Ober's Test
Original Editor - Nicole Kluckhohn, Agapi Hakobyan
Top Contributors - Vidya Acharya, Agapi Hakobyan, Admin, Paige Canada, Madison Hagen, Nicole Kluckhohn, Ben Kasehagen, Tony Varela, Victoria Morris, Kim Jackson, Rachael Lowe, Merlin Roggeman, Tony Lowe, Tarina van der Stockt, Chrysolite Jyothi Kommu, Kai A. Sigel, Wanda van Niekerk, Oyemi Sillo and Sweta Christian
Purpose[edit | edit source]
The Ober's test evaluates a tight, contracted or inflamed Tensor Fasciae Latae (TFL) and Iliotibial band (ITB). The Ober’s test must not be confounded with Noble’s test and the Renne test, two other tests that are commonly used to detect iliotibial band syndrome.
Clinically Relevant Anatomy[edit | edit source]
Anatomically, the ITB is a continuation of the tendinous portion of the TFL muscle with some contributions from the gluteal muscles. TFL/ITB is a synergist of the gluteus medius muscle in hip abduction[1].
Origin:[edit | edit source]
- TFL originates[2] from- the anterior part of the external lip of iliac crest, the outer surface of an anterior superior iliac spine, and the deep surface of fascia lata.
- Iliotibial band (ITB) or tract is a lateral thickening of the fascia lata in the thigh[3]. Proximally it splits into superficial and deep layers, enclosing tensor fasciae lata and anchoring this muscle to the iliac crest. It also receives most of the tendon of the gluteus maximus.
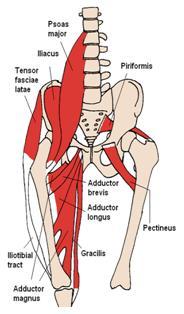 Iliotibial Band and Tensor Fascia Lata
Iliotibial Band and Tensor Fascia Lata

Insertion:[edit | edit source]
- TFL inserts[2] into the ITB at the anterolateral thigh at the junction of proximal and middle thirds of the thigh.
- ITB is generally viewed as a band of dense fibrous connective tissue that passes over the lateral femoral epicondyle and attaches to Gerdy's tubercle[3] on the anterolateral aspect of the tibia.
Action:[edit | edit source]
- TFL flexes, medially rotates, and abducts the hip joint; tenses the fascia lata; and may assist in knee extension[2]. Gluteus medius, gluteus minimus, and upper fibers of the gluteus maximus are the primary synergistic muscles of the hip abductors.
- ITB permits the TFL and Gluteus maximus to influence the stability of the extended knee joint, due to the insertion of these muscles into the ITB[4].
Technique[edit | edit source]
Ober Test[edit | edit source]
Frank Ober described the test for tightness of TFL and ITB in an article entitled "Back Strain and Sciatica", wherein he discussed the relationship of a contracted TFL and ITB to low backache (May 1935). This was later revised in the year 1937 which cautioned on avoiding hip internal rotation and flexion while carrying out the test[5].
Test position[6][7] :[edit | edit source]
- The patient should be in side-lying with the affected side up.
- Bottom knee and hip should be flexed to flatten the lumbar curve.
- Stand behind the patient and firmly stabilize the pelvis/greater trochanter to prevent movement in any direction.
- Grasp the distal end of the patient’s affected leg with your other hand and flex the leg to a right angle at the knee
Test:[edit | edit source]
- Extend and abduct the hip joint.
- Slowly lower the leg toward the table -adduct hip- until motion is restricted.
- Ensure that the hip does not internally rotate and flex during the test and the pelvis must be stabilized. As allowing the thigh to drop in flexion and internal rotation would 'give in' to the tight TFL and not accurately test the length[5].
Results:[edit | edit source]
- If the ITB is normal, the leg will adduct with the thigh dropping down slightly below the horizontal and the patient won't experience any pain; in this case, the test is called negative.
- If the ITB is tight, the leg would remain in the abducted position and the patient would experience lateral knee pain, in this case, the test is called positive.
Modified Ober Test[5][edit | edit source]
A modification of the Ober test was first recommended by Kendalls in Posture and Pain. In this test, there is less strain on the medial aspect of the knee joint, less tension on the patella, less interference by a tight Rectus Femoris and it provides a complete stretch on TFL.
Test position:[edit | edit source]
- The patient is in a side-lying position with underneath leg flexed at hip and knee to flatten the low back.
- The examiner stabilizes the pelvis and keeps the lateral trunk in contact with the table.
- Note: Downward lateral tilt is equivalent to the hip abduction and that would "give in " to a tight TFL.
Test:[edit | edit source]
The examiner extends the leg. Ensure that leg is not internally rotated.
Results:[edit | edit source]
- With the knee straight and the pelvis in a neutral position, the thigh drops about 10 degrees below the horizontal. It is suggestive of normal length.
- The leg fails to drop indicates tight ITB and TFL.
Evidence[edit | edit source]
- There is a limited number of studies to support the validity of this test[10]. A study by Reese et al shows that the use of an inclinometer to measure hip adduction using both the Ober test and the modified Ober test appears to be a reliable method for the measurement of IT band flexibility, and the technique is quite easy to use. It demonstrated a significant difference in ROM between testing with the affected knee flexed vs. extended, with the reliability of .90 and .91 respectively[11]. The modified Ober test allows a significantly greater hip adduction range of motion than the Ober test, the 2 examination procedures should not be used interchangeably for the measurement of the flexibility of the IT band.
- But the study findings in 'An Anatomic Investigation of the Ober Test' [12] by Willet GM et al refutes the hypothesis that the ITB plays a role in limiting hip adduction during either version of the Ober test and question the validity of these tests for determining ITB tightness. The findings underscore the influence of the gluteus medius and minimus muscles as well as the hip joint capsule on Ober test findings. The results of this study suggest that the Ober test assesses the tightness of structures proximal to the hip joint, such as the gluteus medius and minimus muscles and the hip joint capsule, rather than the ITB.
Key Research[edit | edit source]
- The study in Clinical Biomechanics by Gajdosik RL et al showed the hip adduction movement was restricted more with the knee flexed than with the knee extended for both genders (P < 0.009). Thus emphasizing the influence of knee positions and gender on the Ober test for the length of the iliotibial band[13].
- An exercise developed by the Postural Restoration Institute to recruit hamstrings and abdominal muscles showed a significant increase in passive hip-adduction angles (p<0.01) and a decrease in pain (p<0.01), immediately improve Ober's Test measurements in people with lumbopelvic pain. The study[14] showed hamstring/abdominal activation, rather than iliotibial band stretching, may be an effective intervention for addressing lumbopelvic pain and a positive Ober's Test.
- The study shows the effect of ITB stretching and Hamstring and Abdominal activation on positive Ober test in individuals with lumbopelvic pain[15] The hamstring and abdominal activation showed a greater reduction in pain and increase in hip adduction ROM as compared to only ITB stretching.
References[edit | edit source]
- ↑ Arab AM, Nourbakhsh MR. The relationship between hip abductor muscle strength and iliotibial band tightness in individuals with low back pain. Chiropractic & osteopathy. 2010 Dec;18(1):1.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2821316/ (accessed on 25/07/18)
- ↑ 2.0 2.1 2.2 Kendall, McCreary, Provance; Muscle Testing and Function with Posture and Pain 4th Edition; Tensor Fascia Latae; Page No.216
- ↑ 3.0 3.1 Fairclough J, Hayashi K, Toumi H, Lyons K, Bydder G, Phillips N, Best TM, Benjamin M. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding iliotibial band syndrome. Journal of Anatomy. 2006 Mar;208(3):309-16.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2100245/ (accessed on 25/07/2018)
- ↑ Kendall, McCreary, Provance; Muscle Testing and Function with Posture and Pain 4th Edition; Fascia Latae; Page No.227
- ↑ 5.0 5.1 5.2 Kendall, McCreary, Provance; Muscle Testing and Function with Posture and Pain 4th Edition; Modified Ober Test; Page No,56-59.
- ↑ Magee D. Orthopedic Physical Assessment. 2nd ed.Pennsylvania:WB Saunders, 1992. p354-355
- ↑ Hoppenfeld S. Physical Examination of the spine and Extremeities. London: Prentice-Hall International 1976.p167
- ↑ bigesor Ober's Test Available from
- ↑ Modified Ober's Test.Available from https://youtu.be/bFVmNtuH4WU
- ↑ Knee Orthopaedic Test - A Strategic Approach to Assessing the Knee; University of Western States, College of Chiropractic, Clinic Protocol; Ober test; Page No.23; Adopted 12/12. (accessed from Knee_Orthopedic_Tests.pdf on 30/07/18)
- ↑ Reese NB, Bandy WD. Use of an inclinometer to measure flexibility of the iliotibial band using the Ober test and the modified Ober test: differences in magnitude and reliability of measurements. Journal of Orthopaedic & Sports Physical Therapy. 2003 Jun;33(6):326-30.https://www.ncbi.nlm.nih.gov/pubmed/12839207 (accessed on 28/07/2018)
- ↑ Willett GM, Keim SA, Shostrom VK, Lomneth CS. An anatomic investigation of the Ober test. The American journal of sports medicine. 2016 Mar;44(3):696-701.https://www.ncbi.nlm.nih.gov/pubmed/26755689 accessed on 28/07/2018
- ↑ Gajdosik RL, Sandler MM, Marr HL. Influence of knee positions and gender on the Ober test for length of the iliotibial band. Clinical biomechanics. 2003 Jan 1;18(1):77-9.https://www.ncbi.nlm.nih.gov/pubmed/12527250 (accessed on 28/07/2018)
- ↑ Tenney HR, Boyle KL, DeBord A. Influence of hamstring and abdominal muscle activation on a positive Ober's test in people with lumbopelvic pain. Physiotherapy Canada. 2013 Jan;65(1):4-11.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3563370/ (accessed on 28/07/18)
- ↑ Effect of Iliotibial Band stretching versus Hamstrings and Abdominal muscle activation on a positive Ober’s test in subjects with Lumbopelvic Pain: A Randomized Clinical Trial by Vijay Kage, Saitej Kolukula Naidu; July 2015 https://www.ejmanager.com/mnstemps/12/12-1435370486.pdf (accessed on 30/07/18)

