Principles of Amputation: Difference between revisions
mNo edit summary |
Rucha Gadgil (talk | contribs) No edit summary |
||
| (20 intermediate revisions by 8 users not shown) | |||
| Line 1: | Line 1: | ||
<div class="editorbox"> | <div class="editorbox"> | ||
'''Original Editor '''- [[User:Lucy Coughlan|Lucy Coughlan]] as part of the [[ | '''Original Editor '''- [[User:Lucy Coughlan|Lucy Coughlan]] as part of the [[World Physiotherapy Network for Amputee Rehabilitation Project]] | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
| Line 6: | Line 6: | ||
== Introduction == | == Introduction == | ||
Amputation is the cutting off or the removal of limb/extremity or part thereof | Amputation is the cutting off or the removal of limb/extremity or part thereof,<ref>Limb Loss Definitions. Fact Sheet. Amputee Coalition 2008. http://www.amputee-coalition.org/resources/limb-loss-definitions/ [accessed 24 Sep 2017]</ref> by trauma, prolonged constriction or surgery (see [[Pathology leading to amputation|Pathology leading to amputation]]). As a surgical measure, it is used to control pain or a disease process in the affected limb such as malignancy, [[Infection Prevention and Control|infection]] or gangrene. In some cases, an amputation is carried out on individuals as a preventative surgery for such problems and other people are born with amputations due to congenital disorders (see [[Paediatric limb deficiency]]) | ||
Every care should be taken to assure that the amputation is done only when clinically indicated. Amputation should only be considered if the limb is non-viable (gangrenous or grossly ischemic, dangerous, malignancy or infection), or non-functional<ref name="VA">[http://www.healthquality.va.gov/guidelines/Rehab/amp/amp_sum_correction.pdf Clinical Practice Guideline for Rehabilitation of Lower Limb Amputation]. Department of Veterans Affairs, Department of Defence. 2007</ref>. | Every care should be taken to assure that the amputation is done only when clinically indicated. Amputation should only be considered if the limb is non-viable (gangrenous or grossly ischemic, dangerous, malignancy or infection), or non-functional<ref name="VA">[http://www.healthquality.va.gov/guidelines/Rehab/amp/amp_sum_correction.pdf Clinical Practice Guideline for Rehabilitation of Lower Limb Amputation]. Department of Veterans Affairs, Department of Defence. 2007</ref>. | ||
A well-planned and executed amputation can remove a painful, dysfunctional limb and allow rehabilitation with a prosthetic limb to a functional, painless state. In this regard, amputation surgery may be considered reconstructive surgery, with results similar to amputation of an arthritic femoral head and prosthetic replacement (total-hip replacement)<ref name="Moore">[http://www.oandplibrary.org/alp/chap03-01.asp Thomas J. Moore. Planning for Optimal Function in Amputation Surgery]. Chapter 3 - Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles. 2002</ref>. | A well-planned and executed amputation can remove a painful, dysfunctional limb and allow rehabilitation with a prosthetic limb to a functional, painless state. In this regard, amputation surgery may be considered a reconstructive surgery, with results similar to amputation of an arthritic femoral head and prosthetic replacement ([[Hip Disability and Osteoarthritis Outcome Score|total-hip replacement]])<ref name="Moore">[http://www.oandplibrary.org/alp/chap03-01.asp Thomas J. Moore. Planning for Optimal Function in Amputation Surgery]. Chapter 3 - Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles. 2002</ref>. | ||
== Assessment for | == Assessment for Amputation == | ||
A decision to amputate a limb should be made through discussion with the interdisciplinary team - including the patient - wherever possible; in an emergency situation, the decision should be made based on medical need. There are a number of different investigations that can be carried out to assess the need for | A decision to amputate a limb should be made through discussion with the interdisciplinary team - including the patient - wherever possible; in an emergency situation, the decision should be made based on medical need. There are a number of different investigations that can be carried out to assess the need for amputation; these examinations assess the bones and soft tissues to establish limb viability. | ||
*X-ray – images of bones to view fractures or disease | *X-ray – images of bones to view fractures or disease | ||
| Line 28: | Line 28: | ||
*Fibular artery | *Fibular artery | ||
In '''vascular disease''' these arteries can become blocked or narrowed over time which reduces the circulation to the legs; this can cause pain, ulceration and blackened areas. If left untreated this can lead to gangrene or infection and | In '''vascular disease''' these arteries can become blocked or narrowed over time which reduces the circulation to the legs; this can cause pain, ulceration and blackened areas. If left untreated this can lead to gangrene or infection and amputation is needed to avoid this becoming life-threatening. | ||
[[Image:Gangrene.jpg|frame|center]] | [[Image:Gangrene.jpg|frame|center]] | ||
In '''trauma''' one or more of these blood vessels may be ruptured beyond repair due to the nature of the injuries sustained – e.g. in a car accident, gunshot wound or blast. In this situation an amputation is performed as the limb does not have any blood supply beyond the level of injury and is therefore deemed non-viable. | In '''trauma'''<ref name=":2">Devinuwara K, Dworak-Kula A, O'Connor RJ. Rehabilitation and prosthetics post-amputation. Orthopaedics and Trauma. 2018 Aug 1;32(4):234-40.</ref> one or more of these blood vessels may be ruptured beyond repair due to the nature of the injuries sustained – e.g. in a car accident, gunshot wound or blast. In this situation an amputation is performed as the limb does not have any blood supply beyond the level of injury and is therefore deemed non-viable. | ||
[[Image:Leg-trauma.png|frame|center|300px]] | [[Image:Leg-trauma.png|frame|center|300px]] | ||
| Line 46: | Line 46: | ||
Once a decision has been made to remove part of a limb the level of amputation needs to be decided; this can have significant consequences so there are a number of factors to take into account when planning the surgery: | Once a decision has been made to remove part of a limb the level of amputation needs to be decided; this can have significant consequences so there are a number of factors to take into account when planning the surgery: | ||
* | *The boundary of dead or diseased tissue - if the infection or disease is not completely eradicated the patient may need to undergo further operations or treatment so it is important that the amputation is done at a level where this can be achieved. | ||
*Suitability for prosthesis - if the patient is likely to be a candidate for prosthetic rehab the level of amputation needs to be carefully considered | *Suitability for a prosthesis - if the patient is likely to be a candidate for prosthetic rehab the level of amputation needs to be carefully considered. | ||
*Mobility and function - it is useful to consider the patients’ pre-morbid level of mobility and function | *Mobility and function - it is useful to consider the patients’ pre-morbid level of mobility and function. | ||
*Cosmesis - length and shape of stump affect the aesthetic appearance | *Cosmesis - length and shape of stump affect the aesthetic appearance. | ||
== Amputation Surgery Terminology == | == Amputation Surgery Terminology == | ||
Myodesis: The muscle is secured to the bone by suturing the distal tendon via pre-drilled holes to the bone.<ref name=":0" /> | Myodesis: The muscle is secured to the bone by suturing the distal tendon via pre-drilled holes to the bone.<ref name=":0" /> | ||
* Can be performed on below knee | * Can be performed on below-knee or above-knee amputation. | ||
* This method prevents deformity of the residual limb by preventing excessive shift of the muscle during contraction (when this happens it interferes with the muscle control in the prosthesis)<ref name=":0">Spires MC, Kelly BM, Davis AJ, editors. Prosthetic restoration and rehabilitation of the upper and lower extremity. Demos Medical Publishing; 2013 Dec 19.</ref> | * This method prevents deformity of the residual limb by preventing the excessive shift of the muscle during contraction (when this happens it interferes with the muscle control in the prosthesis).<ref name=":0">Spires MC, Kelly BM, Davis AJ, editors. Prosthetic restoration and rehabilitation of the upper and lower extremity. Demos Medical Publishing; 2013 Dec 19.</ref> | ||
Myoplasty: Attaching sectioned muscles to opposing muscles <ref>Burgess EM, Zettl JH. Amputations below the knee. Artif Limbs. 1969 Jan 1;13(1):1-2. Available at http://www.oandplibrary.org/al/1969_01_001.asp? [Accessed 9 Oct 2017]</ref> | Myoplasty: Attaching sectioned muscles to opposing muscles <ref>Burgess EM, Zettl JH. Amputations below the knee. Artif Limbs. 1969 Jan 1;13(1):1-2. Available at http://www.oandplibrary.org/al/1969_01_001.asp? [Accessed 9 Oct 2017]</ref> | ||
Amputations classifications: | |||
* Minor - toe and partial foot amputations<ref name=":1">Guest F, Marshall C, Stansby G. Amputation and rehabilitation. Surgery (Oxford). 2019 Feb 1;37(2):102-5.</ref> | |||
* Major - when most of the limb is removed<ref name=":1" /> | |||
== Levels of Lower Limb Amputations == | == Levels of Lower Limb Amputations == | ||
=== Amputations of the foot | === Amputations of the foot === | ||
*'''Toe''' - amputation through phalanges or disarticulation of metatarsal-phalangeal joint | *'''Toe''' <ref name=":0" /> - amputation through phalanges or disarticulation of metatarsal-phalangeal joint | ||
**this is the most common lower limb amputation<ref name=":1" /> | |||
**usually due to ulcers | **usually due to ulcers | ||
**great toe amputation affects balance, and ambulation because the late stance phase of gait and push off is disrupted without a first toe/ray to act as the final point of weight transfer | **great toe amputation affects balance, and ambulation because the late stance phase of gait and push off is disrupted without a first toe/ray to act as the final point of weight transfer | ||
**the second toe acts as lateral support to the great toe and amputation of the second toe may lead to halux valgus | **the second toe acts as lateral support to the great toe and amputation of the second toe may lead to halux valgus | ||
**the transverse arch of the foot get affected with the removal of any toe | **the transverse arch of the foot get affected with the removal of any toe<ref name=":0" /> | ||
*'''Ray''' - amputation of toe and the corresponding metatarsal | **usually amputated through the proximal phalanx <ref name=":1" /> | ||
**first ray along with great toe amputations affects balance and gait negatively | **toe amputations should not be performed through the joint because it will expose the avascular cartilage<ref name=":1" /> | ||
*'''Ray''' <ref name=":0" />- amputation of the toe and the corresponding metatarsal | |||
**The first ray along with great toe amputations affects balance and gait negatively | |||
**amputation of the 2nd through 4th ray disrupts the transverse arch because the ligamentous structure is removed | **amputation of the 2nd through 4th ray disrupts the transverse arch because the ligamentous structure is removed | ||
**single ray amputations decrease the "structural integrity of the arch" | **single ray amputations decrease the "structural integrity of the arch" | ||
**when the fifth ray is resected it negatively impacts gait during midstance to terminal stance because it changes the rollover action of the foot | **when the fifth ray is resected it negatively impacts gait during midstance to terminal stance because it changes the rollover action of the foot<ref name=":0" /> | ||
*'''Transmetatarsal''' - partial foot amputation through metatarsals | **when there is infection surgeons can leave the wound open<ref name=":1" /> | ||
**usually due to wounds in the forefoot | *'''Transmetatarsal'''<ref name=":0" /> - partial foot amputation through metatarsals | ||
**usually due to wounds in the forefoot due to gangrene or infection<ref name=":1" /> | |||
**a guillotine amputation is sometimes done in order to rid the foot of infection | **a guillotine amputation is sometimes done in order to rid the foot of infection | ||
**dorsal split thickness grafts on the plantar aspect of the foot | **dorsal split-thickness grafts on the plantar aspect of the foot are used instead of skin grafts because it is more resilient | ||
**the dorsal contact area of the foot is decreased and this leads to an increase of pressure and may result in calluses, ulcers, and wounds | **the dorsal contact area of the foot is decreased and this leads to an increase of pressure and may result in calluses, ulcers, and wounds | ||
**stance and gait (forward propulsion) is negatively influenced because the lever arm of the foot is shortened | **stance and gait (forward propulsion) is negatively influenced because the lever arm of the foot is shortened | ||
**plantar flexion contracture should be avoided - this may occur because of the gastroc-soleus strength dominance over the dorsiflexors | **plantar flexion contracture should be avoided - this may occur because of the gastroc-soleus strength dominance over the dorsiflexors<ref name=":0" /> | ||
**if the wound is well healed, the patient can have excellent function<ref name=":1" /> | |||
<gallery widths="220px" heights="300px"> | <gallery widths="220px" heights="300px"> | ||
File: Amputations-foot-1.png|Ray Amputation | File: Amputations-foot-1.png|Ray Amputation | ||
File: Amputation-foot-2.png|Transmetatarsal | File: Amputation-foot-2.png|Transmetatarsal | ||
File: Amputations-foot-3.png|Great Toe Amputation </gallery> | File: Amputations-foot-3.png|Great Toe Amputation </gallery> | ||
'''MIDFOOT AND HINDFOOT AMPUTATIONS''' [[File:Foot amputation levels .png|350px|thumb|right]] | '''MIDFOOT AND HINDFOOT AMPUTATIONS'''<ref name=":0" /> [[File:Foot amputation levels .png|350px|thumb|right]] | ||
*'''Tarsometatarsal (Lisfranc)''' - amputation of the forefoot at the tarsometatarsal line. | *'''Tarsometatarsal (Lisfranc)''' - amputation of the forefoot at the tarsometatarsal line. | ||
*'''Mid-tarsal (Chopart)''' - amputation between the talus and the calcaneus proximally and the cuboid and the navicular distally. | *'''Mid-tarsal (Chopart)''' - amputation between the talus and the calcaneus proximally and the cuboid and the navicular distally. | ||
| Line 102: | Line 111: | ||
Read more: | Read more: | ||
*[http://www.oandplibrary.org/alp/chap16-01.asp Partial-Foot Amputations: Surgical Procedures] | *[http://www.oandplibrary.org/alp/chap16-01.asp Partial-Foot Amputations: Surgical Procedures] | ||
=== Transtibial / | === Transtibial / Below Knee Amputation (BKA) === | ||
This amputation is done through the tibia and fibula, measurements are taken and flap lines marked out. The surgeon dissects through the skin to then isolate and ligate the nerves and blood vessels. In order to minimise the risk of neuropathic pain (see complications) the nerves are dissected on tension so the end will retract back into the tissues where they can heal away from the stump end. The tibia is dissected using an oscillating saw – optimum length of residual bone is approximately 12-17cm<ref>Wheeless’ Textbook of Orthopaedics: Below Knee Amputation. Available at: http://www.wheelessonline.com/ortho/below_knee_amputation</ref>; the tibia should be beveled at approximately 45° to remove the sharp anterior edge, the fibula should ideally be approx. 1-2 cm shorter than the tibia on a perpendicular axis. Preferred flap technique of surgeon is then used to close the wound and create functional stump - options include skew flap, long posterior flap, sagittal flap or medial flap. | This amputation is done through the tibia and fibula, measurements are taken and flap lines marked out. The surgeon dissects through the skin to then isolate and ligate the nerves and blood vessels. In order to minimise the risk of neuropathic pain (see complications) the nerves are dissected on tension so the end will retract back into the tissues where they can heal away from the stump end. The tibia is dissected using an oscillating saw – optimum length of residual bone is approximately 12-17cm<ref>Wheeless’ Textbook of Orthopaedics: Below Knee Amputation. Available at: http://www.wheelessonline.com/ortho/below_knee_amputation</ref>; the tibia should be beveled at approximately 45° to remove the sharp anterior edge, the fibula should ideally be approx. 1-2 cm shorter than the tibia on a perpendicular axis. Preferred flap technique of surgeon is then used to close the wound and create functional stump - options include skew flap, long posterior flap, sagittal flap or medial flap. | ||
| Line 119: | Line 127: | ||
*Preservation of the knee joint leads to less energy expenditure and better proprioception than an above knee amputee | *Preservation of the knee joint leads to less energy expenditure and better proprioception than an above knee amputee | ||
*Candidates for patella tendon bearing prosthesis | *Candidates for patella tendon bearing prosthesis | ||
*Near normal level of function (more energy expenditure than a non-amputee) | *Near the normal level of function (more energy expenditure than a non-amputee) | ||
*Decreased mortality rate and increases the likelihood for ambulation of the older person when compared to the above knee amputation population | *Decreased mortality rate and increases the likelihood for ambulation of the older person when compared to the above-knee amputation population | ||
'''Disadvantages''' | '''Disadvantages''' | ||
* | *The risk of knee flexion contractures ([[Complications post amputation|see complications]]) | ||
*May need ‘bone bridge’ surgery due to distal fibula pain ([[Complications post amputation|see complications]]) | *May need ‘bone bridge’ surgery due to distal fibula pain ([[Complications post amputation|see complications]]) | ||
| Line 130: | Line 138: | ||
This video shows one example of how a transtibial amputation can be performed.<br> | This video shows one example of how a transtibial amputation can be performed.<br> | ||
{{#ev:youtube| | {{#ev:youtube|gr3K5zJTJC4}} | ||
Read more: | Read more: | ||
| Line 136: | Line 144: | ||
*[http://www.oandplibrary.org/alp/chap18-01.asp Transtibial Amputation: Surgical Procedures and Immediate Postsurgical Management] | *[http://www.oandplibrary.org/alp/chap18-01.asp Transtibial Amputation: Surgical Procedures and Immediate Postsurgical Management] | ||
=== Knee | === Knee Disarticulation Amputation (KDA) / Through Knee Amputation === | ||
Amputation done through the knee joint | Amputation done through the knee joint | ||
| Line 157: | Line 165: | ||
*Bulky prosthesis (see complications) | *Bulky prosthesis (see complications) | ||
*Poor cosmesis as knee mechanism is distal to knee joint (see complications) | *Poor cosmesis as knee mechanism is distal to the knee joint (see complications) | ||
*More demanding surgical procedure with the risk of increased wound complications<ref name=":0" /> | *More demanding surgical procedure with the risk of increased wound complications<ref name=":0" /> | ||
Read more: | Read more: | ||
*[http://www.oandplibrary.org/alp/chap19-01.asp Knee Disarticulation: Surgical Procedures] | *[http://www.oandplibrary.org/alp/chap19-01.asp Knee Disarticulation: Surgical Procedures] | ||
=== Transfemoral (TF)/ | === Transfemoral (TF)/ Above Knee Amputation (AKA) === | ||
This amputation is done through the femur, measurements are taken and flap lines marked out. The surgeon dissects through the skin to then isolate and ligate the nerves and blood vessels. In order to minimise the risk of neuropathic pain (see complications) the nerves are dissected on tension so the end will retract back into the tissues where they can heal away from the stump end. The femur is dissected on its perpendicular axis using an oscillating saw. | This amputation is done through the femur, measurements are taken and flap lines marked out. The surgeon dissects through the skin to then isolate and ligate the nerves and blood vessels. In order to minimise the risk of neuropathic pain (see complications) the nerves are dissected on tension so the end will retract back into the tissues where they can heal away from the stump end. The femur is dissected on its perpendicular axis using an oscillating saw. | ||
The optimum length of residual bone is approximately 7.5-10cm proximal to the superior border of patella. Very short trans-femoral stumps often end up in abduction because there is an imbalance between the adductor and abductor muscles. | The optimum length of the residual bone is approximately 7.5-10cm proximal to the superior border of the patella. Very short trans-femoral stumps often end up in abduction because there is an imbalance between the adductor and abductor muscles. There is a significantly higher level of energy expenditure on the part of an amputee. It varies between 60% and 110% so lower levels of activity and mobility would be expected<ref name=":2" />. | ||
With a transfemoral amputation the distal attachments of the thigh muscles | With a transfemoral amputation, the distal attachments of the thigh muscles are lost, in order to preserve their function and length, a myodesis may be performed to anchor the adductor (and sometimes hamstring) muscles to bone. The hamstrings and quadriceps may then be sutured together over the distal end of the femur – a technique called a myoplasty. It is a myoplasty of the antagonist muscles to help pad the end of the stump to perform Gottchaltk myodesis (adductor magnus trans-osseously fixed and covering the distal femoral end) | ||
<gallery widths="250px" heights="350px"> | <gallery widths="250px" heights="350px"> | ||
| Line 197: | Line 199: | ||
Short stump (c) | Short stump (c) | ||
*weak adductor muscles, causing severe imbalance | *weak adductor muscles, causing a severe imbalance | ||
*the position of the stump often ends up in flexion and abduction | *the position of the stump often ends up in flexion and abduction | ||
*causes massive energy expenditure (effort) and prosthesis can be heavy<br>[[File:TF amputation level3.png|400px|thumb|Very short trans-femoral stumps often end up in abduction because there is an imbalance between the adductor and abductor muscles.|center]] | *causes massive energy expenditure (effort) and the prosthesis can be heavy<br>[[File:TF amputation level3.png|400px|thumb|Very short trans-femoral stumps often end up in abduction because there is an imbalance between the adductor and abductor muscles.|center]] | ||
Read more: | Read more: | ||
*[http://www.oandplibrary.org/alp/chap20-01.asp Transfemoral Amputation: Surgical Procedures] | *[http://www.oandplibrary.org/alp/chap20-01.asp Transfemoral Amputation: Surgical Procedures] | ||
*[ | *[https://www.amputee-coalition.org/resources/transfemoral-amputation-part-2/ The Transfemoral Amputation Level, Part 2, Surgery and Postoperative Care] | ||
=== Other | === Other Types of Amputation in the Lower Limb === | ||
[[File:Hip_and_transpelvis_amputation.jpg|right]] | [[File:Hip_and_transpelvis_amputation.jpg|right]] | ||
==== Hip | ==== Hip Disarticulation ==== | ||
Hip disarticulation is amputation of the whole lower limb through the hip joint. A traditional hip disarticulation is done by separating the ball from the socket of the hip joint, while a modified version retains a small portion of the proximal (upper) femur to improve the contours of the hip disarticulation for sitting. A hip disarticulation results most often from trauma, tumors and severe infections, such as necrotizing fasciitis (commonly referred to as flesh-eating bacteria). Less often, it results from vascular disease and complications of diabetes. <ref name="Smith">Douglas G. Smith. [http://www.amputee-coalition.org/inmotion/jan_feb_05/higherchallenges.html Higher Challenges: The Hip Disarticulation and Transpelvic Amputation Levels]. inMotion, January/February 2005, 15(1).</ref> Many are wheelchair users but can be considered for ischial tuberosity bearing prosthesis. The risks for wound complications and mortality with this type of amputation is very high.<ref name=":0" /> | Hip disarticulation is amputation of the whole lower limb through the hip joint. A traditional hip disarticulation is done by separating the ball from the socket of the hip joint, while a modified version retains a small portion of the proximal (upper) femur to improve the contours of the hip disarticulation for sitting. A hip disarticulation results most often from trauma, tumors and severe infections, such as necrotizing fasciitis (commonly referred to as flesh-eating bacteria). Less often, it results from vascular disease and complications of diabetes. <ref name="Smith">Douglas G. Smith. [http://www.amputee-coalition.org/inmotion/jan_feb_05/higherchallenges.html Higher Challenges: The Hip Disarticulation and Transpelvic Amputation Levels]. inMotion, January/February 2005, 15(1).</ref> Many are wheelchair users but can be considered for ischial tuberosity bearing prosthesis. The risks for wound complications and mortality with this type of amputation is very high.<ref name=":0" /> | ||
==== Hemi-pelvectomy ( | ==== Hemi-pelvectomy (Hindquarter) ==== | ||
Amputation of the whole lower limb and ipsilateral hemi-pelvis<ref>Robert E. Tooms and Frederick L. Hampton. [http://www.oandplibrary.org/alp/chap21-01.asp Hip Disarticulation and Transpelvic Amputation: Surgical Procedures]. Chapter 21A In: Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles.</ref> This type of amputation is most rare. They are likely to be a wheelchair user, some are considered for a trunk and contralateral ischial tuberosity weight bearing prosthesis | Amputation of the whole lower limb and ipsilateral hemi-pelvis<ref>Robert E. Tooms and Frederick L. Hampton. [http://www.oandplibrary.org/alp/chap21-01.asp Hip Disarticulation and Transpelvic Amputation: Surgical Procedures]. Chapter 21A In: Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles.</ref> This type of amputation is most rare. They are likely to be a wheelchair user, some are considered for a trunk and contralateral ischial tuberosity weight-bearing prosthesis | ||
Read more: | Read more: | ||
| Line 239: | Line 239: | ||
*[http://www.oandplibrary.org/alp/chap10-01.asp Scapulo-thoracic dissociation] (forequarter) | *[http://www.oandplibrary.org/alp/chap10-01.asp Scapulo-thoracic dissociation] (forequarter) | ||
There | There is a range of different prosthetics available for the upper limb; these range from hooks to passive orthotics that might mainly serve an aesthetic purpose to fully mechanical and functional limbs.<br> | ||
== Resources == | == Resources == | ||
| Line 251: | Line 251: | ||
[[Category:Amputees]] | [[Category:Amputees]] | ||
[[Category: | [[Category:World Physiotherapy Amputee Project]] | ||
[[Category:Occupational Health]] | [[Category:Occupational Health]] | ||
[[Category:Older People/Geriatrics]] | |||
[[Category:Course Pages]] | |||
Latest revision as of 16:18, 21 July 2023
Original Editor - Lucy Coughlan as part of the World Physiotherapy Network for Amputee Rehabilitation Project
Top Contributors - Admin, Aicha Benyaich, Tarina van der Stockt, Rachael Lowe, Tony Lowe, Kim Jackson, Shaimaa Eldib, Rucha Gadgil, Lauren Lopez, Sheik Abdul Khadir, Amrita Patro, Wanda van Niekerk, Jess Bell and Simisola Ajeyalemi
Introduction[edit | edit source]
Amputation is the cutting off or the removal of limb/extremity or part thereof,[1] by trauma, prolonged constriction or surgery (see Pathology leading to amputation). As a surgical measure, it is used to control pain or a disease process in the affected limb such as malignancy, infection or gangrene. In some cases, an amputation is carried out on individuals as a preventative surgery for such problems and other people are born with amputations due to congenital disorders (see Paediatric limb deficiency)
Every care should be taken to assure that the amputation is done only when clinically indicated. Amputation should only be considered if the limb is non-viable (gangrenous or grossly ischemic, dangerous, malignancy or infection), or non-functional[2].
A well-planned and executed amputation can remove a painful, dysfunctional limb and allow rehabilitation with a prosthetic limb to a functional, painless state. In this regard, amputation surgery may be considered a reconstructive surgery, with results similar to amputation of an arthritic femoral head and prosthetic replacement (total-hip replacement)[3].
Assessment for Amputation[edit | edit source]
A decision to amputate a limb should be made through discussion with the interdisciplinary team - including the patient - wherever possible; in an emergency situation, the decision should be made based on medical need. There are a number of different investigations that can be carried out to assess the need for amputation; these examinations assess the bones and soft tissues to establish limb viability.
- X-ray – images of bones to view fractures or disease
- Computerised Tomography (CT) scan – detailed images of bone, tissue and blood vessels
- Angiogram – outlines blood vessels
- Doppler ultrasound – occlusion of blood vessels
- Venogram and arteriogram – detailed imaging of blood vessels
These investigations will help the surgeons to find out if the blood supply to the limb is intact. The lower limb is supplied by the popliteal artery which subdivides into the:
- Posterior tibial artery
- Anterior tibial artery
- Fibular artery
In vascular disease these arteries can become blocked or narrowed over time which reduces the circulation to the legs; this can cause pain, ulceration and blackened areas. If left untreated this can lead to gangrene or infection and amputation is needed to avoid this becoming life-threatening.

In trauma[4] one or more of these blood vessels may be ruptured beyond repair due to the nature of the injuries sustained – e.g. in a car accident, gunshot wound or blast. In this situation an amputation is performed as the limb does not have any blood supply beyond the level of injury and is therefore deemed non-viable.

There are a number of injury severity scores that may be used in conjunction with clinical investigations to establish the likelihood of limb salvage. Examples of this include:
- Nerve Injury, Ischemia, Soft-Tissue Injury, Skeletal Injury, Shock, and Age of Patient Score (NISSA)[5]
- Limb salvage index (LSI) [6]
- Mangled Extremity Severity Score (MESS)[7]

Once a decision has been made to remove part of a limb the level of amputation needs to be decided; this can have significant consequences so there are a number of factors to take into account when planning the surgery:
- The boundary of dead or diseased tissue - if the infection or disease is not completely eradicated the patient may need to undergo further operations or treatment so it is important that the amputation is done at a level where this can be achieved.
- Suitability for a prosthesis - if the patient is likely to be a candidate for prosthetic rehab the level of amputation needs to be carefully considered.
- Mobility and function - it is useful to consider the patients’ pre-morbid level of mobility and function.
- Cosmesis - length and shape of stump affect the aesthetic appearance.
Amputation Surgery Terminology[edit | edit source]
Myodesis: The muscle is secured to the bone by suturing the distal tendon via pre-drilled holes to the bone.[8]
- Can be performed on below-knee or above-knee amputation.
- This method prevents deformity of the residual limb by preventing the excessive shift of the muscle during contraction (when this happens it interferes with the muscle control in the prosthesis).[8]
Myoplasty: Attaching sectioned muscles to opposing muscles [9]
Amputations classifications:
Levels of Lower Limb Amputations[edit | edit source]
Amputations of the foot[edit | edit source]
- Toe [8] - amputation through phalanges or disarticulation of metatarsal-phalangeal joint
- this is the most common lower limb amputation[10]
- usually due to ulcers
- great toe amputation affects balance, and ambulation because the late stance phase of gait and push off is disrupted without a first toe/ray to act as the final point of weight transfer
- the second toe acts as lateral support to the great toe and amputation of the second toe may lead to halux valgus
- the transverse arch of the foot get affected with the removal of any toe[8]
- usually amputated through the proximal phalanx [10]
- toe amputations should not be performed through the joint because it will expose the avascular cartilage[10]
- Ray [8]- amputation of the toe and the corresponding metatarsal
- The first ray along with great toe amputations affects balance and gait negatively
- amputation of the 2nd through 4th ray disrupts the transverse arch because the ligamentous structure is removed
- single ray amputations decrease the "structural integrity of the arch"
- when the fifth ray is resected it negatively impacts gait during midstance to terminal stance because it changes the rollover action of the foot[8]
- when there is infection surgeons can leave the wound open[10]
- Transmetatarsal[8] - partial foot amputation through metatarsals
- usually due to wounds in the forefoot due to gangrene or infection[10]
- a guillotine amputation is sometimes done in order to rid the foot of infection
- dorsal split-thickness grafts on the plantar aspect of the foot are used instead of skin grafts because it is more resilient
- the dorsal contact area of the foot is decreased and this leads to an increase of pressure and may result in calluses, ulcers, and wounds
- stance and gait (forward propulsion) is negatively influenced because the lever arm of the foot is shortened
- plantar flexion contracture should be avoided - this may occur because of the gastroc-soleus strength dominance over the dorsiflexors[8]
- if the wound is well healed, the patient can have excellent function[10]

Ray Amputation

Transmetatarsal

Great Toe Amputation



MIDFOOT AND HINDFOOT AMPUTATIONS[8]

- Tarsometatarsal (Lisfranc) - amputation of the forefoot at the tarsometatarsal line.
- Mid-tarsal (Chopart) - amputation between the talus and the calcaneus proximally and the cuboid and the navicular distally.
- Ankle disarticulation (Symes) – amputation through the ankle joint
- these 3-type of amputations are mainly performed in children to preserve the length of the residual limb and to keep the epiphyseal plate intact
- equinus varus foot deformity is possible due to the following: a gastrox-soleus and dorsiflexor imbalance, as well as a shortened lever arm
- surgical techniques to prevent this deformity include Achilles Tendon lengthening and the "reattachment of the peroneal and anterior tibial muscles to the more advantageous biomechanical position"
Advantages
- Range of prosthetic options such as insoles, toe fillers or ankle-foot orthosis (exception for ankle disarticulation)
Disadvantages
- May need further surgery in future
- Can lead to skin breakdown and joint pain
- Cosmesis might be not accepted by the patient
Read more:
Transtibial / Below Knee Amputation (BKA)[edit | edit source]
This amputation is done through the tibia and fibula, measurements are taken and flap lines marked out. The surgeon dissects through the skin to then isolate and ligate the nerves and blood vessels. In order to minimise the risk of neuropathic pain (see complications) the nerves are dissected on tension so the end will retract back into the tissues where they can heal away from the stump end. The tibia is dissected using an oscillating saw – optimum length of residual bone is approximately 12-17cm[11]; the tibia should be beveled at approximately 45° to remove the sharp anterior edge, the fibula should ideally be approx. 1-2 cm shorter than the tibia on a perpendicular axis. Preferred flap technique of surgeon is then used to close the wound and create functional stump - options include skew flap, long posterior flap, sagittal flap or medial flap.
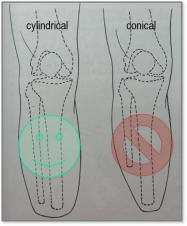
Cylindrical stump (fibula 5-10 mm shorter)
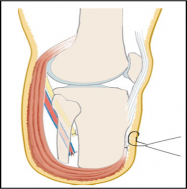
Long posterior muscular flap covering the distal end, attached ventrally to a shorter anterior flap (ventral suture)

Transtibial

Transtibial

.png)


Advantages[8]
- Preservation of the knee joint leads to less energy expenditure and better proprioception than an above knee amputee
- Candidates for patella tendon bearing prosthesis
- Near the normal level of function (more energy expenditure than a non-amputee)
- Decreased mortality rate and increases the likelihood for ambulation of the older person when compared to the above-knee amputation population
Disadvantages
- The risk of knee flexion contractures (see complications)
- May need ‘bone bridge’ surgery due to distal fibula pain (see complications)
This video shows one example of how a transtibial amputation can be performed.
Read more:
Knee Disarticulation Amputation (KDA) / Through Knee Amputation[edit | edit source]
Amputation done through the knee joint



Advantages
- Long lever prevents contractures and allows consequently the movement control[8]
- Maintains muscle length and strength
- Preserves growth plates in children
- Candidates for end bearing prosthesis
- Conserve condyles and the patella
- Proprioception and better distribution of pressure[8]
Disadvantages
- Bulky prosthesis (see complications)
- Poor cosmesis as knee mechanism is distal to the knee joint (see complications)
- More demanding surgical procedure with the risk of increased wound complications[8]
Read more:
Transfemoral (TF)/ Above Knee Amputation (AKA)[edit | edit source]
This amputation is done through the femur, measurements are taken and flap lines marked out. The surgeon dissects through the skin to then isolate and ligate the nerves and blood vessels. In order to minimise the risk of neuropathic pain (see complications) the nerves are dissected on tension so the end will retract back into the tissues where they can heal away from the stump end. The femur is dissected on its perpendicular axis using an oscillating saw.
The optimum length of the residual bone is approximately 7.5-10cm proximal to the superior border of the patella. Very short trans-femoral stumps often end up in abduction because there is an imbalance between the adductor and abductor muscles. There is a significantly higher level of energy expenditure on the part of an amputee. It varies between 60% and 110% so lower levels of activity and mobility would be expected[4].
With a transfemoral amputation, the distal attachments of the thigh muscles are lost, in order to preserve their function and length, a myodesis may be performed to anchor the adductor (and sometimes hamstring) muscles to bone. The hamstrings and quadriceps may then be sutured together over the distal end of the femur – a technique called a myoplasty. It is a myoplasty of the antagonist muscles to help pad the end of the stump to perform Gottchaltk myodesis (adductor magnus trans-osseously fixed and covering the distal femoral end)



Advantages and Disadvantages
For Long stump (a)
- best lever
- better muscular balance while preserving the strength of the adductors
- energy efficient
- candidate for ischial tuberosity bearing prosthesis
Medium-length stump (b)
- reduced strength of the adductors
- increased flexion and abduction
- increased energy expenditure
Short stump (c)
- weak adductor muscles, causing a severe imbalance
- the position of the stump often ends up in flexion and abduction
- causes massive energy expenditure (effort) and the prosthesis can be heavy

Read more:
- Transfemoral Amputation: Surgical Procedures
- The Transfemoral Amputation Level, Part 2, Surgery and Postoperative Care
Other Types of Amputation in the Lower Limb[edit | edit source]

Hip Disarticulation[edit | edit source]
Hip disarticulation is amputation of the whole lower limb through the hip joint. A traditional hip disarticulation is done by separating the ball from the socket of the hip joint, while a modified version retains a small portion of the proximal (upper) femur to improve the contours of the hip disarticulation for sitting. A hip disarticulation results most often from trauma, tumors and severe infections, such as necrotizing fasciitis (commonly referred to as flesh-eating bacteria). Less often, it results from vascular disease and complications of diabetes. [12] Many are wheelchair users but can be considered for ischial tuberosity bearing prosthesis. The risks for wound complications and mortality with this type of amputation is very high.[8]
Hemi-pelvectomy (Hindquarter)[edit | edit source]
Amputation of the whole lower limb and ipsilateral hemi-pelvis[13] This type of amputation is most rare. They are likely to be a wheelchair user, some are considered for a trunk and contralateral ischial tuberosity weight-bearing prosthesis
Read more:
Upper Limb Amputations[edit | edit source]

54% of all upper limb amputations are as a result of trauma; in comparison, only 3% of lower limb amputations are as a result of trauma. Upper limb amputations are seen more rarely than lower limb amputations.
Levels of upper limb amputations:
- Fingers
- Partial hand
- Wrist disarticulation
- Transradial
- Elbow disarticulation
- Transhumeral
- Shoulder disarticulation
- Scapulo-thoracic dissociation (forequarter)
There is a range of different prosthetics available for the upper limb; these range from hooks to passive orthotics that might mainly serve an aesthetic purpose to fully mechanical and functional limbs.
Resources[edit | edit source]
- Definitions of amputation related terms from the Amputee Coalition
- Questions to Ask Your Surgeon
References[edit | edit source]
- ↑ Limb Loss Definitions. Fact Sheet. Amputee Coalition 2008. http://www.amputee-coalition.org/resources/limb-loss-definitions/ [accessed 24 Sep 2017]
- ↑ Clinical Practice Guideline for Rehabilitation of Lower Limb Amputation. Department of Veterans Affairs, Department of Defence. 2007
- ↑ Thomas J. Moore. Planning for Optimal Function in Amputation Surgery. Chapter 3 - Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles. 2002
- ↑ 4.0 4.1 Devinuwara K, Dworak-Kula A, O'Connor RJ. Rehabilitation and prosthetics post-amputation. Orthopaedics and Trauma. 2018 Aug 1;32(4):234-40.
- ↑ McNamara et al (1994) Severe Open Fractures of the Lower Extremity: A Retrospective Evaluation of the Mangled Extremity Severity Score (MESS). J Orthop Trauma 8: 81-7
- ↑ Russell et al (1991) Limb Salvage Versus Traumatic Amputation A Decision Based on a Seven-part Predictive Index Ann Surg. 213: 473-81
- ↑ Johansen et al (1990) Objective Criteria Accurately Predict Amputation following Lower Extremity Trauma. J Trauma.30: 568-73
- ↑ 8.00 8.01 8.02 8.03 8.04 8.05 8.06 8.07 8.08 8.09 8.10 8.11 8.12 8.13 Spires MC, Kelly BM, Davis AJ, editors. Prosthetic restoration and rehabilitation of the upper and lower extremity. Demos Medical Publishing; 2013 Dec 19.
- ↑ Burgess EM, Zettl JH. Amputations below the knee. Artif Limbs. 1969 Jan 1;13(1):1-2. Available at http://www.oandplibrary.org/al/1969_01_001.asp? [Accessed 9 Oct 2017]
- ↑ 10.0 10.1 10.2 10.3 10.4 10.5 10.6 10.7 Guest F, Marshall C, Stansby G. Amputation and rehabilitation. Surgery (Oxford). 2019 Feb 1;37(2):102-5.
- ↑ Wheeless’ Textbook of Orthopaedics: Below Knee Amputation. Available at: http://www.wheelessonline.com/ortho/below_knee_amputation
- ↑ Douglas G. Smith. Higher Challenges: The Hip Disarticulation and Transpelvic Amputation Levels. inMotion, January/February 2005, 15(1).
- ↑ Robert E. Tooms and Frederick L. Hampton. Hip Disarticulation and Transpelvic Amputation: Surgical Procedures. Chapter 21A In: Atlas of Limb Prosthetics: Surgical, Prosthetic, and Rehabilitation Principles.

