Obesity: Difference between revisions
(replace wrong ampersand with single one) |
m (Changed protection settings for "Obesity": Course Page ([Edit=⧼protect-level-ppadmin⧽] (indefinite) [Move=⧼protect-level-ppadmin⧽] (indefinite))) |
||
| (30 intermediate revisions by 10 users not shown) | |||
| Line 4: | Line 4: | ||
'''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
</div> | </div> | ||
== | == Introduction == | ||
[[File:Waist big.jpeg|right|frameless]] | |||
Obesity is the excessive accumulation of [[Adipose Tissue|adipose tissue]] in the body, that may impair health, due to consuming more food than is required for energy<ref name="Maguire">Maguire, T & Haslam, D (2010) The Obesity Epidemic and Its Management [Online] London. Pharmaceutical Press. Available from http://lib.myilibrary.com/Open.aspx?id=239868&src=0 [Accessed 6/3/2012]</ref><ref name="Haslam">Haslam, D, Sattar, N & Lean, M (2007) Obesity- time to wake up. In: Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.</ref>. | |||
* According to the WHO in 2016 1.9 billion people were overweight, 600 million of these were obese and alarmingly 41 million children under the age of 5 were overweight or obese.<ref name=":0" /> | |||
* By 2030 some epidemiologists suggest that 20% of the world's population will be obese, i.e., having a body mass index ([[Body Mass Index|BMI]]) of more than 30 kg/m² in adults, or a BMI ≥95th percentile for age and sex in children aged 2 to 18 years<ref>Tirthani E, Said MS, Rehman A. [https://www.statpearls.com/ArticleLibrary/viewarticle/131519 Genetics and Obesity.] StatPearls [Internet]. 2021 Aug 4.Available:https://https://www.statpearls.com/ArticleLibrary/viewarticle/131519 (accessed 13.11.2021)</ref>. it is also vital to check [[Waist Measurement|waist measurement]] and [[Body Composition|body composition]]. Obesity correlates with increasing an individual’s risk of cancers, [[stroke]], [[Metabolic Syndrome|metabolic disease]], [[Heart Failure|heart failure,]] and other [[Cardiovascular Disease|cardiovascular]] conditions, | |||
* As research into obesity continues new definitions emerge, one being normal weight obesity. This refers to individuals with normal body weight by body mass index (BMI) but a high body [[Adipose Tissue|fat]] percentage. This group of people are at a notably increased risk of developing metabolic syndrome, cardiometabolic dysfunction and increased mortality<ref>Mohammadian Khonsari N, Baygi F, Tabatabaei-Malazy O, Mohammadpoor Nami S, Ehsani A, Asadi S, Qorbani M. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10010388/ Association of normal weight obesity phenotype with inflammatory markers: A systematic review and meta-analysis]. Frontiers in Immunology. 2023 Feb 27;14:1044178.Available:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10010388/ (accessed 29.9.2023)</ref>. | |||
[[ | == Etiology == | ||
Obesity is the result of an imbalance between daily energy intake and energy expenditure resulting in excessive weight gain. Obesity is caused by multiple factors which can be [[File:Junk food.jpg|right|frameless|300x300px]] | |||
* genetic | |||
* cultural | |||
* societal | |||
*reduced physical activity | |||
* insomnia | |||
* food habits | |||
* [[Metabolic and Endocrine Disorders|endocrine]] disorders | |||
* medications, | |||
* food advertisements | |||
* energy metabolism<ref name=":1">Kiran K. Panuganti; Ravi K. Kshirsagar. | |||
☀October 28, 2019 [https://www.ncbi.nlm.nih.gov/books/NBK459357/ Obesity] . Available from:https://www.ncbi.nlm.nih.gov/books/NBK459357/ (last accessed 15.2.2020) | |||
</ref>. | |||
< | == Epidemiology == | ||
[[File:Obese Child.jpg|right|frameless]]According to the WHO in 2016 1.9 billion people were overweight, 600 million of these were obese and alarmingly 41 million children under the age of 5 were overweight or obese<ref name=":0">World Health Organisation. Obesity and overweight factsheet. http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight [Accessed 3 Dec 2018] | |||
</ref>. | |||
* Nearly one-third of adults and about 17% of adolescents in the United States are obese. | |||
* Recent statistics show that nearly a quarter of the UK adult population are obese and obesity is rising quickly, every year obesity in the UK costs the economy £3.5bn<ref name="Haslam" />. | |||
* According to Center for Disease Control and Prevention (CDC), 2011 to 2012 data, one out of five adolescents, one out of six elementary school age children, and one out of 12 preschool age children are obese.<ref name=":1" /> | |||
* Obesity is more prevalent in African Americans, followed by Hispanics and whites. Southern US states have the highest prevalence, followed by the Midwest, Northeast and the west. | |||
* Obesity is a global problem with rates even higher than what are seen in North America.<ref name=":1" /> | |||
Deemed Obese in England, figures (see the need for concern!) | |||
* 1980, 6% of men and 8% of women | |||
* 1995 15% of men and 16.5% of women were classed as obese<ref name="Anderson">Anderson, P & Butcher, K (2006) Childhood Obesity: Trends and Potential Causes, The Future of Children, 16 (1) Princeton University and The Brookings Institution.</ref>'''.''' | |||
* 2010, 23.6% of men and 23.8% of women in England were obese. Obesity levels in Scotland were slightly higher in women with 26% being obese<ref name="Haslam" />. | |||
Obesity is a significant risk for developing [[Diabetes Mellitus Type 2|Type 2 Diabetes]], with 90% of diabetes diagnosis being type 2. There are over 422 million people worldwide living with diabetes<ref>World Health Organisation. World Health Day 2016: Beat diabetes http://www.who.int/campaigns/world-health-day/2016/en/ [Accessed 3 Dec 2018] | |||
</ref> and in 2012 1.5 million people died as a direct result of this disease. | |||
== How Physiotherapists Can help == | |||
< | Physiotherapists, as [[Exercise Physiology|exercise]] experts, join the worldwide concern for the ever-growing epidemic of obesity, which affects adults and children alike<ref name="Crawley">Crawley, J (2006) Markets and Childhood Obesity Policy, The Future of Children, 16 (1) Princeton University and The Brookings Institution.</ref>. It is probably one of the greatest challenges to our health systems around the world in the 21st century. | ||
< | There are two important interventions to prevent and manage obesity. | ||
* Optimal [[Nutrition|nutrition]]. | |||
* Increased exercise and [[Physical Activity|physical activity]]. The potential contribution of physical therapists to the latter approach is immense.<ref>Dr Marilyn Moffat, President of the WCPT. [http://www.wcpt.org/sites/wcpt.org/files/files/ads/WPTDay2011-B4-President_Quotes.pdf How physical therapists fight non-communicable fckLRdisease throughout the lifespan]. 2011</ref> | |||
Physiotherapists can introduce the idea of utilizing exercise as a means of reducing obesity (i.e., reducing fat mass) and associated benefits. | |||
* Fitness is associated with more desirable clinical outcomes in many instances, such as decreasing metabolic disease, cardiovascular disease, Alzheimer disease risk, inflammation, and many other disease. | |||
* If the patient is able to exercise, exercise may be the preferred route to decrease disease symptoms and/or future risk compared to alternative pharmaceuticals that may exacerbate symptoms. | |||
* An open and communicative relationship between the physiotherapist and the patient must be present in order to suggest the addition of exercise to the patient's lifestyle in order to decrease obesity and improve negative side effects. | |||
< | ===Exercise and Physical Activity=== | ||
Physical activity is any movement of the body that requires the use of our skeletal muscles, which in turn requires energy expenditure. This energy expenditure is basic to weight control. | |||
* Aerobic exercise prescriptions and recommendations for strength/resistance training must go hand in hand with reduced food intake, and the progression of activity should be gradual, scientifically based, and tailored individually to each person. | |||
* It is important that the physiotherapist finds the most appropriate activity for the individual, so that they will not only enjoy the activity but also have a greater chance of staying with it. | |||
* There are numerous types of exercise prescriptions that the physiotherapist may use in their increasing effort to battle the obesity epidemic. | |||
The sooner all our nations begin to adopt initiatives and programmes to combat obesity and other diseases of civilisation, the less will be the burdens on health systems delivery around the world. | |||
* Obesity is reaching epidemic proportions and the topic of obesity is a core part in medical curricula<ref name="Lean 2007">Lean, M, & Lara, J & O Hill, J (2007) Strategies for preventing obesity. In: Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.</ref>. | |||
* Every time a health professional has the opportunity to see a patient, they should be able to assess the patient to see if they have a weight problem and either refer them to a specialist or offer simple advice<ref name="Lean 2007" />. | |||
* Physiotherapists have a key role to play in trying to reverse this trend as they often use exercise as a form of treatment, so if a patient is too overweight to do exercise, it becomes harder for the treatment to be successful<ref name="Bird">Bird, S (1992) Exercise Physiology For Health Professionals. London. Chapman & Hall.</ref>. | |||
A cross-sectional study performed in 115 children in Japan assessing the factors associated with excess weight in children suggest that decreasing children's sedentary behavior in addition to more physical activity is essential for the prevention of overweight status and obesity in high-risk children with lifestyle diseases<ref>NAKANO S, HIRANO C, HOTTA K, FUJITA Y, YANAGI H. [https://pubmed.ncbi.nlm.nih.gov/32015943-factors-associated-with-overweight-status-obesity-and-sedentary-behavior-in-elementary-and-junior-high-school-students/ Factors associated with overweight status, obesity, and sedentary behavior in elementary and junior high school students.] Physical Therapy Research. 2019 Dec 20;22(2):66-72.</ref>. Study results suggest that aerobic exercise is more relevant than resisted exercise training in modulating inflammatory cytokines and quality of life among obese post-menopausal women<ref>Abd El-Kader SM, Al-Jiffri OH. [https://pubmed.ncbi.nlm.nih.gov/32127864/ Impact of aerobic versus resisted exercise training on systemic inflammation biomarkers and quality of Life among obese post-menopausal women.] African Health Sciences. 2019;19(4):2881-91.</ref>. | |||
< | A pilot trial found that ferritin in postmenopausal women participating in Resisted Training (RT) over 15 weeks positively correlated with ferritin, total cholesterol, low-density lipoprotein, and non-high-density lipoprotein cholesterol while negatively correlated with HDL. However, a large-scale cohort is needed to confirm these findings<ref>Ward LJ, Hammar M, Lindh-Åstrand L, Berin E, Lindblom H, Rubér M, Holm AC, Li W. [https://pubmed.ncbi.nlm.nih.gov/32123242/ Does resistance training have an effect on levels of ferritin and atherogenic lipids in postmenopausal women?–A pilot trial.] Scientific reports. 2020 Mar 2;10(1):1-8.</ref>. | ||
===Patient Education=== | |||
[[File:Obesity & BMI.png|right|frameless]] | |||
One of the main roles of a physiotherapist regarding obesity is educating patients. | |||
< | Many people are falsely led to believe that they can lose weight without putting in effort or changing from a sedentary lifestyle<ref name="Bird" />. Physiotherapists have to explain why that is not true, because if the patient doesn’t understand why this is incorrect, they will continue to believe it. | ||
When a physiotherapist meets an overweight patient who can’t do the exercises required for treatment, they should sensitively express their concern about their body weight and check their BMI (It never pays to get the client offside). | |||
< | If the [[Physiotherapy communication approaches in management of obesity and overweight|BMI]] is | ||
* 25 or less the physiotherapist should provide health promotion information | |||
* between 25 and 28, they should offer simple weight control advice, such as amount of calories consumed in relation to physical activity levels<ref name="Avenell">Avenell, A, Sattar, N & Lean, M (2007) Management: Part I- Behaviour change, diet and activity. In Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.</ref>. | |||
* over 30 offer education about health risks and offer simple weight control advice, such as amount of calories consumed in relation to physical activity levels<ref name="Avenell" />. | |||
If the patient wants to lose weight, the physiotherapist should advise the patient to go to their doctor to devise a strategy for weight loss, which would include the help of other health professionals such as dietitians, nutritionists and behaviour therapy. <ref name="NICE" /> | |||
< | On the other hand, if the patient does not want to lose weight the physiotherapist should advise see their doctors for regular health checks<ref name="NICE">National Institutes Of Health (1998) Clinical Guidelines On The Identification, Evaluation And Treatment Of Overweight And Obesity In Adults-The Evidence Report. NIH Publication No. 98-4083.</ref>.. | ||
===Nutrition=== | |||
In the obese the dietary modification should be individualized with close monitoring of regular weight loss. | |||
* Low-calorie diets are recommended. Low calorie could be carbohydrate or fat restricted. | |||
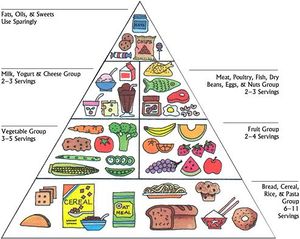
*[[File:Food pyramid usda.jpg|right|frameless]]A low-carbohydrate diet can produce greater weight loss in the first months compared to a low-fat diet. A study finding highlights that different forms of calcium (Calcium citrate and Vit D), in combination with low-calorie, higher carbohydrate diet, may trigger changes in body mass or body composition<ref>Kerksick CM, Roberts MD, Campbell BI, Galbreath MM, Taylor LW, Wilborn CD, Lee A, Dove J, Bunn JW, Rasmussen CJ, Kreider RB. [https://pubmed.ncbi.nlm.nih.gov/32156010/ Differential impact of calcium and vitamin D on body composition changes in post-menopausal women following a restricted energy diet and exercise program.] Nutrients. 2020 Mar;12(3):713.</ref>. | |||
* The patient's adherence to their diet should frequently be emphasized. | |||
Health professionals can | |||
In | * Encourage healthy eating, consisting on the 5 food types, information can be given to patients via the “eatwell plate” model<ref name="Scottish">Scottish Intercollegiate Guidelines (2011)Management Of Obesity- Quick Reference Guide. [Online] Edinburgh. Scottish Intercollegiate Guidelines Network. Available from http://www.sign.ac.uk/pdf/qrg115.pdf [Accessed 13/3/2012]</ref>. | ||
* Make patients aware of the numerous benefits of modest weight loss<ref>Scottish Intercollegiate Guidelines (2011)Management Of Obesity- Quick Reference Guide. [Online] Edinburgh. Scottish Intercollegiate Guidelines Network. Available from http://www.sign.ac.uk/pdf/qrg115.pdf [Accessed 13/3/2012]</ref> eg reduced risk of cancer, diabetes and the holistic benefit of having an improved physical, social and mental well being. <br>Physiotherapists are not responsible for setting goals or weight management programmes, therefore it is vital that they understand the importance of referral to a specialist.<ref>Scottish Intercollegiate Guidelines (2011)Management Of Obesity- Quick Reference Guide. [Online] Edinburgh. Scottish Intercollegiate Guidelines Network. Available from http://www.sign.ac.uk/pdf/qrg115.pdf [Accessed 13/3/2012]</ref> | |||
* Physiotherapists should make patients aware about when they are more likely to put on weight eg, pregnancy, menopause and adjust accordingly | |||
Health professionals could get involved with the food industry and the environment in order to try and promote physical activity, healthy eating and better self confidence. In reality this would be extremely difficult to do because fast food companies are making their products for a profit, not for health issues. What they are doing now is making them a huge profit so why would they try to change when they are being very successful?<ref name="Lean 2007" /> | |||
NB Physiotherapists should “practice what they preach” and follow a healthy diet themselves!<ref name="Lean 1998">Lean, M (1998) Clinical Handbook of Weight Management. London. Martin Dunitz Ltd</ref>. | |||
== Physiotherapy Management == | == Physiotherapy Management == | ||
[[Management of Obesity]] | [[Management of Obesity]] | ||
[ | [[Childhood Obesity]] | ||
== References == | |||
== References | |||
<references /><br> | <references /><br> | ||
[[Category:Obesity]] [[Category: | [[Category:Obesity]] | ||
[[Category:Global Health]] | |||
[[Category:Course Pages]] | |||
Latest revision as of 22:57, 18 October 2023
Original Editor - Lizzie_White
Top Contributors - Admin, Vanessa Rhule, Lucinda hampton, Kim Jackson, Vidya Acharya, Lizzie White, Tony Lowe, Simisola Ajeyalemi, 127.0.0.1, WikiSysop, Rucha Gadgil and Scott Buxton
Introduction[edit | edit source]

Obesity is the excessive accumulation of adipose tissue in the body, that may impair health, due to consuming more food than is required for energy[1][2].
- According to the WHO in 2016 1.9 billion people were overweight, 600 million of these were obese and alarmingly 41 million children under the age of 5 were overweight or obese.[3]
- By 2030 some epidemiologists suggest that 20% of the world's population will be obese, i.e., having a body mass index (BMI) of more than 30 kg/m² in adults, or a BMI ≥95th percentile for age and sex in children aged 2 to 18 years[4]. it is also vital to check waist measurement and body composition. Obesity correlates with increasing an individual’s risk of cancers, stroke, metabolic disease, heart failure, and other cardiovascular conditions,
- As research into obesity continues new definitions emerge, one being normal weight obesity. This refers to individuals with normal body weight by body mass index (BMI) but a high body fat percentage. This group of people are at a notably increased risk of developing metabolic syndrome, cardiometabolic dysfunction and increased mortality[5].
Etiology[edit | edit source]
Obesity is the result of an imbalance between daily energy intake and energy expenditure resulting in excessive weight gain. Obesity is caused by multiple factors which can be

- genetic
- cultural
- societal
- reduced physical activity
- insomnia
- food habits
- endocrine disorders
- medications,
- food advertisements
- energy metabolism[6].
Epidemiology[edit | edit source]

According to the WHO in 2016 1.9 billion people were overweight, 600 million of these were obese and alarmingly 41 million children under the age of 5 were overweight or obese[3].
- Nearly one-third of adults and about 17% of adolescents in the United States are obese.
- Recent statistics show that nearly a quarter of the UK adult population are obese and obesity is rising quickly, every year obesity in the UK costs the economy £3.5bn[2].
- According to Center for Disease Control and Prevention (CDC), 2011 to 2012 data, one out of five adolescents, one out of six elementary school age children, and one out of 12 preschool age children are obese.[6]
- Obesity is more prevalent in African Americans, followed by Hispanics and whites. Southern US states have the highest prevalence, followed by the Midwest, Northeast and the west.
- Obesity is a global problem with rates even higher than what are seen in North America.[6]
Deemed Obese in England, figures (see the need for concern!)
- 1980, 6% of men and 8% of women
- 1995 15% of men and 16.5% of women were classed as obese[7].
- 2010, 23.6% of men and 23.8% of women in England were obese. Obesity levels in Scotland were slightly higher in women with 26% being obese[2].
Obesity is a significant risk for developing Type 2 Diabetes, with 90% of diabetes diagnosis being type 2. There are over 422 million people worldwide living with diabetes[8] and in 2012 1.5 million people died as a direct result of this disease.
How Physiotherapists Can help[edit | edit source]
Physiotherapists, as exercise experts, join the worldwide concern for the ever-growing epidemic of obesity, which affects adults and children alike[9]. It is probably one of the greatest challenges to our health systems around the world in the 21st century.
There are two important interventions to prevent and manage obesity.
- Optimal nutrition.
- Increased exercise and physical activity. The potential contribution of physical therapists to the latter approach is immense.[10]
Physiotherapists can introduce the idea of utilizing exercise as a means of reducing obesity (i.e., reducing fat mass) and associated benefits.
- Fitness is associated with more desirable clinical outcomes in many instances, such as decreasing metabolic disease, cardiovascular disease, Alzheimer disease risk, inflammation, and many other disease.
- If the patient is able to exercise, exercise may be the preferred route to decrease disease symptoms and/or future risk compared to alternative pharmaceuticals that may exacerbate symptoms.
- An open and communicative relationship between the physiotherapist and the patient must be present in order to suggest the addition of exercise to the patient's lifestyle in order to decrease obesity and improve negative side effects.
Exercise and Physical Activity[edit | edit source]
Physical activity is any movement of the body that requires the use of our skeletal muscles, which in turn requires energy expenditure. This energy expenditure is basic to weight control.
- Aerobic exercise prescriptions and recommendations for strength/resistance training must go hand in hand with reduced food intake, and the progression of activity should be gradual, scientifically based, and tailored individually to each person.
- It is important that the physiotherapist finds the most appropriate activity for the individual, so that they will not only enjoy the activity but also have a greater chance of staying with it.
- There are numerous types of exercise prescriptions that the physiotherapist may use in their increasing effort to battle the obesity epidemic.
The sooner all our nations begin to adopt initiatives and programmes to combat obesity and other diseases of civilisation, the less will be the burdens on health systems delivery around the world.
- Obesity is reaching epidemic proportions and the topic of obesity is a core part in medical curricula[11].
- Every time a health professional has the opportunity to see a patient, they should be able to assess the patient to see if they have a weight problem and either refer them to a specialist or offer simple advice[11].
- Physiotherapists have a key role to play in trying to reverse this trend as they often use exercise as a form of treatment, so if a patient is too overweight to do exercise, it becomes harder for the treatment to be successful[12].
A cross-sectional study performed in 115 children in Japan assessing the factors associated with excess weight in children suggest that decreasing children's sedentary behavior in addition to more physical activity is essential for the prevention of overweight status and obesity in high-risk children with lifestyle diseases[13]. Study results suggest that aerobic exercise is more relevant than resisted exercise training in modulating inflammatory cytokines and quality of life among obese post-menopausal women[14].
A pilot trial found that ferritin in postmenopausal women participating in Resisted Training (RT) over 15 weeks positively correlated with ferritin, total cholesterol, low-density lipoprotein, and non-high-density lipoprotein cholesterol while negatively correlated with HDL. However, a large-scale cohort is needed to confirm these findings[15].
Patient Education[edit | edit source]

One of the main roles of a physiotherapist regarding obesity is educating patients.
Many people are falsely led to believe that they can lose weight without putting in effort or changing from a sedentary lifestyle[12]. Physiotherapists have to explain why that is not true, because if the patient doesn’t understand why this is incorrect, they will continue to believe it.
When a physiotherapist meets an overweight patient who can’t do the exercises required for treatment, they should sensitively express their concern about their body weight and check their BMI (It never pays to get the client offside).
If the BMI is
- 25 or less the physiotherapist should provide health promotion information
- between 25 and 28, they should offer simple weight control advice, such as amount of calories consumed in relation to physical activity levels[16].
- over 30 offer education about health risks and offer simple weight control advice, such as amount of calories consumed in relation to physical activity levels[16].
If the patient wants to lose weight, the physiotherapist should advise the patient to go to their doctor to devise a strategy for weight loss, which would include the help of other health professionals such as dietitians, nutritionists and behaviour therapy. [17]
On the other hand, if the patient does not want to lose weight the physiotherapist should advise see their doctors for regular health checks[17]..
Nutrition[edit | edit source]
In the obese the dietary modification should be individualized with close monitoring of regular weight loss.
- Low-calorie diets are recommended. Low calorie could be carbohydrate or fat restricted.
- A low-carbohydrate diet can produce greater weight loss in the first months compared to a low-fat diet. A study finding highlights that different forms of calcium (Calcium citrate and Vit D), in combination with low-calorie, higher carbohydrate diet, may trigger changes in body mass or body composition[18].
- The patient's adherence to their diet should frequently be emphasized.

Health professionals can
- Encourage healthy eating, consisting on the 5 food types, information can be given to patients via the “eatwell plate” model[19].
- Make patients aware of the numerous benefits of modest weight loss[20] eg reduced risk of cancer, diabetes and the holistic benefit of having an improved physical, social and mental well being.
Physiotherapists are not responsible for setting goals or weight management programmes, therefore it is vital that they understand the importance of referral to a specialist.[21] - Physiotherapists should make patients aware about when they are more likely to put on weight eg, pregnancy, menopause and adjust accordingly
Health professionals could get involved with the food industry and the environment in order to try and promote physical activity, healthy eating and better self confidence. In reality this would be extremely difficult to do because fast food companies are making their products for a profit, not for health issues. What they are doing now is making them a huge profit so why would they try to change when they are being very successful?[11]
NB Physiotherapists should “practice what they preach” and follow a healthy diet themselves![22].
Physiotherapy Management[edit | edit source]
References[edit | edit source]
- ↑ Maguire, T & Haslam, D (2010) The Obesity Epidemic and Its Management [Online] London. Pharmaceutical Press. Available from http://lib.myilibrary.com/Open.aspx?id=239868&src=0 [Accessed 6/3/2012]
- ↑ 2.0 2.1 2.2 Haslam, D, Sattar, N & Lean, M (2007) Obesity- time to wake up. In: Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.
- ↑ 3.0 3.1 World Health Organisation. Obesity and overweight factsheet. http://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight [Accessed 3 Dec 2018]
- ↑ Tirthani E, Said MS, Rehman A. Genetics and Obesity. StatPearls [Internet]. 2021 Aug 4.Available:https://https://www.statpearls.com/ArticleLibrary/viewarticle/131519 (accessed 13.11.2021)
- ↑ Mohammadian Khonsari N, Baygi F, Tabatabaei-Malazy O, Mohammadpoor Nami S, Ehsani A, Asadi S, Qorbani M. Association of normal weight obesity phenotype with inflammatory markers: A systematic review and meta-analysis. Frontiers in Immunology. 2023 Feb 27;14:1044178.Available:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10010388/ (accessed 29.9.2023)
- ↑ 6.0 6.1 6.2 Kiran K. Panuganti; Ravi K. Kshirsagar. ☀October 28, 2019 Obesity . Available from:https://www.ncbi.nlm.nih.gov/books/NBK459357/ (last accessed 15.2.2020)
- ↑ Anderson, P & Butcher, K (2006) Childhood Obesity: Trends and Potential Causes, The Future of Children, 16 (1) Princeton University and The Brookings Institution.
- ↑ World Health Organisation. World Health Day 2016: Beat diabetes http://www.who.int/campaigns/world-health-day/2016/en/ [Accessed 3 Dec 2018]
- ↑ Crawley, J (2006) Markets and Childhood Obesity Policy, The Future of Children, 16 (1) Princeton University and The Brookings Institution.
- ↑ Dr Marilyn Moffat, President of the WCPT. How physical therapists fight non-communicable fckLRdisease throughout the lifespan. 2011
- ↑ 11.0 11.1 11.2 Lean, M, & Lara, J & O Hill, J (2007) Strategies for preventing obesity. In: Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.
- ↑ 12.0 12.1 Bird, S (1992) Exercise Physiology For Health Professionals. London. Chapman & Hall.
- ↑ NAKANO S, HIRANO C, HOTTA K, FUJITA Y, YANAGI H. Factors associated with overweight status, obesity, and sedentary behavior in elementary and junior high school students. Physical Therapy Research. 2019 Dec 20;22(2):66-72.
- ↑ Abd El-Kader SM, Al-Jiffri OH. Impact of aerobic versus resisted exercise training on systemic inflammation biomarkers and quality of Life among obese post-menopausal women. African Health Sciences. 2019;19(4):2881-91.
- ↑ Ward LJ, Hammar M, Lindh-Åstrand L, Berin E, Lindblom H, Rubér M, Holm AC, Li W. Does resistance training have an effect on levels of ferritin and atherogenic lipids in postmenopausal women?–A pilot trial. Scientific reports. 2020 Mar 2;10(1):1-8.
- ↑ 16.0 16.1 Avenell, A, Sattar, N & Lean, M (2007) Management: Part I- Behaviour change, diet and activity. In Sattar, N & Lean, M (eds.) ABC of Obesity. Oxford, Blackwell Publishing.
- ↑ 17.0 17.1 National Institutes Of Health (1998) Clinical Guidelines On The Identification, Evaluation And Treatment Of Overweight And Obesity In Adults-The Evidence Report. NIH Publication No. 98-4083.
- ↑ Kerksick CM, Roberts MD, Campbell BI, Galbreath MM, Taylor LW, Wilborn CD, Lee A, Dove J, Bunn JW, Rasmussen CJ, Kreider RB. Differential impact of calcium and vitamin D on body composition changes in post-menopausal women following a restricted energy diet and exercise program. Nutrients. 2020 Mar;12(3):713.
- ↑ Scottish Intercollegiate Guidelines (2011)Management Of Obesity- Quick Reference Guide. [Online] Edinburgh. Scottish Intercollegiate Guidelines Network. Available from http://www.sign.ac.uk/pdf/qrg115.pdf [Accessed 13/3/2012]
- ↑ Scottish Intercollegiate Guidelines (2011)Management Of Obesity- Quick Reference Guide. [Online] Edinburgh. Scottish Intercollegiate Guidelines Network. Available from http://www.sign.ac.uk/pdf/qrg115.pdf [Accessed 13/3/2012]
- ↑ Scottish Intercollegiate Guidelines (2011)Management Of Obesity- Quick Reference Guide. [Online] Edinburgh. Scottish Intercollegiate Guidelines Network. Available from http://www.sign.ac.uk/pdf/qrg115.pdf [Accessed 13/3/2012]
- ↑ Lean, M (1998) Clinical Handbook of Weight Management. London. Martin Dunitz Ltd

