Developmental Coordination Disorder and Physical Activity
Original Editor Irene Leahy
Top Contributors - Stacy Zousmer, Irene Leahy, Kim Jackson, Admin, Adam Vallely Farrell, 127.0.0.1 and Michelle Lee
What is Developmental Coordination Disorder?[edit | edit source]
Developmental coordination disorder (DCD) is a diagnosis given to children who have marked impairment in motor coordination that significantly impacts on their academic achievement and activities of daily living and is not due to any known medical or mental condition as stated in the DSM-IV-TR [1].
Children may meet the diagnosis of DCD if they present with some of the following;
- Performance in daily activities that require motor coordination is substantially below that expected, given the person’s chronological age and measured intelligence. This may be manifested by:
- Marked delays in achieving motor milestones (e.g., walking, crawling, sitting)
- Dropping things
- Clumsiness
- Poor performance in sports
- Poor handwriting
- When the disturbance significantly interferes with academic achievement or ADLs
- When the disturbance is not due to a general medical condition (e.g. cerebral palsy, hemiplegia, or muscular dystrophy) and does not meet criteria for a Pervasive Developmental Disorder
- If a learning disability is present, but the motor difficulties are in excess of those that are usually associated with it[2]
For a diagnosis of DCD to be made it is important a paediatrician/neurologist referral is made to; rule out underlying neurological or physical disorders (peripheral neuromuscular conditions, central neuromuscular conditions, mixed peripheral and central nervous system conditions), determine child has significant coordination difficulties compatible with DCD, refer to OT/Physiotherapy as required. [2]
DCD should not be confused with dyspraxia in which there is no formal diagnostic criteria and is not recognised by many paediatricians and school authorities as a diagnosis.
Prevalence[edit | edit source]
Developmental coordination disorder is identified as a common disorder of childhood and is usually identified in children between 6 and 12 years of age. In the 1990s researchers estimated that DCD occurred in 10% to 19% of school-aged children.[3] Following a more precise diagnostic criteria and definition, the current prevalence is estimated to be 5%- 8% of all school-aged children.[4] It is more prevalent in boys than in girls (2:1).[5] This difference is often associated with a higher referral rate for boys, because the behaviour of boys with motor incoordination may be more difficult to manage at home and in the classroom.
Causes[edit | edit source]
Motor control processes depend on the integrated functioning of the sensory, perceptual, cognitive and motor systems. Due to this, it is difficult to determine the location and nature of this neural deficiency.[6] Current evidence reports a significantly higher risk in premature and/low birth weight children, those with delayed walking after 15 months and abnormalities in neurotransmission. [7]
Characteristics of DCD[edit | edit source]
| Gross Motor | Fine Motor | Perceptual/Sensory | Psychosocial |
|---|---|---|---|
| Hypotonia | Handwriting | Poor awareness of body position in space | Learning disabilities |
| Immature balance reactions | Drawing | Poor sense of direction | Reading problems |
| Awkward running patterns | Confused about which hand to use | Sensitive to touch | Speech problems |
| Poor posture | Gripping | Find some fabrics uncomfortable | Class clown |
| Frequent falls | Dressing | Few friends | |
| Dropping items | Buttons | Lower self-esteem | |
| Difficulty imitating body positions | Zipping | Increased anxiety | |
| Difficulty following 2-3 stage motor commands | Shoelaces | ||
| Reduced ability to throw/catch ball | |||
| Difficulty hopping, skipping, riding a bike | |||
| Slow to dress |
Measurement of DCD[edit | edit source]
There is currently no gold standard for the measurement of DCD. Common outcome measures that can be used by a physiotherapist to measure its severity and impact include;
- Developmental Coordination Disorder Questionnaire (DCD-Q)
- Movement Assessment Battery for Children (M-ABC) most widely used
- Bruininks-Oseretsky Test of Motor Proficiency (BOTMP)
- BOT-SF (Short Form)
Why is Participation in Physical Activity Important? 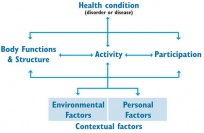 [edit | edit source]
[edit | edit source]

The international classification of function, disability and health considers activity and participation limitation due to disability important [10](WHO 2001). Research in the participation of children with DCD has shown decreased physical activity (PA) and fitness [11]. This has a negative impact on physical health [11], mental health and social development [12].
Outcome Measures[edit | edit source]
Studies of PA use subjective methods such as questionnaires and diaries or objective measures such as accelerometers. Objective measures are more reliable but only measure frequency and intensity of activity [13]. Subjective methods are less reliable and error in reporting occurs [14]. However, they can address numerous aspects of PA participation such as diversity, intensity, frequency, enjoyment and whether they participate in group activities or choose solitary activities [15]. There is a bias toward parent and teacher-reported PA participation in children with DCD in the literature [16]. It is important to consider children's perspectives and priorities as they do not mirror that reported by adults [17][18]. Therefore, research of children with DCD should examine their unique perspective so that research is of children rather than about them [19].
Elements of PA in children with DCD that were considered are frequency, intensity and diversity of participation.
Frequency of Participation in PA[edit | edit source]
Frequency of participation in PA is reduced in this population of children. Children with DCD between the age of 9 and 14 years report lower frequency of participation in free-and organised-play [20]. [21]Fong et al (2011) and [15]Jarus et al (2011) agreed with this finding for children aged between 6 and 12 years and 5 and 7 years, respectively. [20]Cairney et al (2005,2005a,2006) and [15]Jarus et al (2011) used a small sample of children that was not randomly selected. [21]Fong et al (2011) had a larger sample based on statistical power calculations. This was the only study to calculate sample size based on statistical power but the sample was still a convenience sample. Therefore there is a risk of selection bias in these studies. While [15]Jarus et al (2011) and [21]Fong et al (2011) had a sample of children with DCD diagnosis those included in [20]Cairney et al (2005,2005a,2006) had no formal diagnosis. Only one other study used a sample of children with a formal diagnosis of DCD [22]. No studies blinded the assessors which may lead to detection bias. Frequency of PA participation was consistently reduced in all studies of children with DCD.
Intensity of Participation in PA[edit | edit source]
[23]Poulsen et al (2008,2008a) reported adolescent boys with DCD spent decreased time in high-intensity PA and had a preference for low-intensity PA compared to boys without DCD. This was estimated from a one-week diary log of PA which has a high risk of reporting error as it relies on recall abilities of participants [24](Anderson et al 2005). [15]Jarus et al (2011) and [21]Fong et al (2011) included both genders and reported decreased intensity of PA in children with DCD. These results are more reliable as it was calculated using the Child Assessment of Participation and Enjoyment (CAPE) questionnaire (King et al 2007)[25]. Both studies matched controls and participants for age, gender and socio-economic class but like the other studies in this review they did not account for other confounding variables such as birth weight, gestational age or maternal PA levels during pregnancy in the statistical analyses which have been shown to influence PA in childhood [26](Mattocks et al 2008). Therefore differences in PA may be due to factors other than DCD.
Diversity of Participation in PA[edit | edit source]
Fong et al (2011)[21] reported that children aged 6-12 years participate in a smaller variety of activities. Analysis of results shows that participation is less in informal, physical, social, skill-based and self-improvement activities than their peers without DCD. However, participation in formal and recreational activities did not differ between groups. The majority of recreational activities in the CAPE questionnaire are sedentary and do not require motor coordination. Jarus et al (2011)[15] also used the CAPE questionnaire and found that children aged 5-7 years with DCD engage in less physical, skill-based and informal activities. In contrast no statistical significant difference in social and self-improvement activities was found. This may be due to the small sample size as mentioned before. Poulsen et al (2008,2008a) [23]measured diversity of activities in boys with DCD over a week. This may not be accurate due to the short time span. The CAPE questionnaire used by the previous studies considers the diversity of participation over the previous 4 months. Taking this into account, results once again show that boys with DCD participated in less diverse activities and the majority of time was spent in sedentary activities. Participation in team sports and unstructured social physical activities were significantly lower than their peers without DCD. Unstructured social PA included streetball games or running games. Interestingly, there was no difference between groups in individual sports. This may be due to these activities not requiring the evaluative skills needed for team sports[23]. It is clear from the available literature; diversity of PA is narrower in children with DCD.
Effect of Age on Participation Patterns[edit | edit source]
Suggestions are made that the activity-deficit in children with DCD would increase with age[27]. This was not seen in children between the age of 9 and 14 years in free- and organised-play [20]. Appropriate ANCOVA tests were used to analyse this difference but results should be interpreted with caution as this study was cross-sectional. More accurate results would be obtained from a longitudinal study following the same group of children rather than comparing results from different individuals at different ages. The only longitudinal study in this review used mixed-effects modelling analysis which showed a difference over a 3 year period[20]. Boys showed an increase in the frequency of PA while girls exhibited a consistent decrease. The increasing expectations and complexity of PA in adolescence were cited as a difficulty[28]. The sample used in this qualitative study was a group of university students which is not representative of the wider heterogeneous population of children with DCD. However, it is important to consider qualitative research as it gives a deeper meaning to the reduced participation in this population.
Effect of Gender on Participation[edit | edit source]
There are less societal expectations for females to be physically active ([29]. Therefore it is suggested that girls with DCD will be less active than boys with DCD. Cairney et al (2005) found that there was no statistical difference in PA frequency between genders. Despite this, there is a trend towards lower participation in free-and organized-play in girls but it does not reach statistical significance which may be due to the smaller sample size. Cairney et al (2009)[20] used a larger sample size and showed that there was increased frequency of PA in boys with DCD compared with girls as they got older. It is important to remember that both these studies used Participation Questionnaire (PQ) which only accounts for organised- and free-play and not other forms of PA such as chores and active transport. Additionally, Engel-Yeger and Hanna Kasis (2010)[30] showed there were differences between genders in preference for certain activities. Girls with DCD favoured skill-based activities whereas boys favoured active PA which was similar to their peers without DCD. This study unlike the others included parent education as well as age and gender as confounding factors in analysis. A limitation of this study is the use of Preference for Activities of Children (PAC) as it just measures preference and gives no indication of whether these activities are performed. Therefore, it does not indicate actual participation patterns.
Effect of Motor Ability on Participation[edit | edit source]
Limited studies considered the effect of motor ability on participation. Motor ability was shown to positively correlate to PA [15]. (2011)[21] used multiple regression analysis and concluded that after motor ability was added to regression with age and gender it accounted for 7.6% of the variance in PA diversity. In contrast, Jarus et al (2011)[15] only used Pearson’s correlation coefficient to analyse this relationship so it only considers two factors in isolation. Preference to participate in active PA was also positively correlated with motor ability[15]. These findings suggest that children with higher motor ability have an increased ability to activate and sequence motor movements which provides more opportunities for participation [31]. However, it is important to remember the cross-sectional design of these studies making it impossible to demonstrate causal pathways for the relationship between these factors.
Effect of Reduced Participation on Social Development[edit | edit source]
Reduced PA may have a detrimental effect on social development[12]. A greater number of children with DCD play alone during out of school activities compared to their peers (Jarus et al 2011)[15]. This was reiterated in qualitative studies where individual activities were preferred as they avoid ridicule and pressure from peers [28], [32]. Fong et al (2011)[21] concluded that a large number of children in their sample with and without DCD participated in activities with family with no difference between groups. This may be due to cultural influence and a higher emphasis on family in this Asian sample [33]. Boys with DCD had a lower perception of their social competence which had a negative impact on the intensity of participation[23]. Poulsen et al (2008a)[23] found that motor ability affected loneliness negatively and life satisfaction positively in the same group of boys. They discovered that team sport participation increased life satisfaction and decreased loneliness which is probably due to the social nature of these sports. However, there may be other factors that were not taken into consideration in this study such as social-environmental influences because only partial mediation effects were demonstrated. All the participants were from a high socio-economic background and were male which may place social value on participation in sport which affects the ability to generalise results. Additionally, there are no other studies that investigated these aspects so it is difficult to draw conclusions from these results.
Effect of Reduced Participation on Self-Efficacy Towards PA[edit | edit source]
Cairney et al (2005, 2005a)[20] and Engel-Yeger and Hanna Kasis (2010)[30] concluded that self-efficacy in children with DCD was significantly lower compared to their peers. However, Cairney et al (2005,2005a)[20] had a low response rate to the PQ which may affect results as there is no data on non-participants. Another limitation of these studies is that the outcome measures used do not measure efficacy in activities outside of school. Children’s Self-perception of Adequacy in and Predilection for Physical Activity (CSAPPA) measures self-efficacy in physical education class [20]and the Perceived Efficacy and Goal Setting System (PEGS) include school and self-care activities as well as leisure activities [30]. Therefore, it is difficult to draw a conclusion about self-efficacy in activities outside of school.
Enjoyment of PA and Participation[edit | edit source]
Studies investigating enjoyment of PA report no difference between children with and without DCD [15], [21]. This may be due to children choosing to participate in activities that they enjoyed (Jarus et al 2011)[15]. These children had not reached adolescence which may affect these results as younger children do not compare themselves to peers and are less frustrated by their inability to perform[34]. Missiuna et al (2008)[28] highlighted that adolescents also chose activities that they were good at and enjoyed. Additionally, Fitzpatrick and Watkinson (2003)[32] reported avoidance of activities that caused humiliation. It was exposure of their awkwardness that decreased enjoyment of activities rather than the lack of coordination itself. This study like Missuina et al (2008)[28] used a phenomenological approach and considered the retrospective viewpoint of adults through interview. Thematic analysis was detailed adequately using member checking for verification of accuracy. Neither study considered the author's role and the bias that this may cause in the data. Participants were not diagnosed with DCD but had significant coordination difficulties that affected daily activities. These studies relied on the recall ability of adults rather than interviewing children. Both studies had flaws but they provide information regarding the selection of enjoyable activities and further qualitative research is needed of children with DCD. Available research shows that children with DCD select activities outside of school that they can enjoy.
References[edit | edit source]
- ↑ American Psychiatric Association (2000) Diagnostic and Statistical Manual of Mental Disorders:DSM-IV-TR, 4th ed., Washington D.C.: American Psychiatric Association
- ↑ 2.0 2.1 American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th edn, text revision. Washington, DC: American Psychiatric Association, 2000.
- ↑ Barnhart R, Davenport M, Epps S, Nordquist V. Developmental coordination disorder. Physical Therapy Aug 2003; 83(8); 722-731.
- ↑ Smyth TR. Impaired motor skill (clumsiness) in otherwise normal children: a review. Child Care, Health, and Development. 1992;18:283–300.
- ↑ Gordon N, McKinlay I. Helping clumsy children. Edinburgh: Churchill Livingstone, 1980.
- ↑ Edwards J, Berube M, Erlandson K, Haug S, Johnstone H, Meagher, M, Sarkodee-Adoo S, Zwicker, J. Developmental Coordination Disorder in school-aged children born very preterm and/or at very low birth weight: A systematic review. Journal of Developmental and Behavioral Pediatrics Nov/Dec 2011; 32(9):678-687.
- ↑ Faebo Larsen R, Hvas Mortensen L, Martinussen Torben, Nybo Andersen A. determinants of developmental coordination disorder in 7-year old children: a study of children in the Danish National Birth Cohort. Developmental Medicine & Child Neurology 2013;55(11);1016-1022.
- ↑ Dewey D, Wilson BN. Developmental coordination disorder: what is it? Physical and Occupational Therapy in Pediatrics. 2001;20:5–27.
- ↑ Skinner RA, Piek JP. Psychosocial implications of poor motor coordination in children and adolescents. Hum Mov Sci. 2001;20(1–2): 73–94.
- ↑ World Health Organisation (2001) International classification of functioning, disability and health, available: http://www.who.int/classifications/icf/en/ [accessed 1 April 2012]
- ↑ 11.0 11.1 Rivilis, I., Hay, J., Cairney, J., Klentrous, P., Liu, J. and Faught, B.E. (2011) ‘Physical activity and fitness in children with developmental coordination disorder: A systematic review’, Research in developmental Disabilities, 32(3), 894-910, available: ScienceDirect [accessed 8 Mar 2012]
- ↑ 12.0 12.1 Hands, B. and Larkin, D. (2002) ‘Physical fitness and developmental coordination disorder’, in Cermack, S.A. and Larkin, D., eds., Developmental Coordination Disorder, New York: Delmar Thomson Learning, 172-185
- ↑ Green, D., Lingam, R., Mattocks, C., Riddoch, C., Ness, A. and Emond, A. (2011) ‘The risk of reduced physical activity in children with probable developmental coordination disorder: a prospective longitudinal study’, Research in developmental disabilities, 32(4), 1332-1342, available: ScienceDirect [accessed 5 Mar 2012]
- ↑ Dockrell, J., Lewis, A. and Lindsay, G. (2000) ‘Researching children’s perspectives: a psychological dimension’, in Lewis, A. and Lindsay, G., eds., Researching Children’s Perspectives, Philadelphia: Open University Press, 46-58
- ↑ 15.00 15.01 15.02 15.03 15.04 15.05 15.06 15.07 15.08 15.09 15.10 15.11 Jarus, T., Lourie-Gelberg, Y., Engel-Yeger, B. and Bart, O. (2011) ‘Participation patterns in school-aged children with and without DCD’, Research in developmental disabilities, 32(4), 1323-1331, available: ScienceDirect [accessed 20 Mar 2012]
- ↑ Magalhaes, L.C., Cardoso, A.A. and Missiuna, C. (2011) ‘Activities and participation in children with developmental coordination disorder: A systematic review’, Research in developmental disabilities,32(4), 1309-1316, available: ScienceDirect [accessed 8 Mar 2011]
- ↑ Lloyd-Smith, M. and Tarr, J. (2000) ‘Researching children’s perspectives: a sociological dimension’, in Lewis, A. and Lindsay, G., eds., Researching Children’s Perspectives, Philadelphia: Open University Press, 59-70
- ↑ Pollock, N. and Stewart, D. (1998) ‘Occupational performance needs of school-aged children with physical disabilities in the community’, Physical and occupational therapy in pediatrics, 18(1), 55-68, available: Informa Healthcare [accessed 20 Mar 2012]
- ↑ Winn-Oakley, M. (2000) ‘Children and young people and care proceedings’, in Lewis, A. and Lindsay, G., eds., Researching children’s perspectives, Philadelphia: Open University Press, 73-85
- ↑ 20.0 20.1 20.2 20.3 20.4 20.5 20.6 20.7 20.8 Cairney, J., Hay, J.A., Faught, B.E., Wade, T.J., Corna, L. and Flours, A. (2005a) ‘Developmental coordination disorder, generalized self-efficacy toward physical activity, and participation in organized and free play activities’, The journal of paediatrics, 147(4), 515-520, available: ScienceDirect [accessed 6 Mar 2012]
- ↑ 21.0 21.1 21.2 21.3 21.4 21.5 21.6 21.7 Fong, S.S.M., Lee, V.Y.L., Chan, N.N.C., Chan, R.S.H., Chak, W. and Pang, M.Y.C. (2011) ‘Motor ability and weight status are determinants of out-of-school activity participation for children with developmental coordination disorder’, Research in developmental disabilities,32(6), available: ScienceDirect [accessed 5 Mar 2012]
- ↑ Engel-Yeger, B. and Hanna Kasis (2010) ‘The relationship between developmental coordination disorder, child’s perceived self-efficacy and preference to participate in daily activities’, Child: Care, Health and Development, 36(5), 670-677, available: Wiley Online Library [accessed 5 Mar 2012]
- ↑ 23.0 23.1 23.2 23.3 23.4 Poulsen, A.A., Ziviani, J.M., Johnson, H. and Cuskelly, M. (2008a) ‘Loneliness and life satisfaction of boys with developmental coordination disorder: the impact of leisure participation and perceived freedom in leisure’, Human movement science, 27(2), 325-343, available: ScienceDirect [accessed 6 Mar 2012]
- ↑ Anderson, C.P., Hagstromer, M. and Yngve, A. (2005) ‘Validation of the PDPAR as an adolescent diary: Effect of accelerometer cut points’, Medicine and science in sports and exercise, 37(7), 1224-1230, available: OvidSP [accessed 6 Mar 2012]
- ↑ King, G., Law, M., King, S., Hurley, P., Hanna, S., Kertoy, M. and Rosenbaum, P. (2007) ‘Measuring children’s participation in recreational and leisure activities: construct validation of the CAPE and PAC’, Child: Care, Health and Development, 33(1), 28-39, available: CINAHL
- ↑ Mattocks, C., Ness, A., Deere, K., Leary, S., Tilling, K., Blair, S.N. and Riddoch, C. (2008) ‘Early determinants of physical activity in 11 to 12 year olds: cohort study’, British Medical Journal, 336(7634), 26-29, available: JSTOR
- ↑ Wall, A.E. (2004) ‘The development of skill learning gap hypothesis: implications for children with movement difficulties’, Adapted physical activity quarterly, 21(3), 197-218, available: SPORTDiscus
- ↑ 28.0 28.1 28.2 28.3 Missiuna, C., Moll, S., King, G., Stewart, D. and MacDonald, K. (2008) ‘Life experiences of young adults who have coordination difficulties’, Canadian Journal of Occupational Therapy, 75(3), 157-166
- ↑ Chase, M.A. and Dummer, G.M. (1992) ‘The role of sports as a social status determinant for children’, Research quarterly for exercise and sport, 63(4), 418-424
- ↑ 30.0 30.1 30.2 Engel-Yeger, B. and Hanna Kasis (2010) ‘The relationship between developmental coordination disorder, child’s perceived self-efficacy and preference to participate in daily activities’, Child: Care, Health and Development, 36(5), 670-677, available: Wiley Online Library
- ↑ Wrotniak, B.H., Epstein, L.H., Dorn, J.M., Jones, K.E. and Kondilis, V.A. (2006) ‘The relationship between motor proficiency and physical activity in children’, Pediatrics, 118, (6), 1758-1765
- ↑ 32.0 32.1 Fitzpatrick, D.A. and Watkinson, E.J. (2003) ‘The lived experience of physical awkwardness: adults’ retrospective views’, Adapted physical activity quarterly, 20(3), 279-297, available: SPORTDiscus [accessed 6 Mar 2012]
- ↑ Kim, S.Y. and Wong, V.Y. (2002) ‘Assessing Asian and Asian American parenting: A review of the literature’, in Kurasaki, K., Okazaki, S. and Sue, S., eds., Asian American mental health: Assessment methods and theory, Netherlands; Kluwer Academic Publishers, 185-203
- ↑ Harter, S. and Pike, R. (1984) ‘The pictorial scales of perceived competence and social acceptance for young children’, Child development, 55(6), 1969-1982, available:

