Prescribing in Physiotherapy for Pain
Prescribing in Physiotherapy for Pain: A Current and Emerging Role[edit | edit source]
Aim[edit | edit source]
With changing demographics, higher expectations and an increase in long term conditions (Department of Health, 2012) there is an heightened pressure and demand on the NHS. To meet these demands the roles within the NHS have had to change and expand.
As recently as 2013, physiotherapists in England have been granted the right to independently prescribe, giving them the ability to prescribe drugs, including some controlled drugs. These prescriptions must be used “within the overarching framework of human movement, performance and function” (NHS England Publications, 2013)
With these new responsibilities that are becoming a part of a physiotherapist’s remit, this page looks to explore prescribing as a physiotherapist. It also looks to provide information around their scope and responsibilities for prescribing for pain that impacts specialist musculoskeletal physiotherapist’s areas of expertise.
Audience: The resource was produced for use by Band 5 physiotherapists to understand the role the profession plays in prescribing medicines. It may be of benefit to other health professionals seeking knowledge. A case study and questions will be included, which can be used to check understanding after each section
Abbreviations[edit | edit source]

Learning Outcomes[edit | edit source]
LO1. – The learner will able to complete the case study questions to demonstrate an understanding of prescribing within physiotherapy.
LO2. – the learner will be able to distinguish the scope of practice for non-prescribers, supplementary prescribers and independent prescribers within physiotherapy.
LO3. - The learner will be able to comprehend the process of how to become an independent and supplementary prescriber.
LO4. – The learner will be able to describe the effects & side effects of common groups of pain medication, and the role they have to play in patient centred care. Also, they should be able to provide general advice at a band 5 level for pain.
LO5. - The learner will be able to evaluate the effect of prescribing on the current and future role of physiotherapists.
Key Definitions[edit | edit source]
- Pain - The ISAP define pain as “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.” http://www.iasp-pain.org/Taxonomy#Pain
- Extended Scope Practitioner - A clinician who applies and expands their expert knowledge and skills to areas of healthcare traditionally performed by another healthcare profession, which is currently seen as outside the scope of practice of the majority of their profession (Crane and Delany 2013).
- Drug Classes - A drug is put into a class based on the penalty it would have if there was any offence involving the drug.
- Non-prescribers - Physiotherapists without further training within the prescribing field, newly qualified Band 5’s fit within this areas.
- Supplementary prescriber- Those who have had some further training and have an agreed working relationship with a doctor or a dentist to implement treatment plans, any prescriptions that are written by this group must be signed off by the medical practitioner.
- Independent prescribers - Without consultation are able to either from their own diagnosis or a previous diagnosis prescribe treatment including prescribing and are fully responsible and accountable for the treatment. This should be done within the physiotherapists area of expertise.
- Non-Medical Prescriber - Any healthcare professional other than doctors or dentists who can independently prescribe medicine to a patient this includes physiotherapists nurses, podiatrists, pharmacists, chiropodists and optometrists.
Background[edit | edit source]
In 2013 in England and in 2014 for the rest of the UK, physiotherapists were given the right to train to prescribe independently. Below shows a timeline of Key dates:
insert picture here
As the healthcare needs of the British population change, the NHS must also change and adapt to meet them. For example, the British public are living longer and acquiring more long term conditions as a result. These are estimated to occupy 50% of the GP appointments and 70% of hospital beds. Another issue is that there is also thought to be an increase in the expectations of patients who want a co-ordinated, accessible 7-day service from the NHS. It has also been felt in literature that patients may find their healthcare experience disjointed and repetitive, due to a lack of integration between healthcare professionals (Morris 2002). Each of these puts extra pressure on a resource strapped service, with costs currently thought to be around £12.3 billion per year (Donaldson, 2008). To meet these challenges new approaches and changing roles are being implemented (NHS England 2013) .
Due to this setting of increasing demand and reducing resources, a supported decision was made to grant physiotherapists prescribing powers. Some of the many highlighted benefits of this for the patient include;
- Making a patient’s prescribing experience an easier, quicker and more streamlined pathway within a single appointment, reducing a patient’s total number of appointments within the NHS (NHS England Publications, 2013)
- Increasing involvement and independent management of a patient’s entire healthcare journey, as a result of the increasing use of physiotherapists as first-contact practitioners (Chartered Society of Physiotherapy 2013)
- Reducing demand on finite medical resources by preventing delays and contributing to a flexible team (DHSSPS, 2013)
- Utilising the skills of the non-medical professions expertise in their specialist area to provide patient centred care.
This was summed up by Phil Gray, chief executive of the Chartered Society of Physiotherapy, upon physiotherapists being awarded the right to independently prescribe said that:
"This is a landmark moment that will lead to patients receiving faster, more effective treatment for their condition” (BBC 2013).
Of the 94 physiotherapists who have taken this professional leap forward, six interviewed by the magazine Frontline indicated that they felt the greatest benefit of their prescribing power was the ability to streamline patient care. They felt that it allowed them to begin treating patients immediately, without having to send them back to their GP for sufficient pain relief, and allowed them to view the bigger picture of a patient’s care (Hunt 2015).
Whilst this resource looks to educate on the drugs used by physiotherapists for pain, physiotherapists are also using the independent prescribing power to help prescribe for other conditions such as spasticity management (Ashford et al 2014)
Scope of Practise[edit | edit source]
Prescribing may appear a strange addition to a physiotherapist’s toolkit and outside the remit of the profession, which are defined by the Chartered Society of Physiotherapy (2013) as anything within the 4 pillars of practice. These are:
- Massage
- Exercise and movement
- Electrotherapy
- Kindred methods of treatment
Any physiotherapist must not only work within their own personal scope of practice, but also within the scope of the profession (Chartered Society of Physiotherapy 2013).
? Do you think prescribing is within the scope of physiotherapy?
In a narrative review, Crane and Delany (2013) comment that physiotherapists demonstrate an excellent ability to clinically reason and adapt to the changing needs of the societies they serve. The UK government has been convinced that prescribing is within physiotherapy’s scope because physiotherapists already possess the core skills that it requires.
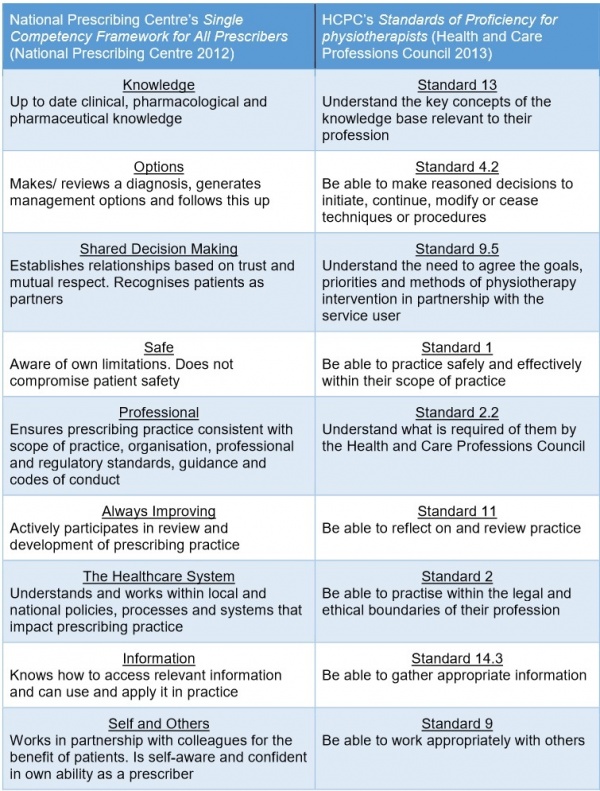
The National Prescribing Centre has produced a framework that applies to all prescribers, no matter what profession they come from. Below is a comparison of this framework it to the HCPC’s Standards of Proficiency for physiotherapists:
 Personal Scope of Practice[edit | edit source]
Personal Scope of Practice[edit | edit source]

Although prescribing is within the scope of the profession, like any skill, it only becomes part of an individual physiotherapist’s scope of practice when they become competent through training (Chartered Society of Physiotherapy 2013). This means that before prescribing is suitable addition to a physiotherapist’s skill set, they must already be an expert in the field they wish to apply it (National Prescribing Centre 2012). As a consequence, although the scope of prescribing within in physiotherapy is very wide, it is limited to only an individual's clinical specialty (Chartered Society of Physiotherapy 2013). This is a major difference from medical prescribing who may prescribe for any condition.
! It is important to remember that prescribing physiotherapists are not the equivalent of doctors, and their practice is restricted to their own patients, who they have performed a comprehensive assessment on (Chartered Society of Physiotherapy 2013).
? You may reach a point in your career where begin to feel that you have gained enough knowledge, training and experience that prescribing is becoming within your scope of practice. Would you be able to ‘tick all these boxes’? Only then is prescribing completely within your scope (Health and Care Professions Council 2013):
Insert boxes here
Once a physiotherapist decides that prescribing would be of benefit and for their practice there are two types of prescriber they can become, based on their level of training.
Supplementary Prescribers[edit | edit source]
Supplementary prescribers can prescribe any medication, but it must be detailed in a written CMP. The CMP is created in partnership with the patient and a medical prescriber (Chartered Society of Physiotherapy 2013). This means that although they are accountable for their decision to prescribe, they share accountability with the medical prescriber for the decision to put the medication in the CMP (Chartered Society of Physiotherapy 2013). In their nursing supplementary prescriber counterparts, this leads many doctors to feel that they have the ultimate responsibility for both supplementary prescriber and patient. This can result in supplementary prescribers feeling subordinate, rather than in partnership with their medical prescriber (Creedon et al. 2015).
Supplementary prescribing is particularly suited to the care of chronic conditions, as once a CMP is in place, medical prescriber can pass over management of a patient to the supplementary prescriber. Supplementary prescribers have expert knowledge of medications within their specialty, and can therefore modify or prescribe any drug detailed within the CMP, but have no influence on drugs that patients receive for other co-morbidities. (Chartered Society of Physiotherapy 2013). As experts in prescribing they may also provide detailed advice on any aspect of a medication for a patient, so long as they are used in their area of clinical specialty (Chartered Society of Physiotherapy 2013).
Independent Prescribers[edit | edit source]
Independent prescribers share many features and core skills with supplementary prescribers (National Prescribing Centre 2012). However, as they prescribe completely autonomously and not in partnership with medical prescribers, they are wholly responsible for every aspect of the prescribing process (Chartered Society of Physiotherapy 2013). They can actually prescribe fewer medicines than a supplementary prescriber, but are fully autonomous when doing so. As a result, Creedon et al. (2015) feel that they represent a greater challenge to medical authority.
? Do you think you would rather become a supplementary or independent prescriber? What would be a more useful adjunct to your practice?
How does a physiotherapist decide what is within their scope? In a qualitative study by Dawson and Ghazi (2004) of physiotherapists working in similar roles, as extended scope practitioners in orthopaedic clinics, many participants commented that they felt many of the skills required were beyond the current scope of physiotherapy. However, all felt confident in their jobs despite this, as they were aware of their limitations and able to liaise with their medical colleagues when in need of advice. This really highlights the key question any responsible physiotherapy prescriber should ask themselves when deciding what is within their scope. Simply put, it is ‘do I feel confident practicing this, with my current level of knowledge and skill set?’ This directly relates to some of the key competencies of a good prescriber, detailed by the Single Competency Framework For All Prescribers (National Prescribing Centre 2012), where prescribers, irrespective of who they are, should be self-aware, aware of their limitations, and confident in their ability.
Non-Prescribers
The vast majority of physiotherapists globally are not prescribers and there appears to be debate regarding what their level of involvement in prescribing should be. In Australia, like in the UK, this is felt to be a legislative ‘grey’ area; different physiotherapist have different opinions on the extent of their scope regarding medicines (Morris and Grimmer 2014). This is reflected in the guidance provided by professional bodies, as they feel an individual’s scope should vary depending on the depth of knowledge that they can demonstrate (Chartered Society of Physiotherapy 2013).
Studies investigating this have found that physiotherapists are frequently asked a wide variety of questions regarding NSAIDs and often feel pressured by patients to provide advice and recommendations regarding them. Almost all felt concerned that they lacked sufficient knowledge to confidently provide this, commensurate with their duty of care to their patients (Kumar and Grimmer 2005).
Kumar and Grimmer (2005) also found that most of the physiotherapists were not aware of the up to date research that has influenced best practice for NSAIDs. It would therefore be argued that this was not within the scope of these physiotherapists. It is expected in the UK that all newly qualified Band 5 physiotherapists should be sufficiently competent to advise patients on where to find appropriate advice regarding their medications, and give appropriate advice of medications that might be suitable for a patient. If they can demonstrate their competence, they can give general information on a medicine, such as widely known side-effects of a commonly accessible medicine like ibuprofen (Chartered Society of Physiotherapy 2013). However, they are keen to stress there is a difference between giving advice and prescribing, and therefore non-prescribing physiotherapists can not suggest alterations to a patient’s prescribed medications.
Importantly, if you notice a patient is taking a medication wrongly, you can show them the directions that have been prescribed. If you feel a medicine would be of benefit to a patient, you can suggest they speak to their doctor regarding it; and if you are concerned of the effects of a medication you may ask them to speak to their doctor, or directly contact them (Chartered Society of Physiotherapy 2013).

