Pain-Modulation: Difference between revisions
No edit summary |
No edit summary |
||
| Line 15: | Line 15: | ||
===== Level 1: Periphery ===== | ===== Level 1: Periphery ===== | ||
Level 1 pain modulation refers to events acting in the periphery of the body, at the source of the pain source. The [[somatosensation]] defined as the sensation from skin, mucus, limbs, and joints and classified into: thermoception, [[nociception]], equilibrioception mechanoreception response to (vibration, touch, and pressure), and [[Proprioception|proprioception.]] | Level 1 [[Pain Behaviours|pain]] modulation refers to events acting in the periphery of the body, at the source of the pain source. The [[somatosensation]] defined as the sensation from skin, mucus, limbs, and [[Joint Classification|joints]] and classified into: thermoception, [[nociception]], equilibrioception mechanoreception response to (vibration, touch, and pressure), and [[Proprioception|proprioception.]] | ||
Nociceptors are peripheral cell nerve endings that initiate pain sensation, respond to noxious stimulus (thermal, mechanical, or chemical) which in turn trigger action potential to the spinal cord and to higher centers. It is divided into A delta and C fibers. | [[Nociception|Nociceptors]] are peripheral cell nerve endings that initiate pain sensation, respond to noxious stimulus (thermal, mechanical, or chemical) which in turn trigger action potential to the [[Spinal cord anatomy|spinal cord]] and to higher centers. It is divided into A delta and C fibers. | ||
* A- delta fibers are large(larger than C- fiber) myelinated, fast conducting fibers, concerned with localized, sharp, and fast sensation of pain. | * A- delta fibers are large(larger than C- fiber) myelinated, fast conducting fibers, concerned with localized, sharp, and fast sensation of pain. | ||
| Line 40: | Line 40: | ||
The modulation at the level of spinal cord produce localized analgesic effect and it receive another control from the descending pathway to cause diffuse inhibition of pain. | The modulation at the level of spinal cord produce localized analgesic effect and it receive another control from the descending pathway to cause diffuse inhibition of pain. | ||
===== Level 3: Fast Neuronal Descending Pathways | ===== Level 3: Fast Neuronal Descending Pathways and Endogenous ===== | ||
The [[Descending Pathways|descending inhibitory pathway]]/ pain modulation mechanism depend on the release of [[opioids]] at the SG it controls/ inhibits signals transmission between the the 1<sup>st</sup> and 2<sup>nd</sup> order neuron. The descending pathway start from periaqueductal gray matter PAG in the [[Brainstem|midbrain]], then to raphe nucleus in the medulla to the dorsal horn of spinal cord where: | The [[Descending Pathways|descending inhibitory pathway]]/ pain modulation mechanism depend on the release of [[opioids]] at the SG it controls/ inhibits signals transmission between the the 1<sup>st</sup> and 2<sup>nd</sup> order neuron. The descending pathway start from periaqueductal gray matter PAG in the [[Brainstem|midbrain]], then to raphe nucleus in the medulla to the dorsal horn of spinal cord where: | ||
These pathways release serotonin and noradrenergic neuron to inhibit the release of substance P from the presynaptic cleft of the first order neuron. | These pathways release serotonin and noradrenergic neuron to inhibit the release of substance P from the presynaptic cleft of the first order neuron. | ||
Stimulate the inhibitory interneuron to release opioids which in turn inhibit the presynaptic form releasing substance P and inhibit the post synapse of the second order neuron from transmitting signals. | Stimulate the inhibitory interneuron to release opioids (endorphin, enkephalin) which in turn inhibit the presynaptic form releasing substance P and inhibit the post synapse of the second order neuron from transmitting signals. | ||
{{#ev:youtube|5c8maFAhqIc|300}}<ref>Armando Hasudungan. PAIN! Physiology - The Ascending Pathway, Descending Pain Pathway and the Substantia Gelatinosa. Available from: http://www.youtube.com/watch?v=5c8maFAhqIc[last accessed 11/12/2021]</ref> | {{#ev:youtube|5c8maFAhqIc|300}}<ref>Armando Hasudungan. PAIN! Physiology - The Ascending Pathway, Descending Pain Pathway and the Substantia Gelatinosa. Available from: http://www.youtube.com/watch?v=5c8maFAhqIc[last accessed 11/12/2021]</ref> | ||
===== Level 5: Cortical ===== | |||
===== Level 5: Cortical | |||
[[File:Anterior cingulate gyrus animation.gif|thumb|Anterior cingulate cortex.]] | [[File:Anterior cingulate gyrus animation.gif|thumb|Anterior cingulate cortex.]] | ||
The noxious stimulus transmit to the cortex via [[spinothalamic tract]] that relay as a 3<sup>rd</sup> interneuron in the [[Cerebral Cortex|somatosensory area]]. Pain signals at the cortex induce pain modulation by two mechanisms: | The noxious stimulus transmit to the cortex via [[spinothalamic tract]] that relay as a 3<sup>rd</sup> interneuron in the [[Cerebral Cortex|somatosensory area]]. Pain signals at the cortex induce pain modulation by two mechanisms: | ||
Revision as of 21:48, 12 December 2021
This article or area is currently under construction and may only be partially complete. Please come back soon to see the finished work!
Pain Modulation[edit | edit source]
Pain modulation the process of alterations in the pain signals along the transmission pathway of pain, it explains why individuals response to the same stimulus different, explains the mechanism of action when using clinical analgesic. Pain control and modulation is a complex chore that is often the primary reason patients seek the services of rehabilitation professionals. Modulation of pain begins with an understanding of the various levels of pain modulation and extends to clinical interventions and protocols designed to reduce pain. For example, opiates they are capable of increasing and decreasing pain experience.
Levels of Pain Modulation[edit | edit source]
Pain modulation is easily classified into 5 discreet levels of interaction. These levels correspond to either important synaptic junctions, or significant chemical processes involved in the transmission of pain.
Level 1: Periphery[edit | edit source]
Level 1 pain modulation refers to events acting in the periphery of the body, at the source of the pain source. The somatosensation defined as the sensation from skin, mucus, limbs, and joints and classified into: thermoception, nociception, equilibrioception mechanoreception response to (vibration, touch, and pressure), and proprioception.
Nociceptors are peripheral cell nerve endings that initiate pain sensation, respond to noxious stimulus (thermal, mechanical, or chemical) which in turn trigger action potential to the spinal cord and to higher centers. It is divided into A delta and C fibers.
- A- delta fibers are large(larger than C- fiber) myelinated, fast conducting fibers, concerned with localized, sharp, and fast sensation of pain.
- C- fibers are small, unmyelinated, slow conducting nerve fibers, concerned with dull, and slow pain sensation.
Under normal conditions the nociceptors are inactive when there is a noxious stimulus (tissue damage) those pain receptors respond according to the stimulus type and cyclooxygenase-2 is activated to release more PG(prostaglandin) at the site of injury, and the nociceptors will transmit signals to the dorsal horn of spinal cord (first order neuron) where the firs neuron release chemical substance P to transmit signals..
A- beta are myelinated, large diameter, and have the fastest conduction velocity. These fibers respond to non painful stimulus such as touch sensation, mild pressure, and vibration. A beta stimulated by deep touch that explain why rubbing the painful site relief your pain[1][2].
Level 2: Dorsal Horn[edit | edit source]
Level 2 pain modulation refers to events in the dorsal horn of the spinal cord. The modulation at the level of spinal cord take place at Substantial Gelatenosa of Ronaldo SG under the theory of gait control theory GCT, it was proposed for first time in 1965 by Ronald Melzack and Patrick Wall, this theory explain pain transmission and modulation depending on large(A-Beta) and small (C-fibers) sensory fibers. At homeostasis conditions the gait is closed and no pain signals are transmitted (the inhibitory interneuron I block the projection neuron which transmit pain signals and connect to the brain).
When small nociceptors fibers are stimulated by noxious stimulus action potential signals are transmitted which in turn inhibit the inhibitory interneuron (I) and the projection neuron is activated the gate is opened and pain signal are transmitted to the brain. When action potential transmits through the first order neuron that in turn activate the vesicles to release the substance P which propagate the transmission of pain signals.
If large sensory fibers(A-Beta) activated by deep touch for example the transmitted signals activate the inhibitory interneuron and which blocks the projection neuron, the gate is close and no pain[3]. Interruption of pain signals at dorsal horn affect on spinothalamic tract to the cortex.
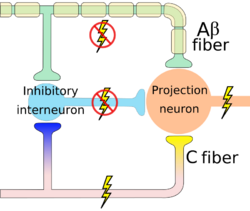
gate opened
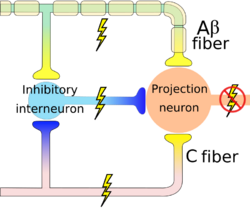
gate closed


The modulation at the level of spinal cord produce localized analgesic effect and it receive another control from the descending pathway to cause diffuse inhibition of pain.
Level 3: Fast Neuronal Descending Pathways and Endogenous[edit | edit source]
The descending inhibitory pathway/ pain modulation mechanism depend on the release of opioids at the SG it controls/ inhibits signals transmission between the the 1st and 2nd order neuron. The descending pathway start from periaqueductal gray matter PAG in the midbrain, then to raphe nucleus in the medulla to the dorsal horn of spinal cord where:
These pathways release serotonin and noradrenergic neuron to inhibit the release of substance P from the presynaptic cleft of the first order neuron.
Stimulate the inhibitory interneuron to release opioids (endorphin, enkephalin) which in turn inhibit the presynaptic form releasing substance P and inhibit the post synapse of the second order neuron from transmitting signals.
Level 5: Cortical[edit | edit source]

The noxious stimulus transmit to the cortex via spinothalamic tract that relay as a 3rd interneuron in the somatosensory area. Pain signals at the cortex induce pain modulation by two mechanisms:
- The cortex activate the PAG in the midbrain to activate the descending pathway (top down control of pain ) that interrupt and inhibit pain signals at the dorsal horn as mentioned before, so by extension the spinothalamic tract is inhibited[5].
- The interaction between different areas; cerebral cortex, limbic forebrain structures, basal ganglia, importance of this interaction is to perceive the noxious but as a non painful. For example activation of Anterior cingulate cortex (ACC) and the Rostral agranular insular cortex (RAIC) by noxious stimulus showed activation of these area and increase in the regional cerebral blood flow (rCBF) to these area. ACC plays a role in pain transmission and believed to be related to placebo analgesia and has a role with conditioned learning[6][7].

Rostral agranular insular cortex also affect on the descending inhibitory pathway and is responsible for pain learning and memory. There is a study suggest that paraventricular hypothalamic nucleus send projections of oxytocinergic that support GABA neurotransmission and activate descending spinal noradrenergic mechanisms[8].
Pain Interventions[edit | edit source]
Modalities[edit | edit source]
Transcutaneous Electrical Nerve Stimulation (TENS).
Acupuncture, Acupressure.
Exercise[edit | edit source]
Manual Therapy[edit | edit source]
Myofascial release and Message.
Joint mobilization.
Resources[edit | edit source]
UTHealth, the university of Texas
References[edit | edit source]
- ↑ Purves D, Augustine GJ, Fitzpatrick D, Katz LC, LaMantia AS, McNamara JO, Williams SM. Nociceptors. Sunderland, MA. 2001.
- ↑ Yam MF, Loh YC, Tan CS, Khadijah Adam S, Abdul Manan N, Basir R. General pathways of pain sensation and the major neurotransmitters involved in pain regulation. International journal of molecular sciences. 2018 Aug;19(8):2164.
- ↑ Yam MF, Loh YC, Tan CS, Khadijah Adam S, Abdul Manan N, Basir R. General pathways of pain sensation and the major neurotransmitters involved in pain regulation. International journal of molecular sciences. 2018 Aug;19(8):2164.
- ↑ Armando Hasudungan. PAIN! Physiology - The Ascending Pathway, Descending Pain Pathway and the Substantia Gelatinosa. Available from: http://www.youtube.com/watch?v=5c8maFAhqIc[last accessed 11/12/2021]
- ↑ Ohara PT, Vit JP, Jasmin L. Cortical modulation of pain. Cellular and Molecular Life Sciences CMLS. 2005 Jan;62(1):44-52.
- ↑ Xie YF, Huo FQ, Tang JS. Cerebral cortex modulation of pain. Acta Pharmacologica Sinica. 2009 Jan;30(1):31-41.
- ↑ Steeds CE. The anatomy and physiology of pain. Surgery (Oxford). 2009 Dec 1;27(12):507-11.
- ↑ Gamal-Eltrabily M, de Los Monteros-Zúñiga AE, Manzano-García A, Martínez-Lorenzana G, Condés-Lara M, González-Hernández A. The rostral agranular insular cortex, a new site of oxytocin to induce antinociception. Journal of Neuroscience. 2020 Jul 15;40(29):5669-80.

