Avulsion Fractures of the Ankle: Difference between revisions
m (Text replace - '- Your name will be added here if you are a lead editor on this page.' to ' ') |
m (Text replace - ''''Lead Editors'''' to ''''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}}') |
||
| Line 2: | Line 2: | ||
'''Original Editors ''' - [[User:Niels Verbeeck|Niels Verbeeck]] | '''Original Editors ''' - [[User:Niels Verbeeck|Niels Verbeeck]] | ||
''' | '''Top Contributors''' - {{Special:Contributors/{{FULLPAGENAME}}}} | ||
</div> | </div> | ||
== Search Strategy == | == Search Strategy == | ||
Revision as of 16:37, 14 June 2013
Original Editors - Niels Verbeeck
Top Contributors - Niels Verbeeck, Kim Jackson, Admin, Pierreux Maarten, Shaimaa Eldib, Scott Cornish, Uchechukwu Chukwuemeka, Vidya Acharya, Rachael Lowe, Jan Alderweireldt, Claire Knott, Wanda van Niekerk, Lucinda hampton and 127.0.0.1
Search Strategy[edit | edit source]
Key words: Avulsion fractures, ankle, 5th metatarsal, treatment, diagnosise
An avulsion fracture of the 5th metatarsal is also called Pseudo-Jones fracture.
Main information: VUB (Free University of Brussels) library (books) and sites: Pubmed, Web of knowledge (RCT’s), PEDro evidence
Definition/Description
[edit | edit source]
An avulsion fracture is a fracture caused by a traumatic traction (longterm repetitive pulling or single high impact traumatic traction) from a tendon to the bone. Because the tendon can bear more pull than the bone, it is common that the bone will pull off instead of the tendon. The tendon pulls off a tiny fragment of bone.[1] [2]
An avulsion fracture can occur at many places in the body, but some areas in the body are more sensitive than others. An avulsion fracture of the ankle is mostly situated at the base of the fifth metatarsal, but may also be found at the talus and calcaneus.
Clinically Relevant Anatomy[edit | edit source]
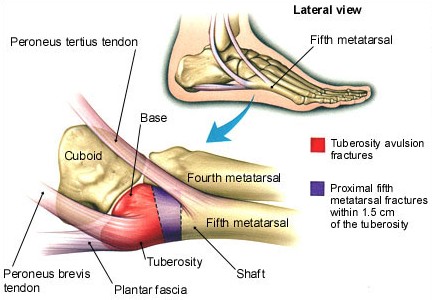
The 5th metatarsal is located at the lateral side of the foot. The metatarsal is divided into 3 parts: the base (also called tuberosity), the metaphysis and the head. The peroneus (fibularis) brevis’ is attached at the lateral side of the tuberosity metatarsal V.(red area at figure) The peroneus (fibularis) tertius’ is attached at the dorsal side of the most proximal compartment of the metaphysis. Because of large traction by these structures, during inversion injury, tuberosity avulsion fractures occur. (between red and purple area at figure)
figure1: source: http://www.med-info.nl/images/images_trauma/Trauma_voet_MT5_Jones_groot.jpg
Epidemiology /Etiology[edit | edit source]
add text here
Characteristics/Clinical Presentation[edit | edit source]
add text here
Differential Diagnosis[edit | edit source]
Avulsion fractures are often confused with other types of fractures to the fifth metatarsal:
- Jones fractures
- Stress fractures
- Mid-shaft fractures
Diagnostic Procedures[edit | edit source]
An x-ray may be ordered by the surgeon. Avulsion fractures are sometimes overlooked when an x-ray is taken or when the injury to MT V occurs together with an ankle sprain. In this case other imaging studies are recommended, such as MR imaging, CT scan or scintigrams. [2] [3] [4]
Outcome Measures[edit | edit source]
add links to outcome measures here (also see Outcome Measures Database)
Examination[edit | edit source]
During the medical history taking the surgeon or a physiotherapist has to ask the patient how the injury occurred and when the pain started. Using the Ottawa Ankle Rules localize the exact area of pain. Palpation of the 5th metatarsal tuberosity is painfull.
Medical Management[edit | edit source]
Patients with an avulsion fracture of the base of the 5th metatarsal are usually treated conservative. If the bone is not displaced, the treatment is accomplished with a walking boot or a walking cast. They will be casted for four to six weeks. Surgery is only recommended if the bone is displaced from its normal position or when there is more than 30% of the cubometatarsal joint involved. The bone will be removed or fixed with osteosynthesis material. Crutches may be useful to avoid weight on the injured foot. [5]
Physical Therapy Management
[edit | edit source]
Avulsion fractures are often treated as ankle sprains. A physiotherapist doesn’t treat ‘an avulsion fracture’ on its own, but the dysfunctional movement and impairments of an individual. Therefore it is important to individualize the treatment. [4]
It is important to follow a full ankle rehabilitation after an avulsion fracture, because inappropriately managed avulsion fractures can lead to significant long-term functional disability. Most fractures heal well, but following a strict immobilization it is indicated to regain full range of motion (normal arthrokinematics), strength of the lower extremity muscles, proprioception and functionality in sport.
A full ankle rehabilitation after an avulsion fracture consists of three phases, the acute phase, the recovery phase and the functional phase:
- The first phase, also called ‘the acute phase’, can be started at two weeks postoperatively. The first phase will include passive range of motion exercises and crytherapy. This phase is based on the reduction of pain, inflammation and edema while retarding muscle atrophy of the lower extremity complex.
- The second phase, also called ‘the recovery phase’, can be started after the patient has met the goals of the first phase, usually at three to four weeks postoperatively. The second phase includes range of motion exercises, exercises improving lower extremity strength with theraband and proprioception exercises with a biomechanical ankle platform system. At the beginning of the second phase, advice the patients they should use the least resistant band. Toward the end of the second phase, the patient should begin using a wobble board to improve proprioception and begin closed kinetic chain activities (walking and loading).
- The third phase, also called ‘the functional phase’, can be started at six to eight weeks postoperatively. The third phase involves increasing power of the lower extremity complex, increasing neuromuscular control and utilizing sport-specific training of the lower extremity for a full return to sport. [6]
Key Research[edit | edit source]
add links and reviews of high quality evidence here (case studies should be added on new pages using the case study template)
Resources
[edit | edit source]
Articles:
- E.W. Zwitser *, R.S. Breederveld, Fractures of the fifth metatarsal; diagnosis and treatment, Injury, Int. J. Care Injured 41 (2010) 555–562 (level: A1)
- Haraguchi N, Toga H, Shiba N, Kato F, Avulsion fracture of the lateral ankle ligament complex in severe inversion injury: incidence and clinical outcome, Am J Sports Med. 2007 Jul;35(7):1144-52 (level: A2)
- Peter Vorlat , Wim Achtergael , Patrick Haentjens, Predictors of outcome of non-displaced fractures of the base of the fifth metatarsal, International Orthopaedics (SICOT) (2007) 31: 5–10 (level: B)
- Duke G. Pao, Theodore E. Keats, Robert G. Dussault, Avulsion Fracture of the Base of the Fifth Metatarsal Not Seen on Conventional Radiography of the Foot: The Need for an Additional Projection, AJR 2000;175:549–552 (level: C)
Books:
- David F. Paton. Fractures and Orthopaedics. Edinburgh: Churchill Livingstone, 1988.
- Ronald McRace. Practical Fracture Treatment. 3rd ed. Edinburgh: Churchill Livingstone, 1994.
Sites:
- http://orthopedics.about.com/od/brokenbones/a/avulsion.htm
- http://www.foothealthfacts.org/footankleinfo/fifth-metatarsal_fractures.htm
- http://www.podiatrytoday.com/article/6565
Clinical Bottom Line[edit | edit source]
add text here
Recent Related Research (from Pubmed)[edit | edit source]
see tutorial on Adding PubMed Feed
Extension:RSS -- Error: Not a valid URL: Feed goes here!!|charset=UTF-8|short|max=10
References[edit | edit source]
see adding references tutorial.
- ↑ http://orthopedics.about.com/od/brokenbones/a/avulsion.htm
- ↑ 2.0 2.1 http://www.foothealthfacts.org/footankleinfo/fifth-metatarsal_fractures.htm
- ↑ Duke G. Pao, Theodore E. Keats, Robert G. Dussault, Avulsion Fracture of the Base of the Fifth Metatarsal Not Seen on Conventional Radiography of the Foot: The Need for an Additional Projection, AJR 2000;175:549–552
- ↑ 4.0 4.1 Haraguchi N, Toga H, Shiba N, Kato F, Avulsion fracture of the lateral ankle ligament complex in severe inversion injury: incidence and clinical outcome, Am J Sports Med. 2007 Jul;35(7):1144-52
- ↑ E.W. Zwitser *, R.S. Breederveld, Fractures of the fifth metatarsal; diagnosis and treatment, Injury, Int. J. Care Injured 41 (2010) 555–562
- ↑ http://www.podiatrytoday.com/article/6565


{kind=link}
{kind=link}