Diaphragmatic Breathing and Ventilator-Induced Diaphragmatic Dysfunction
Top Contributors - Ewa Jaraczewska, Carin Hunter, Jess Bell, Kim Jackson and Wanda van Niekerk
Introduction[edit | edit source]
Diaphragm function is vital for normal and effective respiration. Diaphragm dysfunction affects not only breathing but vocalisations and swallowing as well.[1] The physiology of the diaphragm's function affects sympathetic and parasympathetic nervous systems, motor nerve activities, the brain, postural stability, defecation, micturition, intra-abdominal pressure, metabolic balance, and cardiovascular and intraperitoneal lymphatic systems. [1] Quality of life and survival depends on diaphragmatic function. This article discusses the role of the diaphragm in detail and how mechanical ventilation affects it. It offers examples of breathing exercises and applying breathing to aid with functional activities.
Effects of Diaphragmatic Breathing[edit | edit source]
- Detoxifies and releases toxins:[2]
- The human body can release 70% of its toxins through breathing. It is recommended that diaphragmatic breathing (DB) at least 3 times per day for 39 seconds can be beneficial.
- Anti-stress:[2][3]
- When someone experiences stress, their adrenal gland releases cortisol (i.e. the "stress hormone") - the adrenal glands act in response to signals from the pituitary gland. The pituitary gland responds to signals from the hypothalamus.[4] Cortisol causes an increase in heart rate and blood pressure.
- Taking a few diaphragmatic breaths can lead to a reduction in heart rate. This allows more oxygen to enter the bloodstream, which calms the brain down (i.e. reduces anxiety, improves circulation, enhances muscular relaxation, etc).
- Deep breathing can also lead to the release of endorphins, which elevates mood.
- Relaxation and mood elevation:[2][1]
- Diaphragmatic breathing stimulates the vagus nerve, which induces relaxation (i.e. the parasympathetic nervous system is activated). NB 75% of vagal nerve fibres are parasympathetic.[2]
- Diaphragmatic breathing may lower physiological stress and psychological stress. A quantitative systematic review by Hopper et al.[5] indicated that the effect of DB on psychological stress can be measured by blood pressure, respiration and cortisol levels. The authors further concluded that "diaphragmatic breathing has the potential to offer a readily available and inexpensive treatment to help manage stress daily."[5]
- Pain relief:[2][6]
- Breathing into pain can improve circulation to that area, relieve tension and enhance oxygenation levels. This triggers the release of endorphins, which positively impacts pain levels.[6]
- Breathing disorders may directly or indirectly negatively affect motor control of all muscles surrounding the spine. It is recommended that patients with non-specific neck pain should perform diaphragmatic exercises. Diaphragmatic mobilisation and respiratory exercises improved musculoskeletal and respiratory outcomes and respiratory function.[7]
- Enhances the immune system:[2]
- Deep breathing improves an individual's ability to metabolise nutrients and vitamins. It is also beneficial for digestion, which ultimately strengthens immunity.
- Pursed-lip breathing (PLB) training, abdominal breathing training, coughing and expectoration training, and skeletal muscle training combined with general exercise training improve anxiety, depression, and other negative emotions, improve T cell immune function of the body in patients with a stable chronic obstructive pulmonary disease (COPD).[8]
- Reduces blood pressure:[6]
- Relaxation leads to the dilation of the blood vessels, which improves circulation and decreases blood pressure. Deep breathing also helps reduce/regulate heart rate, positively impacting blood pressure.
- Diaphragmatic deep breathing is based on deep and slow rhythmic breathing that increases the diaphragm contraction length, minimises the respiration frequency, and deepens the inhalation and exhalation volumes. [9] The result is a maximum amount of oxygen entering the bloodstream. Diaphragmatic deep breathing performed at 6 or ≤10 breaths per minute can lead to a decrease in systolic and diastolic blood pressure in hypertensive adults.[9]
- Improves cellular regeneration:[2]
- Deep breathing helps our bodies to be better oxygenated and improves circulation, which enhances cellular regeneration.
- Enhances posture:[2][6]
- Inspiration lengthens the spine, facilitates lumbopelvic movements, and activates core muscles. It has also been shown that it may be associated with improvements in balance.[10]
- The diaphragm and abdominals improve trunk stability due to the hydraulic effect in the abdominal cavity. The lumbar spine stiffens through increased intra-abdominal pressure. [11]
Effect of Mechanical Ventilation on the Diaphragm[edit | edit source]
- Ventilator-induced diaphragmatic dysfunction (VIDD):
- VIDD is the loss of diaphragmatic force-generating capacity. It occurs due to the use of mechanical ventilation due to the suppressed inspiratory effort.[12][13]
- Mechanical ventilatory assistance contributes to diaphragm muscle inactivity and unloading, thus leading to diaphragmatic atrophy and fatigue.[14]
- Diaphragm weakness is a leading cause of difficult weaning from mechanical ventilation[15] and loss of thickness of diaphragm muscle. However, if there is insufficient ventilatory support and the diaphragm is not unloaded adequately, this can lead to load-induced inflammation and injury.[16][17]
- Diaphragm atrophy developed during mechanical ventilation strongly impacts clinical outcomes. Targeting an inspiratory effort level similar to that of healthy subjects at rest might accelerate liberation from ventilation.[18]
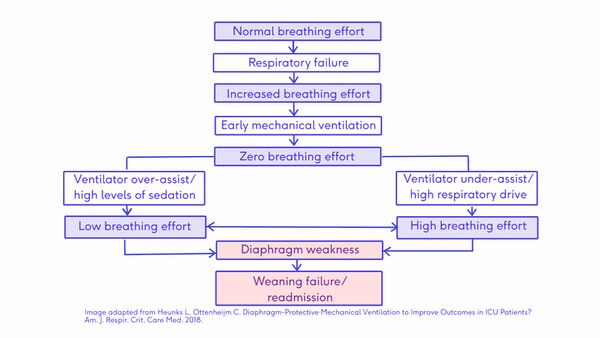 Ventilator-Induced Diaphragmatic Dysfunction Flow chart [19]
Ventilator-Induced Diaphragmatic Dysfunction Flow chart [19]

Evidence-Based Practice[edit | edit source]
- Allison et al.[20] reported that diaphragmatic activity increases in healthy subjects during lumbopelvic motion control tests.
- O’Sullivan and Beales[21] concluded in their case studies that lumbopelvic movements decrease in patients with diaphragmatic injuries.
- Moreover, patients with chronic low back pain have often been reported to have posture and motor control defects.[22][23]
- The diagram below[13] provides recommendations for clinical approaches in VIDD according to evidence-based medicine grading system (A=strong evidence, B=moderate evidence, C=weak evidence).
- Strong evidence (A)
- Favour spontaneous breathing
- Avoid medication that may be myotoxic
- Reduce sedation
- Get that patient awake and alert as much as possible to get his diaphragm to be voluntarily moving.
- Start an early mobilisation program
- Initiate inspiratory muscle training
- Moderate evidence (B)
- Daily early evaluation of the respiratory muscle strength of volitional and non-volitional diaphragmatic contraction
- Weak evidence (C)
- Apply rescue therapies: transvenous or intramuscular temporary electric diaphragmatic pacing
- Strong evidence (A)

Examples of Breathing Exercises[edit | edit source]
- Relaxation breathing:[24]
- Sit comfortably with their back straight and take a few minutes to relax.
- Put one hand on the chest and the other on the stomach.
- Inhale in through their nose.
- Focus on the feeling of the breath, the movement of the chest, rib cage, shoulders, and the expansion of the lungs.
- Exhale through their mouth, pushing out as much air as possible while contracting the abdominal muscles and moving in as they exhale.
- Continue to inhale in through their nose and out through the mouth.
- Count slowly as they exhale and stay in this relaxed state for a moment, breathing deeply and slowly
- Rhythmic breathing:[25]
- Close your eyes.
- Relax the body muscles.
- Breathe slowly and regularly and uniformly (Inhale, exhale, relax) so that you breathe in the air from your nose and then breathe out slowly through your mouth.
- Pay attention to the movement of your chest, abdomen, and shoulders while breathing.
- Regular smooth breathing:[26]
- Inhale through the nose at the rate of four numbers.
- Paused on a count of four.
- Exhaled on a count of four with the lips pursed.
- Abdominal breathing training: [8]
- Position the patient in a sitting, lying, or standing position.
- Ask the patient to relax their shoulders and upper chest.
- Place one hand in front of the chest and the other on the upper abdomen. The aim of breathing was that the hands should not feel chest undulation but rather the abdominal movement.
- During exhalation, the abdomen retracts and forces. Exhalation should be slow, and the duration of exhalation should be 1–2 times longer than that of inhalation.
- During inhalation, the abdomen bulges against the pressure of the hands. Inhalation should be deep and through the nose.
- Conduct the training for 5 min/time, gradually increasing to 10–15 min/time, 3–4 times/day.
- Pursed-lip breathing (PLB) training: [8]
- The patient is either sitting or standing.
- The patient inhales slowly and deeply through the nose.
- Next, the patient is told to hold the breath for 1–2 s, then contract the lips and slowly exhale through the mouth.
- The ratio of exhalation and inhalation time should be 2:1, 5–10 min/time, 3 times a day.
Practical Clinical Examples of Using Breath for Function[edit | edit source]
The following videos offer a practical clinical application of using breath during exercises and functional activities:
- In this video, the instructor discusses respiratory strategies. The instructor explains the "breathing goes with movement" strategy and offers examples of integrating movement with breathing.
- In this video, the instructor demonstrates the functional relationship between breathing and upper arm motion.
- In this third video, the instructor demonstrates how the transition from standing to sitting can be assisted using breathing and voicing strategies.
References[edit | edit source]
- ↑ 1.0 1.1 1.2 Hamasaki H. Effects of Diaphragmatic Breathing on Health: A Narrative Review. Medicines. 2020 Oct;7(10):65.
- ↑ 2.0 2.1 2.2 2.3 2.4 2.5 2.6 2.7 Pandya R. Diaphragmatic Breathing and Ventilator-Induced Diaphragmatic Dysfunction Course. Plus. 2022.
- ↑ Hunt MG, Rushton J, Shenberger E, Murayama S. Positive effects of diaphragmatic breathing on physiological stress reactivity in varsity athletes. Journal of Clinical Sport Psychology. 2018 Mar 1;12(1):27-38.
- ↑ Johns Hopkins Medicine. Adrenal Glands. Available from https://www.hopkinsmedicine.org/health/conditions-and-diseases/adrenal-glands (last accessed 12 February 2023).
- ↑ 5.0 5.1 Hopper SI, Murray SL, Ferrara LR, Singleton JK. Effectiveness of diaphragmatic breathing for reducing physiological and psychological stress in adults: a quantitative systematic review. JBI Database of Systematic Reviews and Implementation Reports 2019; 17(9):1855-1876.
- ↑ 6.0 6.1 6.2 6.3 Watkins A. Benefits of deep breathing [Internet]. Urban Balance. 2014 [cited 2 December 2021]. Available from: https://www.urbanbalance.com/benefits-deep-breathing/
- ↑ Tatsios PI, Grammatopoulou E, Dimitriadis Z, Papandreou M, Paraskevopoulos E, Spanos S, Karakasidou P, Koumantakis GA. The Effectiveness of Spinal, Diaphragmatic, and Specific Stabilization Exercise Manual Therapy and Respiratory-Related Interventions in Patients with Chronic Nonspecific Neck Pain: Systematic Review and Meta-Analysis. Diagnostics. 2022; 12(7):1598.
- ↑ 8.0 8.1 8.2 Ma Y, Chen Y, Zhang N, Xu G, Wang Y, Sun Y, Bai C, Zuo Z. Efficacy and safety of pulmonary rehabilitation training on lung function, quality of life, and T cell immune function in patients with stable chronic obstructive pulmonary disease: a randomized controlled trial. APM 2022;11(5).
- ↑ 9.0 9.1 Yau KK, Loke AY. Effects of diaphragmatic deep breathing exercises on prehypertensive or hypertensive adults: A literature review. Complement Ther Clin Pract. 2021 May;43:101315.
- ↑ Stephens RJ, Haas M, Moore III WL, Emmil JR, Sipress JA, Williams A. Effects of diaphragmatic breathing patterns on balance: a preliminary clinical trial. Journal of manipulative and physiological therapeutics. 2017 Mar 1;40(3):169-75.
- ↑ Foskolou A, Emmanouil A, Boudolos K, Rousanoglou E. Abdominal Breathing Effect on Postural Stability and the Respiratory Muscles’ Activation during Body Stances Used in Fitness Modalities. Biomechanics 2022; 2: 478–493.
- ↑ Kim WY, Lim CM. Ventilator-induced diaphragmatic dysfunction: diagnosis and role of pharmacological agents. Respiratory care. 2017 Nov 1;62(11):1485-91.
- ↑ 13.0 13.1 13.2 Peñuelas O, Keough E, López-Rodríguez L, Carriedo D, Gonçalves G, Barreiro E, Lorente JÁ. Ventilator-induced diaphragm dysfunction: translational mechanisms lead to therapeutical alternatives in the critically ill. Intensive care medicine experimental. 2019 Jul;7(1):1-25.
- ↑ Vassilakopoulos T, Petrof BJ. Ventilator-induced diaphragmatic dysfunction. American journal of respiratory and critical care medicine. 2004 Feb 1;169(3):336-41.
- ↑ Dres M, Dubé BP, Mayaux J, Delemazure J, Reuter D, Brochard L, Similowski T, Demoule A. Coexistence and impact of limb muscle and diaphragm weakness at the time of liberation from mechanical ventilation in medical intensive care unit patients. American journal of respiratory and critical care medicine. 2017 Jan 1;195(1):57-66.
- ↑ Orozco-Levi M, Lloreta J, Minguella J, Serrano S, Broquetas JM, Gea J. Injury of the human diaphragm associated with exertion and chronic obstructive pulmonary disease. American journal of respiratory and critical care medicine. 2001 Nov 1;164(9):1734-9.
- ↑ Goligher EC, Dres M, Patel BK, Sahetya SK, Beitler JR, Telias I et al. Lung- and diaphragm-protective ventilation. Am J Respir Crit Care Med. 2020 Oct 1;202(7):950-61.
- ↑ Lipson DA, Barnacle H, Birk R, Brealey N, Locantore N, Lomas DA, Ludwig-Sengpiel A, Mohindra R, Tabberer M, Zhu CQ, Pascoe SJ. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. American journal of respiratory and critical care medicine. 2017 Aug 15;196(4):438-46.
- ↑ Schepens T, Dres M, Heunks L, Goligher EC. Diaphragm-protective mechanical ventilation. Current opinion in critical care. 2019 Feb 1;25(1):77-85.
- ↑ Allison G, Kendle K, Roll S, Schupelius J, Scott Q, Panizza J. The role of the diaphragm during abdominal hollowing exercises. Australian Journal of Physiotherapy. 1998 Jan 1;44(2):95-102.
- ↑ O'Sullivan PB, Beales DJ. Changes in pelvic floor and diaphragm kinematics and respiratory patterns in subjects with sacroiliac joint pain following a motor learning intervention: a case series. Man Ther. 2007;12(3):209-18.
- ↑ O’Sullivan P. Diagnosis and classification of chronic low back pain disorders: maladaptive movement and motor control impairments as underlying mechanism. Manual therapy. 2005 Nov 1;10(4):242-55.
- ↑ Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic region: effect and possible mechanisms. Journal of electromyography and kinesiology. 2003 Aug 1;13(4):361-70.
- ↑ Eldin SMA, Mohamed HG, Ragab II. Effect of Relaxation Breathing Technique among Patients with Moderate Burn on their Pain and Anxiety at Wound Care. World Journal of Nursing Sciences 2015; 1(3): 110-123.
- ↑ Bozorg-Nejad M, Azizkhani H, Mohaddes Ardebili F, Mousavi SK, Manafi F, Hosseini AF. The Effect of Rhythmic Breathing on Pain of Dressing Change in Patients with Burns Referred to Ayatollah Mousavi Hospital. World J Plast Surg. 2018 Jan;7(1):51-57.
- ↑ Hoseinzadeh-Karimkoshteh M, Firouzkouhi M, Abdollahimohammad A. Effect of regular smooth breathing on the intensity of pain caused by dressing change in patients with second-degree burns: a clinical trial. Med Surg Nurs J. 2019; 8(2):e92321.
- ↑ Ventilatory Strategies -- Massery PT -- Mary Massery -- If You Can't Breathe, You Can't Function. Available from: https://www.youtube.com/watch?v=bp1BYblDmOA[last accessed 5 November 2023]
- ↑ Functional Relationships -- Massery PT -- Mary Massery -- If You Can't Breathe, You Can't Function. Available from: https://www.youtube.com/watch?v=R2Ox9zkcj68 [last accessed 5 November 2023]
- ↑ Using Voicing Strategies -- Massery PT -- Mary Massery -- If You Can't Breathe, You Can't Function. Available from: https://www.youtube.com/watch?v=c_VlBI-QgOw [last accessed 5 November 2023]

