | == Haemorrhagic Stroke == | ||
In the case of Haemorrhagic Stroke the main aim is to stop the bleeding as early as possible, often requiring Neurosurgical Intervention. | In the case of Haemorrhagic Stroke the main aim is to stop the bleeding as early as possible, often requiring Neurosurgical Intervention. | ||
== Recent Related Research (from [http://www.ncbi.nlm.nih.gov/pubmed/ Pubmed]) == | == Recent Related Research (from [http://www.ncbi.nlm.nih.gov/pubmed/ Pubmed]) == | ||
<div class="researchbox"> | <div class="researchbox"> | ||
<rss>Feed goes here!!|charset=UTF-8|short|max=10</rss> | <rss>Feed goes here!!|charset=UTF-8|short|max=10</rss> | ||
</div> | </div> | ||
== References == | == References == | ||
References will automatically be added here, see [[Adding References|adding references tutorial]]. | References will automatically be added here, see [[Adding References|adding references tutorial]]. | ||
<references /></div> | <references /></div> | ||
Revision as of 00:41, 7 May 2017
Original Editor - Naomi O'Reilly
Top Contributors - Naomi O'Reilly, Kim Jackson, Lucinda hampton, Admin, Simisola Ajeyalemi, Wanda van Niekerk, 127.0.0.1, Karen Wilson, Claire Knott and Rucha Gadgil
Introduction[edit | edit source]
The team approach to stroke management starts with Emergency Medical Services and continues at a hospital within a Stroke System of Care capable of delivering Acute Stroke Care in the Emergency Department and in a dedicated Stroke Unit.The goal for the acute medical management of patients with stroke is to stabilize the patient and to complete initial evaluation and assessment, including imaging and laboratory studies, within a short time frame. Critical decisions focus on the need for intubation, blood pressure control, and determination of risk / benefit for thrombolytic intervention.[1] Patients presenting with Glasgow Coma Scale scores of 8 or less or rapidly decreasing Glasgow Coma Scale scores, require emergent airway control via intubation.
Goals of Emergency Management
- Support Vital Functions
- Restore Cerebral Circulation
- Reduce Neurological Deficits
- Prevent Progression and Cell Death
- Restore Patient to Optimal Level of Pre-Stroke Function
| American Stroke Association Stroke Chain of Survival | |
| Detection |
Patient/Bystander or EMS recognition of Stroke Signs & Symptoms |
| Dispatch |
EMS Activation; Priority Dispatch & Response |
| Delivery |
Prompt Triage - In the interest of saving time, some EMS actions can be accomplished enroute. Limit assessments / Care on scene to those that are urgently needed or clearly indicated by the patients presentation. Transport to most appropriate Stroke Hospital Prehospital Notification |
| Door |
Immediate Emergency Department triage to high-acuity area |
| Data |
Prompt Emergency Department Evaluation. Stroke Team Activation Lab Studies and Brain Imaging Time barriers at the hospital which should be minimised:
|
| Decision |
Diagnosis and determination of most appropriate therapy; Discussion with Patient and Family |
| Drug |
Administration of appropriate Drugs / Treatment / Interventions <span style="white-space: nowrap;" />Tissue Plasminogen Activator (tPa) for the treatment of acute ischemic stroke must be given within 4.5 hours from the onset of symptoms. Ideally, tPA should be administered (“door to drug”) in less than 60 minutes after Emergency Department arrival. Evidence confirms that the sooner tPA is administered, the more optimal the results. |
| Disposition |
Timely Admission to Stroke Unit, ICU, or Transfer Outcomes are best when patients are admitted directly to and receive care in a dedicated stroke unit, where recovery and rehab can begin immediately. Hospitals without full stroke care capabilities should have official transfer agreements with hospitals offering a full complement of stroke care, and patients should be transferred as soon as reasonably possible. |
Suspected Stroke Algorithm[edit | edit source]
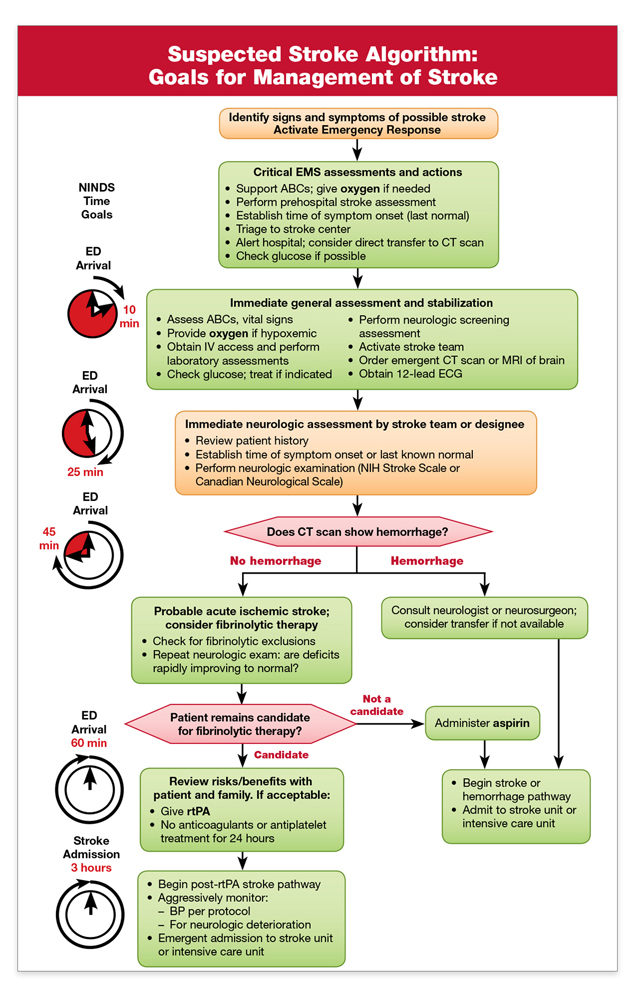 Imaging[edit | edit source]
Imaging[edit | edit source]

According to Prasad (2011) brain imaging should be performed immediately for patients with persistent neurological symptoms if any of the following apply[2]:
- Indication for thrombolysis or early anticoagulation.
- On Anticoagulant Treatment
- Known Bleeding Tendency
- Depressed Level of Consciousness (GCS below 13)
- Severe Headache at onset of Stroke Symptoms
- Papilloedema, Neck Stiffness, Subhyaloid Hemorrhage or Fever
Patients with acute stroke without the above indications for immediate brain imaging, scanning should be performed within 24 hours after onset of symptoms.
Level I Clinical Guideline Recommendations
- Emergency imaging of the brain is recommended before initiating any specific treatment for acute stroke (Class I; Level of Evidence A). In most instances, nonenhanced CT will provide the necessary information to make decisions about emergency management. (Unchanged from the 2013 Guideline)[3]
- If Endovascular Therapy is contemplated, a noninvasive intracranial vascular study is strongly recommended during the initial imaging evaluation of the acute stroke patient but should not delay intravenous r-tPA if indicated. For patients who qualify for intravenous r-tPA according to guidelines from professional medical societies, initiating intravenous r- tPA before noninvasive vascular imaging is recommended for patients who have not had noninvasive vascular imaging as part of their initial imaging assessment for stroke. Noninvasive intracranial vascular imaging should then be obtained as quickly as possible (Class I; Level of Evidence A). (New recommendation)[3]
Ischemic Stroke[edit | edit source]
In the case of an Ischemic Stroke, the more rapidly blood flow is restrored, the ore likely for improved recovery and fewer brain cell deaths. Primary treatment is aimed at breaking down the clot through means of medication (Thrombolysis) or mechanical removal of clot (Thrombectomy). Other treatments aim to minimise the clot becoming larger or prevention of new clot formation by means of anticoagulant type medications such as Aspirin, Clopidogrel or Dipyridamole. In conjunction with this, overall patient medical condition should be managed including montoring of blood sugars, oxygen levels and hydration and providing adequate treatment for same[4].
- All patients with disabling acute ischemic stroke who can be treated within 3 - 4.5 hours after symptom onset should be evaluated without delay to determine their eligibility for treatment with intravenous tissue plasminogen activator.
Thrombolysis[edit | edit source]
Rapid administration of intravenous recombinant tissue-type plasminogen activator (r-tPA) to appropriate patients remains the mainstay of early treatment of acute ischemic stroke. For patients who meet national and international eligibility guidelines, intravenous r-tPA administration improves functional outcomes at 3 to 6 months when given within 4.5 hours of Ischemic Stroke Onset and should be administered. Every effort should be made to shorten any delays in initiation of treatment as earlier treatments are associated with increased benefits.
The goal of therapy for ischemic stroke is to safely maximize patient functional recovery to pre-stroke baseline by rapidly reperfusing the ischemic penumbra. tPA has optimal use within 3 hours from onset of symptoms but in carefully selected patients there is a longer time window for treatment up to 4.5 hours. Studies continue to support that time from onset to treatment with tPA is directly related to outcomes in Ischemic Stroke. The sooner tPA is given, the greater the benefit (Stroke, 2013).
Beyond the approved and recommended time windows for tPA use, risk of complications rises. tPA is no different from other medications in that it has potential adverse effects, which makes it essential that a careful consideration is given to exclusion criteria, risks and benefits for use in each individual patient. The major complications is symptomatic intracranial hemorrhage which occurs at a rate of roughly 5.2%. Other complications include orolingual angioedema (allergic reaction), acute hypotension, and systemic bleeding. (Circulation 2010: Part 11: Adult Stroke).
Level I Clinical Guideline Recommendations
- Patients eligible for intravenous r-tPA should receive intravenous r-tPA even if endovascular treatments are being considered (Class I; Level of Evidence A). (Unchanged from the 2013 Guideline)[3]
Endovascular Therapy[edit | edit source]
Clot retrieval devices: There are currently four FDA- approved devices for clot disruption or removal.
The Mechanical Embolus Removal in Cerebral Ischemia (MERCI) Thrombectomy System is a looped wire with progressively smaller helical loops, advanced via a small catheter through the clot. As the catheter is withdrawn, the coiled wire is deployed, which captures the clot for removal.
The Penumbra Thrombectomy System is designed to aspirate clots from large intracranial vessels. With a suction catheter at the proximal end of the clot, the device continuously debulks and aspirates clot debris until the vessel is clear. The device can remove a clot in a matter of minutes,
whereas fibrinolytics, even those delivered intra-arterially, may take as long as 2 hours to dissolve a thrombus.
The Solitaire Flow Restoration device and the Trevo Retriever device have the unique ability to both immediately bypass the clot and restore flow and retrieve the clot.
Studies have shown that when clot retrieval is performed within eight hours of symptom onset, 60-68% of patients achieved post-procedure revascularization. Patients eligible for clot retrieval are those with recent ischemic stroke, who can receive treatment within at least 12 (preferably 3-6) hours of the onset of stroke. Those patients with uncontrolled HTN, internal bleeding, seizures, blood clotting problems, or those on anticoagulants are not candidates for this procedure.
Complications from clot retrieval procedures include hemorrhage, internal bleeding, death and recurrence of stroke.
Level I Clinical Guideline Recommendations
- Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria (Class I; Level of Evidence A). (New Recommendation):
(a) Prestroke mRS score 0 to 1,
(b) Acute ischemic stroke receiving intravenous r-tPA within 4.5 hours of onset according to guidelines from professional medical societies,
(c) Causative Occlusion of the Internal Carotid Artery or Proximal MCA (M1),
(d) Age ≥18 Years,
(e) NIHSS Score of ≥6,
(f) ASPECTS of ≥6, and
(g) Treatment can be initiated (groin puncture) within 6 hours of symptom onset[3] - Reduced time from symptom onset to reperfusion with endovascular therapies is highly associated with better clinical outcomes. To ensure benefit, reperfusion to TICI Grade 2b/3 should be achieved as early as possible and within 6 hours of Stroke Onset (Class I; Level of Evidence B-R). (Revised from the 2013 Guideline)[3]
Haemorrhagic Stroke[edit | edit source]
In the case of Haemorrhagic Stroke the main aim is to stop the bleeding as early as possible, often requiring Neurosurgical Intervention.
Recent Related Research (from Pubmed)[edit | edit source]
Extension:RSS -- Error: Not a valid URL: Feed goes here!!|charset=UTF-8|short|max=10
References[edit | edit source]
References will automatically be added here, see adding references tutorial.
- ↑ Adams H, Adams R, Del Zoppo G, Goldstein LB. Guidelines for the early management of patients with ischemic stroke: 2005 guidelines update a scientific statement from the Stroke Council of the American Heart Association/American Stroke Association. Stroke. Apr 2005;36(4):916-23.
- ↑ Prasad K, Kaul S, Padma MV, Gorthi SP, Khurana D, Bakshi A. Stroke management. Annals of Indian Academy of Neurology. 2011 Jul 1;14(5):82.
- ↑ 3.0 3.1 3.2 3.3 3.4 Powers WJ, Derdeyn CP, Biller J, Coffey CS, Hoh BL, Jauch EC, Johnston KC, Johnston SC, Khalessi AA, Kidwell CS, Meschia JF. 2015 AHA/ASA focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment. Stroke. 2015 Jan 1:STR-0000000000000074.
- ↑ Verheyen G and Ashbury A. IN Physical Management for Neurological Conditions 3rd Edition. Southampton: Elsevier 2011 pp.12-13

