Axillary Nerve Injury
Original Editors
Lead Editors - Your name will be added here if you are a lead editor on this page. Read more.
Search Strategy[edit | edit source]
Search Databases: CINHAL, Cochrane Library, EBSCO, Medline with Full Text, ProQuest, PubMed, SAGE, ScienceDirect, SpringerLink
Search Terms: anterior shoulder dislocation, axillary nerve, axillary nerve rehabilitation, axillary neuropathy, axillary nerve fracture, instability conservative treatment, nerve injury with anterior dislocation, physical therapy axillary, physical therapy shoulder dislocation, shoulder dislocation, shoulder dislocation nerve, and shoulder dislocation peripheral nerve
Search Timeline: 10/11/2010-11/23/2010
Definition/Description[edit | edit source]
It is characterized by trauma to the axillary nerve from either a compressive force or traction injury following anterior dislocation of the shoulder.[1][2][3][4][5][6][7][8][9][10]
Epidemiology/Etiology[1][2][3][4][5][6][7][8][9][10][edit | edit source]
- Anterior dislocation is the most common occurring dislocation at the shoulder.[2][3][4][5][6][8][9]
- Men and women 3:1[5]
- 9-65% involve axillary nerve injury[2][8][9][11][12]
- 23% have combination neuropathies, all involving the axillary nerve[8]
- The incidence of brachial plexus and axillary nerve injury increases dramatically following shoulder dislocation in patients ≥50 years of age, if fracture is associated with the dislocation, and if the duration of the dislocation lasts >12 hours[8][9][10][13][14]
- Incidence of nerve injury doubled with the presence of an associated fracture[10]
- Incidence of nerve injury doubled with the presence of an associated fracture[10]
- Traction and compression to the axillary nerve[1][2][6][7][9][10][2]
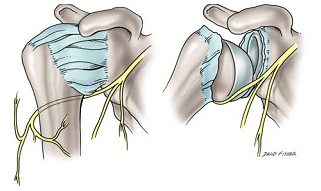 Figure 1- Depiction of the axillary nerve stretched across the humeral head during dislocation.
Figure 1- Depiction of the axillary nerve stretched across the humeral head during dislocation.- The axillary nerve becomes stretched across the humerus as it dislocates anteriorly and inferiorly.[2][9]
- Propagated tension due to overstretching of the axillary nerve over the humeral head during shoulder dislocations may cause elongation of the free portion of the axillary nerve and the increased tension may even result in axillary nerve avulsions from the posterior cord of brachial plexus.[2][9]
- The axillary nerve is susceptible to injury at several sites, including the origin of the nerve from the posterior cord, the anterior inferior aspect of the subscapularis muscle and shouler capsule, the quadrilateral space, and within the subfascial surface of the deltoid uscle.[9]
- The axillary nerve becomes stretched across the humerus as it dislocates anteriorly and inferiorly.[2][9]


Characteristics/Clinical Presentation[edit | edit source]
It is important to note that the clinical presentation of axillary nerve dysfunction is variable and can go undetected, as the concomitant dislocation or fracture may mask the symptoms.[1][9] Nerve injury should be considered as part of the differential diagnosis process when a patient reports pain, weakness, or paresthesias.[7]
- Subjective Examination
- Generalized mild, dull, and achy pain to the deep or lateral shoulder, with occasional radiation to the proximal arm [4][6][15][16]
- Numbness and tingling of the lateral arm and/or posterior aspect of the shoulder [4][6][7][9][14][16]
- In some cases, persisting 2-4 weeks post-injury
- In some cases, persisting 2-4 weeks post-injury
- Feeling of instability[16]
- Weakness, especially with flexion, abduction, and external rotation [6][9][15][16]
- Fatigue, especially with overhead activities, heavy lifting, and/or throwing [7][14][15]
- May/or may not reveal a history of trauma to the shoulder region [4][6]
- History of dislocation with soreness persisting ~1week post-injury [16]
- Easing Factors include: rest, ice, analgesics, and anti-inflammatory medications [6][7][17]
- Generalized mild, dull, and achy pain to the deep or lateral shoulder, with occasional radiation to the proximal arm [4][6][15][16]
Many athletes with axillary nerve injury may be asymptomatic with incomplete or complete lesions, with the only complaints of weakness and early-onset fatigue with exercise. [4][14]
Differential Diagnosis[edit | edit source]
Axillary nerve injury with shoulder dislocation can present similarly to or concomitantly with the following conditions: [9][13][15]
- “Unhappy Triad”
- Quadrilateral Space Syndrome (QSS)
- Posterior Cord of the Brachial Plexus Injury
- C5-6 Radiculopathy
- Parsonage-Turner Syndrome (PTS)
"Unhappy Triad"[edit | edit source]
The “Unhappy Triad” consists of a shoulder dislocation that results in both a rotator cuff tear and axillary nerve injury.
- Occurs in 9-18% of anterior shoulder dislocations[8]
- Risk of an “unhappy triad” with anterior shoulder dislocation increases after the age of 40[8]
Quadrilateral space syndrome(QSS)[edit | edit source]
QSS is an “uncommon condition that involves the compression of the posterior humeral circumflex artery and the axillary nerve within the quadrilateral space,” secondary to an acute trauma or from overuse, especially with overhead sports like throwing and swimming.[17]
- 4 Cardinal Features[17]
- Generalized shoulder pain
- Paresthesias in a nondermatomal pattern
- Point tenderness to the quadrilateral space
- (+) arteriogram findings with the shoulder in abduction and external rotation
- Symptoms are typically present with the arm in an overhead position, especially in late cocking or the early acceleration phases of throwing[17]
Parsonage-Turner Syndrome(PTS)[edit | edit source]
PTS is an uncommon, idiopathic condition, characterized by an acute onset of intense pain, without a mechanism of injury, that subsides within days-weeks, leaving behind residual weakness/paralysis in upper extremity muscles.[18]
- Symptoms are NOT related to neck movements.
- Aka: Acute brachial neuritis
Examination[edit | edit source]
add text here
Medical Management (current best evidence)[edit | edit source]
add text here
Physical Therapy Management (current best evidence)[edit | edit source]
add text here
Key Research[edit | edit source]
There is only minimal, low quality evidence regarding isolated axillary nerve injury in shoulder dislocations, consisting mostly of descriptive and exploratory studies.
- Nerve Injury About the Shoulder in Athletes, Part 1- A descriptive study that reviews the anatomy of the axillary nerve, presentation and clinical examination, diagnostic tests, differential diagnosis, and treatment of axillary nerve injury, with emphasis on early recognition and diagnosis of this type of injury.
- Axillary Nerve Injuries in Contact Sports: Recommendations for Treatment and Rehabilitation- A descriptive study that discusses the relevant anatomy, proper examination and diagnosis of the axillary nerve injury, differential diagnosis (to include cervical spine clearing), conservative treatment, indications for surgical intervention, complications and prognosis, and rehabilitation. In regards to treatment, there is emphasis placed on the axillary nerve injury in conjunction with the shoulder dislocation.
- Diagnosis of Isolated Axillary Neuropathy in Athletes: Case Studies- The most recent case studies in the diagnosis of axillary nerve injury.
Resources
[edit | edit source]
add appropriate resources here
Clinical Bottom Line[edit | edit source]
add text here
Recent Related Research (from Pubmed)[edit | edit source]
see tutorial on Adding PubMed Feed
References[edit | edit source]
see adding references tutorial.
- ↑ 1.0 1.1 1.2 1.3 1.4 Allen J, Dean K. Recognizing, managing, and testing an axillary- nerve dysfunction. Athletic Therapy Today. 2002;7(2):28-29.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 2.8 Apaydin N, Tubbs S, Loukas M, Duparc F. Review of the surgical anatomy of the axillary nerve and the anatomic basis of its iatrogenic and traumatic injury. Springer. 2010;32:193-201.
- ↑ 3.0 3.1 3.2 Cutts S, Prempeh M, Drew S. Anterior shoulder dislocation. Ann R Coll Surg Engl. 2009:91:2-7.
- ↑ 4.0 4.1 4.2 4.3 4.4 4.5 4.6 Duralde X. Neurologic injuries in the athlete’s shoulder. Journal of Athletic Training. 2000;35(3):316-328.
- ↑ 5.0 5.1 5.2 5.3 Handoll HHG, Hanchard NCA, Goodchild LM, Feary J. Conservative management following closed reduction of traumatic ; anterior dislocation of the shoulder (review). Cochrane Database of Systematic Review. 2006;1:1-26.
- ↑ 6.0 6.1 6.2 6.3 6.4 6.5 6.6 6.7 6.8 6.9 Miller T. Peripheral nerve injuries at the shoulder. The Journal of Manual& Manipulative Therapy. 1998;6(4)170-183.
- ↑ 7.0 7.1 7.2 7.3 7.4 7.5 7.6 Neal S, Fields K. Peripheral nerve entrapment and injury in the upper extremity. American Family Physician. 2010; 81(2): 147-155.
- ↑ 8.0 8.1 8.2 8.3 8.4 8.5 8.6 8.7 Payne M, Doherty T, Sequeira K, Miller T. Peripheral nerve injury associated with shoulder trauma: a retrospective study and review of literature. Journal of Clinical Neuromuscular Disease. 2002; 4(1): 1-6.
- ↑ 9.00 9.01 9.02 9.03 9.04 9.05 9.06 9.07 9.08 9.09 9.10 9.11 9.12 Perlmutter G, Apruzzese W. Axillary nerve injuries in contact sports: recommendations for treatment and rehabilitation. Sports Med. 1998;26(5): 351-360.
- ↑ 10.0 10.1 10.2 10.3 10.4 Visser C, Coene L, Brand R, Tavy D. The incidence of nerve injury in anterior dislocation of the shoulder and its influence on functional recovery a prospective clinical and emg study. Journal of Bone and Joint Surgery. British volume. 1999; 81-B(4). 679-685.
- ↑ Cox C, Kuhn J. Operatice versus nonoperative treatment of acute shoulder dislocation in the athlete. Current Sports Medicine Reports. 2008;7(5): 263-268.
- ↑ McFarland E, Caicedo J, Kim T, Banchasuek P. Axillary nerve injury in anterior shoulder reconstructions: use of a subscapularis muscle- splitting technique and a review of the literature. Am J Sports Med. 2002;30:601-606.
- ↑ 13.0 13.1 Kazemi M. Acute traumatic anterior glenohumeral dislocation complicated by axillary nerve damage: a case report. Journal of the Canadian Chiropractic Association. 1998;42(3):150-155.
- ↑ 14.0 14.1 14.2 14.3 Safran M. Nerve injury about the shoulder in athletes, Part 1: Suprascapular nerve and axillary nerve. Am J Sports Med . 2004;32(3):803-819.
- ↑ 15.0 15.1 15.2 15.3 15.4 Vitanzo P, Kenneally B. Diagnosis of isolated axillary neuropathy in athletes:case studies. The Journal of Musculoskeletal Medicine. 2009; 26:307-311.
- ↑ 16.0 16.1 16.2 16.3 16.4 Miller T. Axillary neuropathy following traumatic dislocation of the shoulder: a case study. The Journal of Manual & Manipulative Therapy. 1998;6(4):184-185.
- ↑ 17.0 17.1 17.2 17.3 Manske R, Sumler A, Runge J. Quadrilateral space syndrome. Humen Kinetics-ATTI.2009;14(2):45-47.
- ↑ Mamula C, Erhard R, Piva S. Cervical radiculopathy or parsonage-turner syndrome: differential diagnosis of a patient with neck and upper extremity symptoms. Journal of Orthopaedic & Sports Physical Therapy. 2005; 55(10): 659-664.

